Article Text

Abstract
Objective The COVID-19 pandemic emphasises the need to use healthcare resources efficient and effective to guarantee access to high-quality healthcare in an affordable manner. Surgical cancellations have a negative impact on these. We used the Lean Six Sigma (LSS) methodology to reduce cardiac surgical cancellations in a University Medical Center in the Netherlands, where approximately 20% of cardiac surgeries were being cancelled.
Method A multifunctional project team used the data-driven LSS process improvement methodology and followed the ‘DMAIC’ improvement cycle (Define, Measure, Analyse, Improve, Control). Through all DMAIC phases, real-world data from the hospital information system supported the team during biweekly problem-solving sessions. This quality improvement study used an ‘interrupted time series’ study design. Data were collected between January 2014 and December 2016, covering 20 months prior and 16 months after implementation. Outcomes were number of last-minute coronary artery bypass graft cancellations, number of repeated diagnostics, referral to treatment time and patient satisfaction. Statistical process control charts visualised the change and impact over time. Students two-sample t-test was used to test statistical significance. A p<0.05 was considered as statistically significant.
Results Last-minute cancellations were reduced by 50% (p=0.010), repeated preoperative diagnostics (X-ray) declined by 67% (p=0.021), referral to treatment time reduced by 35% (p=0.000) and patient Net Promoter Score increased by 14% (p=0.005).
Conclusion This study shows that LSS is an effective quality improvement approach to help healthcare organisations to deliver more safe, timely, effective, efficient, equitable and patient-centred care. Crucial success factors were the use of a structured data-driven problem-solving approach, focus on patient value and process flow, leadership support and engagement of involved healthcare professionals through the entire care pathway. Ongoing monitoring of key performance indicators is helpful in engaging the organisation to maintain continuous process improvement and sustaining long-term impact.
- quality improvement
- lean management
- six sigma
- root cause analysis
- surgery
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Healthcare systems are confronted with increasing healthcare expenditure and ageing populations.1 This requires improvement of organisation efficiency and increased focus on value adding healthcare for patients. The recent COVID-19 outbreak reinforces the fundamental need for more efficient use of scarce hospital resources to keep healthcare systems sustainable.2 3
Coronary artery disease is the leading cause of mortality worldwide.4 5 Treatment is organised in different care pathways depending on disease progression, with coronary artery bypass graft (CABG) being one of the final treatment options.6 CABG is the most frequently performed procedure within cardiac surgery, representing annual volumes of approximately 200 000 isolated cases in the USA and an average incidence rate of 62 per 100 000 inhabitants in western European countries.7–9
Cardiac surgery has a high impact on patients and hospital resources. To make efficient use of hospital resources such as the operating room (OR) and intensive care unit (ICU), an aligned planning process across the full care pathway is essential. However, last-minute surgical cancellations occur frequently and have a significant impact on hospital resources, costs and quality of care.10 11 Prolonged waiting times and delays in treatment for CABG increase the risk of adverse events.12 13 The aim of reducing surgical cancellations is consistent with the influential framework created by the Institute of Medicine for addressing quality improvement in healthcare, covering six domains: safe, timely, effective, efficient, equitable and patient-centred care (STEEEP).14
Maastricht University Medical Center (MUMC+), a Dutch academic hospital with 5500 employees, 715 beds and 26 ORs, was confronted with approximately 20% last-minute cancellations of planned CABG-procedures in 2014. Besides the significant negative impact on hospital revenue, with a reimbursement of approximately €12 000 per case, the cancellations resulted in lower OR utilisation, prolonged referral to treatment time (RTT), administrative burden of rescheduling operations, repeating of diagnostics, extended length of stay (LOS) and suboptimal patient and staff satisfaction. Furthermore, a decline in production would potentially set the hospital’s license to perform certain cardiac surgery at risk.
Under the umbrella of a hospital-wide operational excellence deployment, the department of cardiothoracic surgery initiated a quality improvement project to reduce the number of CABG cancellations.15 Lean Six Sigma (LSS) is a structured quality improvement methodology that helps organisations to reduce waste and improve flow. It has been effectively applied to healthcare to sustain accessibility, affordability and quality.16–21 The aim of this project was to apply LSS to increase the amount of CABG procedures by reducing the number of last-minute cancellations with 50%.
Methods
This is an ‘interrupted time series’ quality improvement study according to the Standards for Quality Improvement Reporting Excellence Guidelines 2.0.22 All scheduled CABG surgeries in the MUMC+ between January 2014 and December 2016 were included in this study, covering 20 months prior to full implementation of the changes and 16 months after.
Outcomes
Primary endpoint was the percentage of cancellations 24 hours prior to CABG surgery per month.
Secondary endpoints were RTT (in days), number of patients with repeated preoperative diagnostics per month (X-ray) and patient satisfaction.
Data collection and analysis
The surgical planning team registered the number of surgeries and reasons for cancellations in the hospital information system. Data regarding RTT and number of patients with repeated diagnostics were automatically generated in the hospital information system. It was extracted from the hospital system and collected in a separate database. Analysis was performed by using Minitab Statistical Software V.18.1, typically used for LSS projects.
Patient satisfaction was measured by a phone interview with the patient 30 days after discharge from the hospital and presented in the Net Promoter Score (NPS). NPS was based on scores of 0–10, calculated by subtracting the percentage of detractors by the percentage of promoters. Patients were considered promoters (score 9 and 10), passives (7 and 8) and detractors (0 till 6). Statistical difference was tested with Student’s t-test for two samples. Descriptive statistics are shown as 95% CIs. A p<0.05 is considered significant.
Lean Six Sigma
The project applied the LSS quality improvement methodology.23 24 The project started with shaping a multifunctional team, consisting of the department head of cardiothoracic surgery, an outpatient–clinic staff member, an OR schedular, the head nurse, a team leader of the ICU, a business intelligence representative and a staff cardiothoracic surgeon. The team participated in a training to understand the five principles of Lean (define value, map the value stream, create flow, establish pull and pursuit perfection) and Lean tools.25 Supported by an LSS master black belt, the project followed the Define, Measure, Analyse, Improve, Control (DMAIC) improvement cycle: ‘Define’ to identify and scope the challenge, ‘Measure’ to understand and map the baseline capability, ‘Analyse’ to identify the root cause of problems (Value Stream Mapping (VSM), Pareto Analysis and ‘5× Why’), ‘Improve’ to design the new normal and change the way of working based on prioritised countermeasures and ‘Control’ to sustain the gain and measure final capability. Through all phases, real-world data from the hospital information system supported biweekly problem-solving sessions.
Work floor visits (Gemba Walks) helped the project team to better understand how value was created and learn about perceived bottlenecks.25
Value stream mapping
VSM is an important tool of LSS to understand the process of value creation from referral to discharge.26 The CABG care pathway consists of the following steps: (1) referral, (2) multidisciplinary heart team meeting to identify the right patient for the right treatment, (3) preoperative visit to perform necessary diagnostics, inform the patient and establish final decision for surgery, (4) admission to the ward to prepare the patient preoperatively, (5) surgery, and subsequently (6) ICU, (7) MCU, (8) ward to recover and (9) discharge.
The project team identified 60 bottlenecks, which hindered patient flow and potentially lead to last-minute cancellations. Most important bottlenecks were used for a more in-depth root cause analysis (5× Why).
Pareto analysis
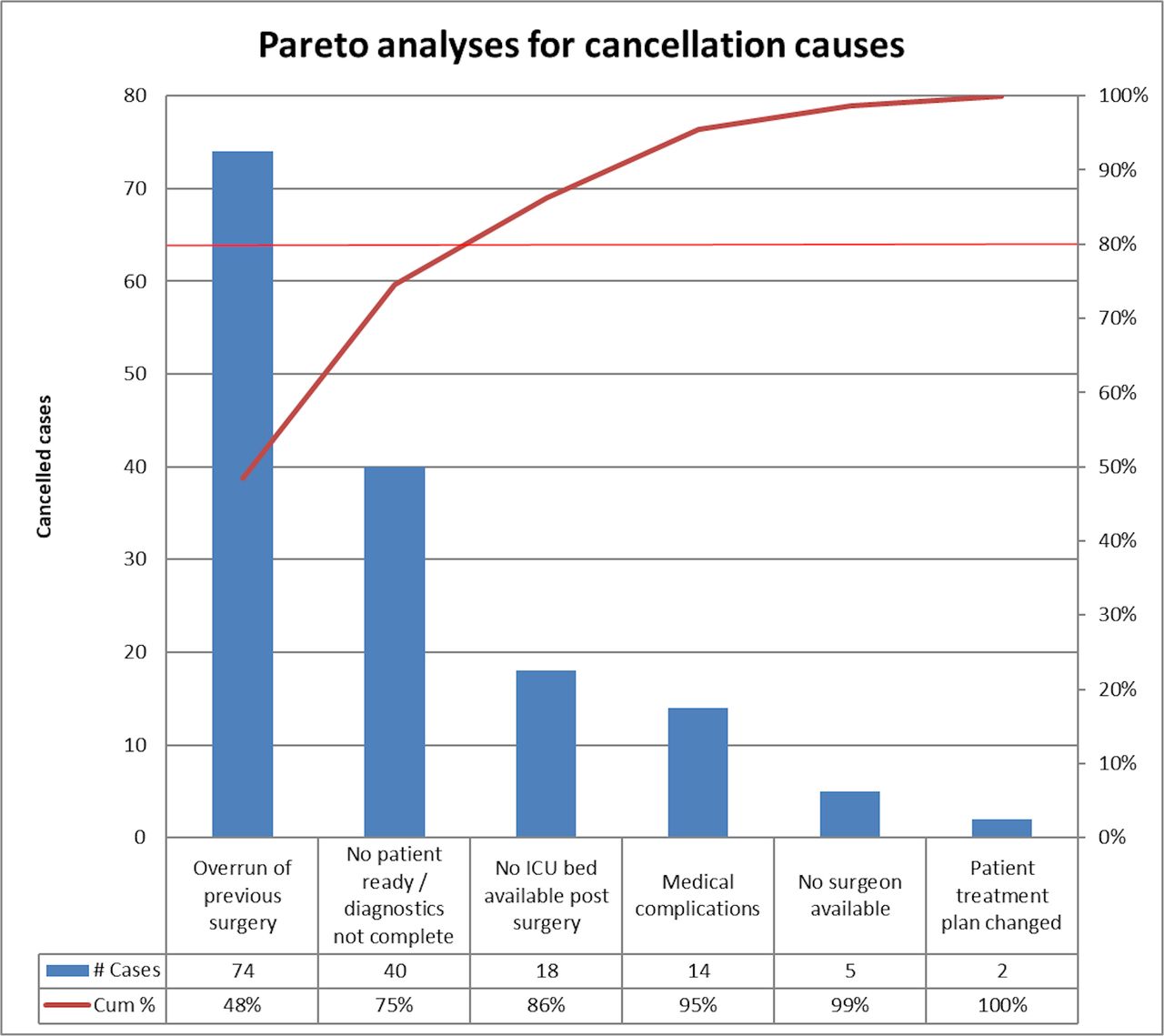
Pareto analysis of the CABG cancellations presents a hierarchy of the most frequent causes of cancellations (figure 1). Forty-eight per cent of cancellations (n=74) were caused by overrun of previous surgery, in 27% of the cases (n=40) patients were incompletely prepared for surgery, 11% (n=18) was caused by unavailability of ICU beds, 9% (n=14) by medical complications, cardiac surgeons not available (4%, n=5) and last-minute change of treatment plan (1%, n=2).

Pareto chart for cancellations. ICU, intensive care unit.
Root cause analysis
The most important VSM bottlenecks and Pareto analysis were input for ‘5× Why root causes analysis’ (figure 2). This methodology is used to understand causes of cancellations more thoroughly. Analysis showed that causes of cancellations were present during all phases of the CABG care pathway:
Preoperative: incomplete preparation of the patient prior to surgery, due to suboptimal documentation, absence of crucial information by referrer, overfull heart team meeting agenda and expired diagnostic tests.
Perioperative: unavailability of an OR because of an overrun of previous surgery. This was caused by inaccurate planning (not tailored to patient characteristics, complexity of procedure and/or staff experience) or late starts (patient, staff or materials arrived late).
Postoperative: bottlenecks in postoperative flow from ICU to MCU and/or ward, caused by inability to discharge patients to the referring centre, rehabilitation clinic, nursing home or directly back home.
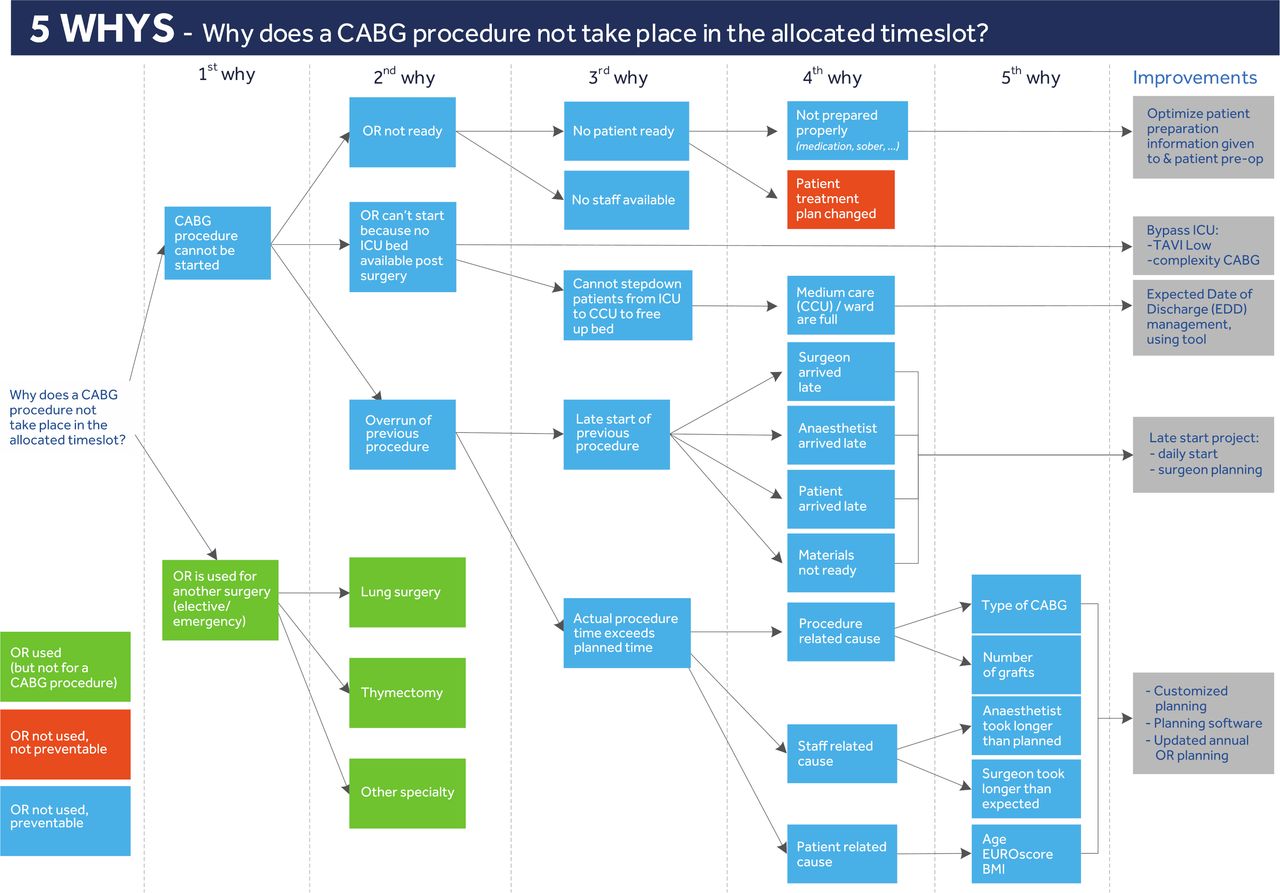
Root cause analysis. BMI, body mass index; CABG, coronary artery bypass graft; ICU, intensive care unit; OR, operating room; CCU, cardiac care unit; TAVI, Transcatheter Aortic Valve Implantation.
Improvements
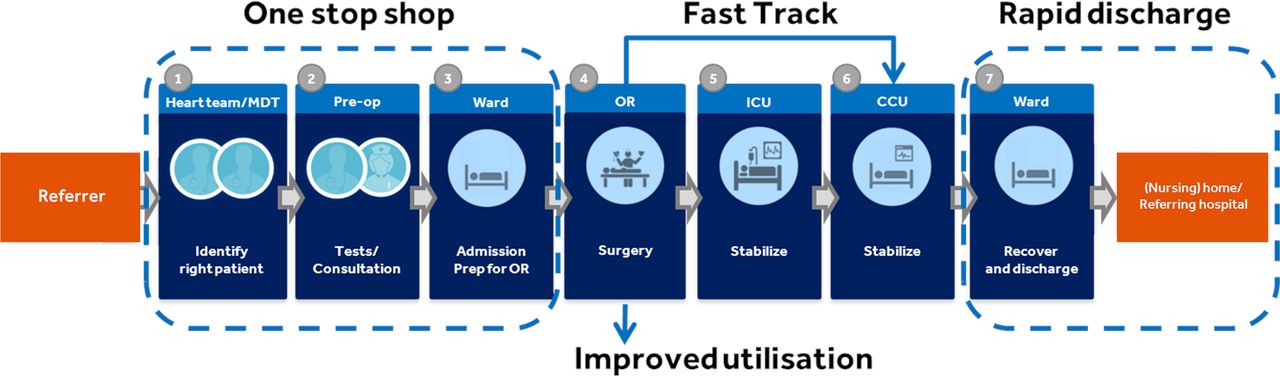
Guided by the third and fourth principle of Lean, ‘create flow’ and ‘establish pull’, the project team identified, prioritised and implemented countermeasures for the root causes of the problems. A summary of improvements to optimise patient flow per process phase is presented in figure 3.
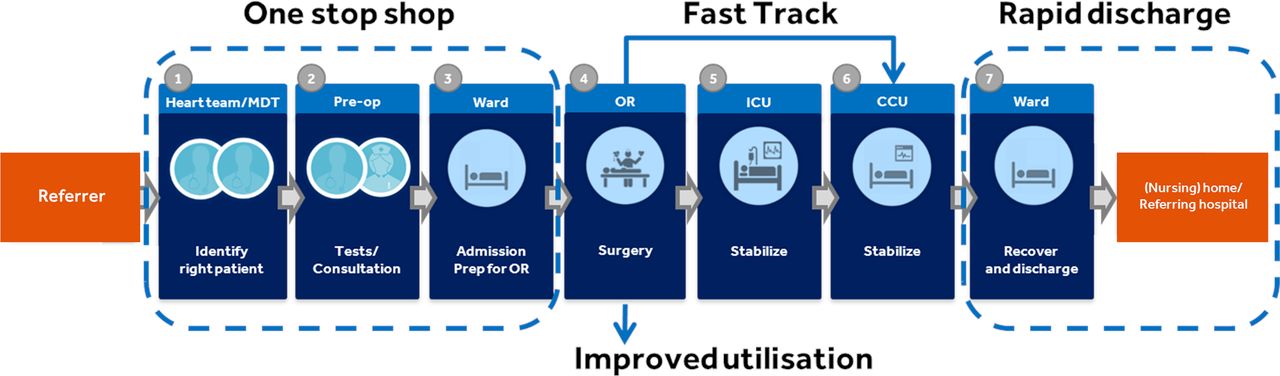
Process map with high-level improvements. MDT, Multidisciplinary Team Meeting; OR, Operating Room; ICU, Intensive Care Unit; CCU, Cardiac Care Unit.
Preoperative phase
Optimising preparation heart team meeting
During heart team meetings, cardiac surgeons and cardiologists discuss all referred patients that are eligible for surgery and decide on treatment plan and priority. Incomplete patient information frequently led to delays in decision making. To tackle this, a checklist for administrative requirements from referring centres was introduced. Patients were only accepted for the heart team meeting if all required information was complete. Second, another cause for delayed decision making was an overfull list of patients being offered for treatment. Therefore, a secretary was appointed to enhance preparation of the heart team meeting with a detailed agenda and an overview of complete patient information. These countermeasures eliminated time of searching for patient information during the meeting and supported timely preparation of patients for surgery. Furthermore, time was saved by standardisation of documentation after decision making and direct, electronic communication to referring centres and practitioners.
One-stop-shop preopoperative clinic
To minimise the number of preoperative visits and reduce time to treatment, a one-stop shop care carousel was created. During a single hospital visit, patients were consulted by a nurse practitioner (NP) or physician assistant (PA), anaesthesiologist and cardiac surgeon for all required diagnostics (ECG, bloodwork, X-thorax). Doctor assistants coordinated patient flow. They ensured the exchange of all required information and documentation for successful admission and surgery as well. The one-stop-shop visit was not planned before the date of surgery was known, which prevented repeating of preoperative diagnostics (eg, X-ray), if they were older than 6 weeks. This is an example of the application of the Lean ‘pull’ principle, which assumes that one should only produce if there is demand. In this case, a patient should only be prepared for surgery once a date of the surgery is planned, so that preoperative diagnostics are still up to date at the time of the surgery.
Perioperative phase
Smart OR scheduling
The Pareto chart shows that overrun of a previous surgery is the most common reason to cancel a surgery. ‘5× Why’ analysis showed that ‘unrealistic planning’ is an underlying root cause, for example, scheduling two subsequent high complex cases in one OR. We, therefore, introduced a new flexible OR schedule, consisting of basic weekly schedules with time slots. Patients were assigned to time slots depending on the predicted duration of the surgery. More accurate time predictions together with risk stratification were implemented. Characteristics used to predict time durations for CABG were complexity of the procedure and patient characteristics, for example, number of bypasses, type of CABG and Euroscore II.27 Time slots were reserved for urgent surgery to avoid cancellations of elective cases. There was an additional list created of elective cases to fill the time slot if there was no patient for emergency surgery.
Surgery check-in
Another cause for overrun of procedures were ‘late starts’. A specific problem-solving session (Kaizen) on this topic resulted in the introduction of a surgery check-in with all involved healthcare professionals present before the procedure started.23 28 This forced the team to arrive on time, check completeness of materials and discuss potential bottlenecks and challenges, avoiding delays during surgery.
Culture of engagement
The project team members admitted that working in independently organised ‘silo’s’ in the CABG care pathway resulted in suboptimal working practices and the inability to see the impact of actions in other parts of the process. The VSM sessions, the analysis of patient surveys and shared experiences by the project team, provided insights in the impact of delays and cancellations. It is strongly believed that the Kaizen procedure would result in increased responsibility and commitment by the full team towards the patient, the treatment plan and the schedule of the day.
Support from the board
To encourage finishing the entire elective OR programme, even when the last procedure was expected to end later than scheduled, the hospital board approved extended surgical hours and additional payment for overtime.
Postoperative phase
To secure availability of beds in the ICU, MCU and ward after surgery, the following countermeasures were implemented in the postoperative phase:
Dedicated ICU beds
To guarantee availability of ICU beds after surgery, a service-level agreement was signed to allocate four beds for cardiac surgery on a daily base.
Fast-track ICU
Postoperative patient flow was optimised by the implementation of ‘fast-track’-procedures where patients, if possible, were directly admitted to the MCU after surgery, bypassing the ICU.
Rapid discharge
To support in-time discharge and consequently reducing preventable hospital stay that impacted patient flow, an Information Technology (IT)discharge planning tool was implemented to monitor and visualise LOS per patient. Service-level agreements were made with referring centres and nursing homes to secure availability of beds when patients were ready for discharge.
Continuous improvement
Key performance indicator dashboard
After implementation of countermeasures, dashboards with key performance indicators (KPI) were developed and monthly reviewed by the team to anticipate when cancellations or underlying causes tend to increase again.
Results
The outcomes are presented in figure 4 and table 1.
Outcomes

{kind=link}
{kind=link}
{kind=link}
{kind=link}
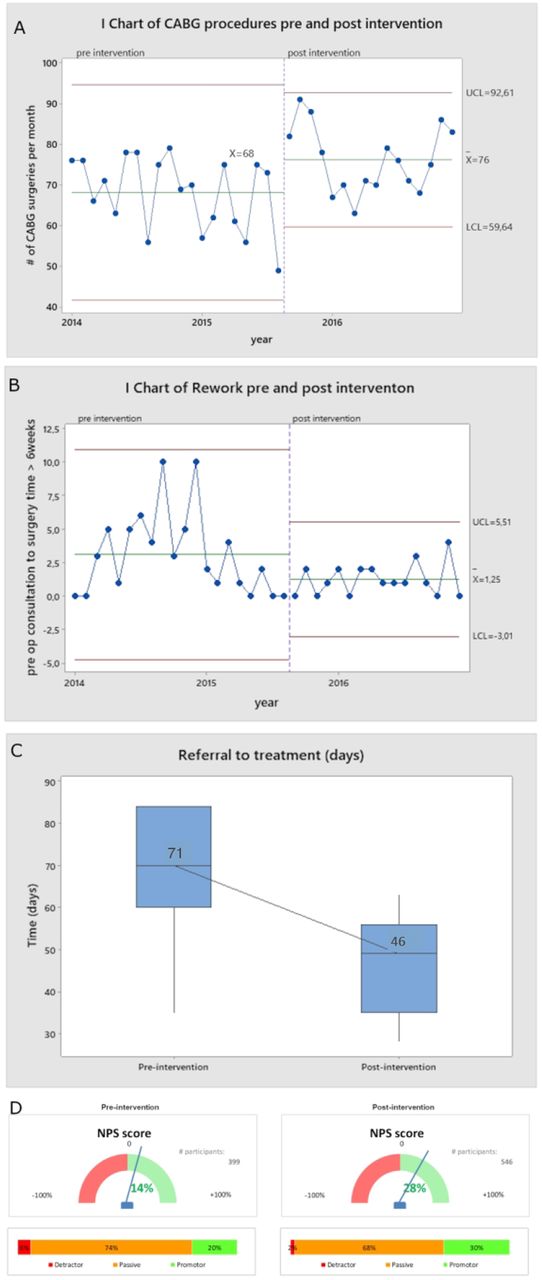
Impact of intervention(s) on (A) number of procedures per month, (B) % of rework, (C) referral to treatment time and (D) patient satisfaction. CABG, coronary artery bypass graft; NPS, Net Promoter Score; LCL, lower control limit; UCL; upper control limit.
Per month 84 CABG procedures were scheduled. The implemented countermeasures reduced the number of cancellations per month from 16 to 8 (p=0.010). Annually, this led to an increase of 95 procedures. Within the Six Sigma methodology, the error rate is defined as number of defects (cancellations) per million opportunities (DPMO). DPMO is calculated as sigma level (6 sigma equals 3.4 defects per million opportunities). This project improved the sigma level from 2.4 to 2.8.
Number of repeated diagnostic X-thorax decreased with 67%, from preintervention 3 to postintervention 1 per month (p=0.021).
RTT decreased with 35% from 71 to 46 days (p=0.000).
From the 399 patients interviewed preintervention, 20% were promoter, 74% passive and 6% detractor, resulting in an NPS of 14%. NPS postintervention (n=546) is 28%, consisting out of 30% promoters, 68% passives and 2% detractors. NPS improved with 14% (p=0.005).
Unintended consequences
Without being outcomes of this project, employee satisfaction and LOS were also positively impacted. Participation in the project increased awareness and engagement, which improved team morale. The OR-scheduling team mentioned they experienced a higher work satisfaction. Due to implemented countermeasures that enabled later admission and earlier discharge LOS was reduced from 10.5 to 9.8 days per patient on average, equalling approximately 600 hospital bed-days annually. The opportunity of extending surgical hours and paid overtime did result in more finished programmes, but not in remarkable prolonged surgical time.
Discussion
This quality improvement project reports a successful application of LSS to significantly reduce the number of surgical cancellations in a University Medical Center in the Netherlands. By applying tools such as VSM, data-driven root cause analysis, patient experience surveys (voice of the customer) and Gemba Walks, improvement opportunities along the full CABG care pathway were identified. This led to the implementation of prioritised countermeasures preoperative: (1) integrating preoperative activities in a one-stop-shop care carousel, (2) better preparation of multidisciplinary heart team meetings, (3) increased focus on ‘first time right’ diagnostics by ‘pull’ planning. Perioperative improvements included (4) flexibility of OR planning and (5) increased focus on timely start of the surgical programme. Postoperative patient flow improved by (6) introduction of ICU-fast track, (7) service-level agreements to dedicate ICU beds for cardiac surgery and (8) proactive discharge planning. These countermeasures resulted in improvements covered by the STEEEP principles.14 More efficient use of OR and hospital bed capacity enabled eight additional CABG procedures per month (p=0.010) and freed up approximately 600 hospital bed days annually, more effective scheduling of preoperative diagnostics (eg, X-rays) cut 67% of duplicated tests (p=0.021), with positive impact on patient safety (less radiation), reduction of waiting times by 35% (p=0.000) guaranteed timely access for all patients in need for care (equitable), and the more patient-centred care process increased patient satisfaction (NPS) by 14% (p=0.005).
Key strength of this study is the in-depth root cause analysis performed by the project team, represented by healthcare professionals throughout the entire CABG care pathway. Patient focus was considered as crucial. In total, 945 patients were interviewed 2 weeks after surgery. Their feedback provided the project team insights to improve the process and consequently the patient experience. Three full years of CABG surgery data were obtained, enabling enough power to prove significant improvement on all defined KPI’s. Data ere automatically generated in the hospital information system, allowing replicability and scalability. No major changes other than the process optimisation took place during the included period. Additionally, training the project team about the LSS methodology combined with support from an external LSS master black belt contributed to comprehensive and structured problem solving. We observed that involving team members across the value stream changed their perspective from independently functioning players to team players with a more holistic view on patient value across the complete care pathway. A possible contribution to the success of this project is the commitment by the board of directors to allow overtime payment, supporting to finish the surgical programme. This indicates that leadership engagement and organisational alignment are important to successfully implement the necessary change.29
Lean aims to reduce waste and optimise flow, where Six Sigma is a structured data-driven way to reduce defects and process variation. The combination of Lean with Six Sigma has been reported to have a synergetic effect.30 Nicolay et al performed a systematic review regarding quality improvement efforts, among which LSS, for surgical patients.17 Even though they included more studies that used Lean (n=4) or Six Sigma (n=5) separately, they found one study by Niemeijer et al implementing LSS (DMAIC) to reduce LOS with 3 days with a 10-month follow-up for patients with trauma.31 In their study, a VSM was performed from admission to discharge to discover factors that impacted LOS. Nevertheless, they do not report a quantitative Pareto analysis and an in-depth root cause analysis. Also, patient satisfaction was not monitored. Several publications about successful applications of LSS to various aspects in healthcare exist. LSS has been effectively applied to introduce care pathways,20 32 improve OR efficiency,16 18 19 33 shorten RTT,16 streamline discharge procedure,31 improve patient outcomes34 and improve financial performance.16 17 For reducing OR cancellations, we found only one study using Six Sigma.35 Our study combined LSS to reduce OR cancellations and focused on optimising flow in the entire care pathway and patient value, rather than a single step in the process or financial impact. Cook et al implemented LSS tools such as VSM to create a ‘focused factory model’ for cardiac surgery in Mayo Clinic (Rochester, Minnesota).36 They reduced resource use, LOS and costs by decreasing the variation within care delivery for specific patient groups, using information technology tools and empowering non-physicians at the bedside for patient care.36 The authors also reported that cultural change, persistence and leadership is essential, besides the implementation of change management itself.36
Our study supports the evidence that the right application of LSS leads to a more efficient organisation of healthcare, with improved use of resources and higher patient satisfaction. We believe that the improvements in this study can be successfully applied to other hospitals and medical conditions, yet we stress the importance of hospital teams going through the DMAIC problem solving methodology themselves. Surgical cancellations are common and not unique for cardiac surgery.37–40 Our improvements may be suitable for other hospitals, for example, organising preoperative activities in a one-stop-shop setting or a fast-track ICU. However, situations and contexts differ. Adopting change may be complicated because of hidden or unexpected powers that backfire on solutions that work perfectly elsewhere. Also, the concept of ‘not-invented-here-syndrome’ may complicate adopting change as well.
The Define, Measure and Analyse phases enhance understanding of the context and complexity, and thus preventing jumping to solutions if the root causes of problems are not identified before implementing countermeasures. Furthermore, this method encourages shaping a project team with representatives of different stakeholders from the entire care pathway, and therefore, contributing to team engagement and adopting change.41 Although we do not recommend to blindly copy improvement actions from one place to the other without understanding the context, we do recommend sharing of best practices by publishing and by exchange visits between hospitals. The latter may also strengthen team morale, inspire out-of-the-box ideas and prevent tunnel vision.
This project illustrated the consequence of fragmentation in care processes and healthcare systems in general. The system is generally organised around independent care providers (silo’s) rather than in care pathways around the patient, which is where the majority of inefficiencies can be found.42 Inefficiencies in care delivery systems lead to imbalance and suboptimal flow, resulting in waste such as cancellations, repeating of diagnostics, prolonged RTT, waiting lists and consequently lower staff satisfaction. This is a vicious downward spiral between process waste (Muda), unevenness or variation (Mura) and overburden of the system (Muri).43 The challenge of improving healthcare finds itself in understanding the complex whole of interrelated and interconnected parts, rather than separate entities.44 This also means that technical solutions by itself do not adequately counter problems that are influenced by a complex health system.29 Our approach ensured a pathway-centred way of identifying and resolving inefficiencies by comprehensive analyses of the context of surgery cancellations from multiple perspectives (patients, healthcare professionals with different functions, management) through the entire value stream. The visualisation of process performance and impact on the patient helped to create sense of urgency and improve team commitment, which significantly contributed to sustainable and accepted change.
The primary focus of this project was to improve quality instead of optimising hospital revenue. However, by improving the process, the hospital increases production with 96 extra surgeries annually. This gets accompanied with €1.15M additional revenue. Since hospital costs on staff and ORs are generally made regardless of cancellations, the amount of value (quality) created per euro spent on society level is increased. The in-hospital burden of rescheduling procedures, duplicated diagnostics, frustrations and negative morale have significantly improved, and these resources can now be spend to contribute positively to a sustainable system.29
The COVID-19 pandemic emphasises that healthcare capacity is scarce, and that efficient and effective use of it is required to guarantee access to high quality and affordability of healthcare. Surgical cancellations have a negative impact on all these challenges, which encouraged us to share and publish our LSS project a few years after the project was finalised.
The study has several limitations. It is a single-centre study focusing on one specific procedure. As the pre time frame and post time frame do not exactly cover the same number of months, the difference in average number of CABG procedures performed per month may be partly explained by seasonality. The large number of countermeasures implemented in the same time period, as well as the intrinsic motivation of involved project team members, makes it difficult to evaluate what the most meaningful interventions were. For example, this study has not analysed the influence of a smarter scheduling on surgical cancellations exclusively from other implemented improvements. Even though the reduction in number of repeated diagnostics is significant, it is based on a limited number. The improved NPS could also have been affected by other factors, such as a positive outcome of the surgery. The interpretation of causal relationships between interventions and results may also be compromised due to the used ‘interruptive time series’ study design. A randomised controlled trial could control for this. However, it may be a challenging study design for an LSS quality improvement project. We encourage further research to the sustainability of the improvements, for example, reported in the study of van der Voort et al.45 We believe that hospital information systems support more structured data capturing and thus facilitating real-time evaluation of KPIs, such as cancellation rates and its root causes. We recommend further research to the impact of real-word data on engagement of healthcare professionals and continuous improvement.
Conclusions
LSS is a proven structured approach that helps organisations to reduce waste and improve flow through the entire care pathway. This study shows how the application of LSS in healthcare, and particularly for reducing surgical cancellations, leads to significant improvement of resource utilisation, patient satisfaction and engagement of healthcare professionals.
Reporting
This report follows the proposed Standards for Quality Improvement Reporting Excellence Guidelines.22
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study does not contain human participants or animals. n-WMO statement issued by METC azm/UM: 2020-2430.
Acknowledgments
The authors thank the entire project team involved, and the MUMC+ Business Information Management team for their contribution in data extraction.
References
Footnotes
SS and PH contributed equally.
Correction notice This article has been corrected since it first published. Author name 'Godefridus van Merode' has been updated.
Contributors SS, SK, JM and RZ: contributed significantly to the concept, design and implementation of the work; the acquisition, analysis, interpretation of data for the work and writing of the manuscript, PH and GvM contributed significantly to the interpretation of data and writing of the manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PH, SK, JM, GvM and RZ have nothing to disclose; SS is employee of Medtronic.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.