Article Text

Abstract
Purpose The use of qualitative data to assess quality of care in nursing homes from the resident’s perspective has shown to be valuable, yet more research is needed to determine how this data can be used to gain insight into the quality of care within nursing homes. Whereas it is crucial to stay close to the stories that are the strength of qualitative data, an intermittent step to classify this data can support the interpretation and use. Therefore, this study introduces an approach that enables the use of narrative quality of care data to learn from and improve with.
Design A cross-sectional mixed-methods study in which qualitative data were collected with the narrative quality assessment method Connecting Conversations and interpreted for analysis.
Methods Connecting Conversations was used to collect narrative data about experienced quality of care in nursing homes according to residents, their families and nursing staff (triads). Data analysis consisted of coding positive/negative valences in each transcript.
Findings A stepwise approach can support the use of narrative quality data consisting of four steps: (1) perform and transcribe the conversations (listen); (2) calculate a valence sore, defined as the mean %-positive within a triad (look); (3) calculate an agreement score, defined as the level of agreement between resident-family-nursing staff (link); and (4) plot scores into a graph for interpretation and learning purposes with agreement score (x-axis) and valence score (y-axis) (learn).
Conclusions Narrative quality data can be interpreted as a valence and agreement score. These scores need to be related to the raw qualitative data to gain a rich understanding of what is going well and what needs to be improved.
- nursing homes
- patient-centred care
- quality improvement
- quality measurement
Data availability statement
No data are available. The transcripts supporting the conclusions of this article are only available in Dutch and cannot be made publicly available to assure anonymity and confidentiality of the participants.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Care provision in nursing homes has experienced a shift from being merely task-centred to being more relationship-centred, in which not only the resident’s needs, but also family and nursing staff’s needs are considered.1–3 This has resulted in a new view towards quality of care in nursing homes known as experienced quality of care. Experienced quality of care is a process that is influenced by expectations; interactions and relationships between the resident, family and nursing staff; and an assessment afterwards.4 Residents, family and nursing staff in the care process each have their own needs and aspects they consider important regarding receiving and providing high quality of care, which can differ from each other.5 6 As service receivers, residents have expressed the importance of the nursing home environment, maintaining personhood; having and maintaining meaningful relationships with staff, family and other residents and receiving tailored care.7 Residents and family have expressed the importance of feeling at home in a nursing home.8 In addition, family values personalised attention for residents, recalling who they used to be, and receiving the opportunity to take some own responsibility in the care for the residents.5 9 As service providers, nursing staff often base their judgement of experienced quality of care on their task priorities, such as delivering personal care, creating a friendly atmosphere and supporting residents emotionally.10 Furthermore, understanding residents’ behaviours is important to them.5 By including these three different perspectives, discrepancies can be identified and a better understanding of the care experiences can be established, which assures that integral quality improvement plans are focused on the correct elements and enhances support to realise these improvements.11 12
Up until recently, experienced quality of care was mostly assessed with questionnaires, such as The Consumer Assessment of Healthcare Providers and Systems in nursing homes (CAHPS-NH).13 Research however has shown that whereas quantitative data are informative for some purposes, it misses the meaning behind a rating, providing insufficient information to determine what exactly is going well and what needs to be improved.14 Therefore, narratives have shown to be a powerful complementary method to discover what residents, families and nursing staff value, and to evaluate and improve care services based on their experiences.15 16 These narratives capture an experience by providing information about the caring relationships, explaining rationales and possessing emotions.17 Connecting Conversations is a narrative method that assesses experienced quality of care by performing separate conversations with the three actors in the care triad.18 It identifies similarities and discrepancies between residents’, families’ and nursing staff’s experienced quality of care and is based on the principles of relationship-centred care. Appreciative inquiry is used to discover positive routines within nursing homes, that is, what is going well.19
Whereas Connecting Conversations has shown to be feasible and valid to assess experienced quality of care in nursing homes, there is a need to improve the usability of the narrative data for quality improvements. Merely assessing experienced quality of care is not sufficient as it is indispensable that the information can be used in practice for learning and improvement purposes.14 There is a need to discover how to use narrative data in practice, as the data are very rich and analysis is considered very time-intensive.20 21 Ideally, narratives are interpreted and classified into usable information to learn from and improve quality of care. Therefore, this study aims to introduce a stepwise approach that enables the use of narrative data collected with Connecting Conversations to acquire an interpretation of the data that can assist with initiating quality improvements.
Methods
Study design
In this cross-sectional mixed-methods study, qualitative data were collected with Connecting Conversations and quantified for analysis. Data were collected during autumn 2018 within the Living Lab in Ageing and Long-Term Care in the south of the Netherlands.22
Setting and participants
This study was conducted in Dutch nursing homes. The large majority of nursing home care in the Netherlands is publicly owned, and includes different types of wards: somatic wards for residents with physical disabilities, psychogeriatric wards for residents with cognitive impairments and rehabilitation wards for residents in need of short-term care. The majority of nursing home residents are women (73%), have a mean age of 85 years and most are diagnosed with memory problems, severe physical impairments and/or comorbidities.23 Caregivers working in nursing homes are mostly certified nurse assistants, nurse assistants and registered nurses, and most Dutch nursing homes work with self-employed elderly care physicians.24 In addition, allied health professionals are part of nursing home staff, including psychologists, occupational therapists, dieticians and physiotherapists among others.
Connecting Conversations was executed in five care organisations, including somatic wards, for older people with physical disabilities, and psychogeriatric wards, for older people with dementia (24 full care triads included). Random selection of residents on a ward was performed by generating a random sequence list of residents’ room numbers of the ward and inviting the first five residents to participate.18 This ensured equal opportunity of participation for all residents on the ward, regardless of their diagnoses, capabilities and personalities. After a resident agreed to participate, a closely involved family member and a caregiver that provided care to the resident at least once a week were invited to participate as part of the care triad.
Participants received information about the purpose of the study at least 2 weeks before the interview and submitted written informed consent. Participants could withdraw their voluntary participation at any moment. For residents living on psychogeriatric wards, the legal representative provided informed consent for their participation and during the interviews residents provided informed assent. To guarantee confidentiality of the interviews, no names or locations were documented.
Data collection
Demographic characteristics were collected for the care triads (residents, family and professional caregivers) by the interviewer. For residents, age in years, sex, months living in the nursing home, activities of daily living (ADL) assessed with the ADL-scale (range from 0 independent to 6 fully dependent) and cognitive functioning assessed with the Cognitive Performance Scale (range from 0 full cognitive functioning to 6 extremely limited cognitive functioning) were collected.25 For family, age in years, sex, relationship to resident and hours of weekly employment were collected. For caregivers, age in years, sex and hours of weekly employment were collected.
Data were collected with the narrative assessment method ‘Connecting Conversations’, which assesses experienced quality of care in nursing homes as defined by the INDividually EXperienced QUAlity of Long-term care (INDEXQUAL) framework,4 by separately interviewing residents, family and nursing staff (care triad), adopting an appreciative inquiry approach.26 This approach focuses on what is going well and how this can be done more, instead of only focusing on problems and the negative. The Connecting Conversations’ interview guide consisted of six questions to trigger respondents to share what matters to them. Questions 1 and 2 are about the resident’s quality of life and satisfaction with caregivers, asking to grade these and hereafter elaborating on what is needed to increase these grades. Hereafter, participants are asked to tell about the most positive experience in the nursing home, about an average day in the nursing home and about relationships between the resident, family and caregivers. Family and nursing staff were asked to answer the questions from the resident’s perspective. The inclusion of three actors within a triad is considered a form of data triangulation.27 Interviewers were nursing staff employed at another nursing home. They received a 3-day Connecting Conversations training in which they learnt to perform separate interviews with residents, their family and professional caregivers. The interviews were audio-recorded and summaries to each question were documented on a tablet. Full details on Connecting Conversations have previously been published.18
Patient and public involvement
Connecting Conversations has been developed and evaluated in co-creation with residents, their representatives, their families, professional caregivers, policymakers and national stakeholders.18 28 In this study residents were participants in Connecting Conversations. In addition, national experts in nursing home policy and practice (n=11), including a representative of the national client council, and a group of client council representatives (n=7) were consulted to assure suitability of the stepwise approach for practice. The national experts provided advice on the content and format of the stepwise approach during two expert panel meetings (once at the start of the development process to discuss requirements and once when the first draft of the approach was developed), to enhance suitability for practice. The group of client council representatives reflected on the content and format of the stepwise approach during one evaluation session, to assure the resident’s perspective remained represented.
Data analysis
Data analysis was performed for all 24 fully completed care triads available with audio recordings.18 Online supplemental figure S1 presents the steps in analysis: listen (collecting data), look (understanding data), link (analysing data) and learn (using data).
Supplemental material

Quadrant-graph of agreement and valence scores for each triad.
To interpret the data as a quality rating, it was important to gain insight into what the conversations were truly about. Therefore, first, interviews were transcribed verbatim by three members of the research team and read multiple times. Second, all 72 transcripts (24 triads) were coded with two codes: positive or negative. Coding was performed by one researcher and checked by another. When disagreements occurred, a third researcher was consulted and coding was discussed until consensus was reached. Only texts that were dependent on the process of care service delivery and the nursing home environment, with a clear valence expressing a positive or negative experience were coded (hereafter called segments). For example, ‘I like the food here’ or ‘the resident enjoys family visits’ were coded as positive, as these aspects were made possible by the nursing home and the words ‘like’ or ‘enjoy’ express a positive valence. Descriptions of the relationship between the resident and family, such as ‘I have a good relationship with my daughter’ or about who the resident is ‘She is lucky she can still walk and is not in a wheelchair’ were not coded, because these are not directly related to the service delivered by the nursing home. In addition, neutral segments without a valence expressing if someone was positive (satisfied) or negative (dissatisfied) were not coded, such as ‘I get showered twice a week’. To validate the coding with positive and negative segments, for six triads (25%) the researchers read the full transcripts to determine if these were overall considered positive or negative as a comparison to the coding. The research team also explored how to translate the ratio of positive/negative valences into a valence score, defined as a score ranging from a transcript being very negative (0% positive) to very positive (100% positive), based on the amount of coded segments. Third, the research team explored possibilities to determine a level of agreement between the resident, family and nursing staff. Agreement was defined as the coherence between individual resident-family-nursing staff triads, dependent on the positive or negative valence score. Agreement did not take into consideration the content of each transcript, thus only the agreement between being negative or positive. No comparison was made between the topics discussed in each conversation. As a final step, possibilities to visualise the analysed data for interpretation and learning purposes were explored. Qualitative analyses were performed with MAXQDA V.20.0.829 and quantitative analysis were performed in MS Excel V.2016.30
Results
In total, 24 triads were included for analysis, in eight nursing homes, of which eight psychogeriatric wards, four somatic wards and one acquired brain injury ward. Further details on the demographic characteristics of the triads are available in online supplemental table S1.
Narratives collected with Connecting Conversations (listen)
In each conversation, there were emotional and/or judgement words used, suggesting that care experiences are indeed expressed with positive and/or negative loaded words. In addition, similarities and/or differences between the valences of residents, families and caregivers were recognised. To portray a better understanding of this, segments from four triads, which are each very different, are presented.
For triad C, there is space for improvement. The resident misses home and believes the caregivers could gossip less and provide more gentle care. Her son also experiences challenges with the caregivers and their communication. The caregiver experiences gratitude from the resident, however also experiences a challenging relationship with the resident’s son.
‘You can’t do anything, you just sit in your chair and must stay seated. Every time you have to ask: can you do this for me? That is the worst.’ Resident (negative)
‘The caregivers often do not know [if mum attended the activities], because the volunteer arranges that. And that is…the communication is sometimes…if something happened you will not hear of it.’ Son (negative)
‘Family always wants to communicate with someone from management, while I really want to be there for their mum…I have actually never been part of all the conversations and I think that is a shame. I always ask why I am not invited and never get to hear anything about it [the conversations] or only later’ Nurse (negative)
For triad F, the resident wanted more attention, recognised by each actor. This triad portrays a clear discrepancy in the resident’s needs and expectations versus what the caregiver believes they can offer with their available resources; and a daughter who is quite positive.
‘And if I need them [the nurses] for something, I call and then they come somewhere next week…they are busy.’ Resident (negative)
‘My contact with the caregivers is good. If they need me, they know where to find me. And if I need them, I will speak to them’ Daughter (positive)
‘If you are busy with the medication round in the morning, she will already be standing in the hallway. And then she actually expects you to come directly to her. And when we tell her we will first do our rounds, because otherwise we may make mistake with the medicines, then she gets angry.’ Nurse (negative)
Triad O shows all actors touched on the topic of dissatisfaction regarding the resident’s participation in activities. On the one hand the resident wanted to be more active and on the other the resident did not want to participate when being offered the opportunity.
‘Sometimes they take me to activities and sometimes they don’t, because I fall asleep quickly…and it’s a shame that they then don’t wake me up [to join in].’ Resident (negative)
‘And you know we also had to force him a little bit to participate in the activities that are here. Because he is also quickly the type to say, no never mind. And we did not want to have that because he soon will be lonely.’ Niece (negative)
‘He always says that he wants more activities and more physiotherapy, but when we ask him for things, he doesn't want to participate at all. But he always complains about this.’ Nurse (negative)
To the contrary, in triad V all three actors were very positive about the nursing home.
‘Yes, I like to live here and I like to be here…it also gives me some security.’ Resident (positive)
‘Because she is happy with her life at the moment. She likes to be here. She has some aches and pains, but overall, I'm happy for her to be here right now.’ Daughter (positive)
‘From day one she felt like: I feel at home and I don’t want to go back.’ Nurse (positive)
Valence scores for care triads (look)
To gain understanding of how to interpret the transcripts, each transcript was coded with positive and negative coded segments and these codes were transferred into a valence score. First, the total number of positive coded segments was calculated as a percentage of the total number of negative + positive coded segments for each transcript, resulting in a so-called %-positive per transcript. Second, to validate this scoring system, for six care triads these %-positives were compared with the interpretation if a transcript was considered positive or negative according to the researchers. This showed a minimum of five coded segments was deemed necessary to determine a legit %-positive that reflected the actual information from the transcript. Third, the valence score was calculated to reflect the mean %-positive of the three actors in the care triad. This valence score was categorised as 0%–25% (very negative), 26%–50% (quite negative), 51%–75% (quite positive) and 76%–100% (very positive). The results are presented in table 1.
Valence and agreement score for each triad
Calculation and interpretation of agreement level and scores
Agreement scores for care triads (link)
To gain understanding of how the resident, family and nursing staff transcripts relate to each other, the %-positives were used as the basis for determining a level of agreement (agreement score) between the three actors. In a preliminary version, this score was calculated without making a distinction between the importance of the three actors. However, when presenting this intermittent version to the panel of experts, they determined that the resident’s perspective should weigh heavier than the families’, and that the lowest level of agreement is when the nursing staff’'s views (the service providers) differ from the residents’ (the service receivers). The reason for this is that nursing staff and residents have a continuous relationship in the nursing home founded on providing and receiving care, whereas family has a supportive role in this service encounter. This resulted in the calculation of an agreement score based on the mean %-positive, with a hierarchy of combinations between actors as presented in table 2. The starting point was that a difference of ≤25%-positive between actors was considered a high level of agreement, and a difference of >25%-positive between actors was considered as disagreement. The agreement level is selected based on the largest %-positive difference between two actors. This resulted in four categories: (1) resident and caregiver and family agree (very high agreement level), (2) caregiver and family disagree (quite high agreement level); (3) resident and family disagree (quite low agreement level); and (4) resident and caregiver disagree (very low agreement level). For all care triads, the agreement scores are presented in table 1.
Combination of valence and agreement scores for care triads (learn)
The valence and agreement scores allowed for a visual representation in a graph. Figure 1 present the valence and agreement scores of 21 out of the 24 triads plotted into a graph. The x-axis presents the agreement level (from very low to very high) and the y-axis the valence (from very negative to very positive). Triads G, H and M had insufficient data from the resident to calculate a %-positive and have therefore not been plotted. The graph can be divided into eight sections, which can help to interpret the placement of triads in the graph as presented in figure 2. The positioning of a triad in the graph reflects the narrative data from the Connecting Conversations. For example, the positive triad V is plotted in the right top of the graph, whereas the negative triad O is plotted in the right bottom. Online supplemental figure S2 provides an example for the listen-look-link-learn steps for care triad F.

Interpretation of agreement and valence scores.
Discussion
The aim of this study was to introduce an approach that enables the analysis of narrative data collected with Connecting Conversations for quality improvements. Results indicate that narrative Connecting Conversations’ data (listen) can be quantified into a valence score based on positive/negative segment coding (look), and an agreement score can be deducted from this (link). In addition, these scores can be positioned in a graph portraying the level of agreement between the resident, family and nursing staff (x-axis) and the mean %-positive of the triad (y-axis). The positioning in the graph can be interpreted into eight categories ranging from very negative with very low agreement to very positive with very high agreement (learn).
Findings show that narrative data can be used to detect similarities and differences between residents’, families’ and nursing staff’s experienced quality of care. Different actors contribute towards and benefit from creating added value to an experience.31 32 Nursing homes strive to create a balance between the residents’, families’, staff’s and organisations’ needs (balanced centricity), which can also enhance their effectivity and performance.33 Nursing staff have expressed their desire to collaborate more to find solutions and implement sustainable improvements, however, undertaking action together with families and residents does not occur automatically.34 35 To improve this, a learning climate is needed in which a care organisation aims at improvement by stimulating, facilitating and rewarding learning and development.36 A successful learning climate positively influences organisational commitment and job satisfaction by providing space for decision-making, initiative and innovation, support and help from management, and support from and teamwork with colleagues.37
Our analysis show narrative data collected with Connecting Conversations can be interpreted as a valence and agreement score. One might argue this defeats the purpose of using narrative data, as eventually only a quality rating is plotted in the graph while the story behind the rating is considered most meaningful. However, the graph of plotted triads should not be considered the final outcome, but a first impression of how a nursing home is performing. Based on this, a better understanding of the conversations can be achieved. Taking into consideration the desire for a more learning culture, it would be beneficial to provide care teams with the responsibility to reflect on and learn from narrative quality data together with residents and family. This provides care teams with more voice and responsibility in their quality reporting and improvement initiatives, which is a response to a recent Dutch advice pleading for a change in bureaucratic quality reporting.38
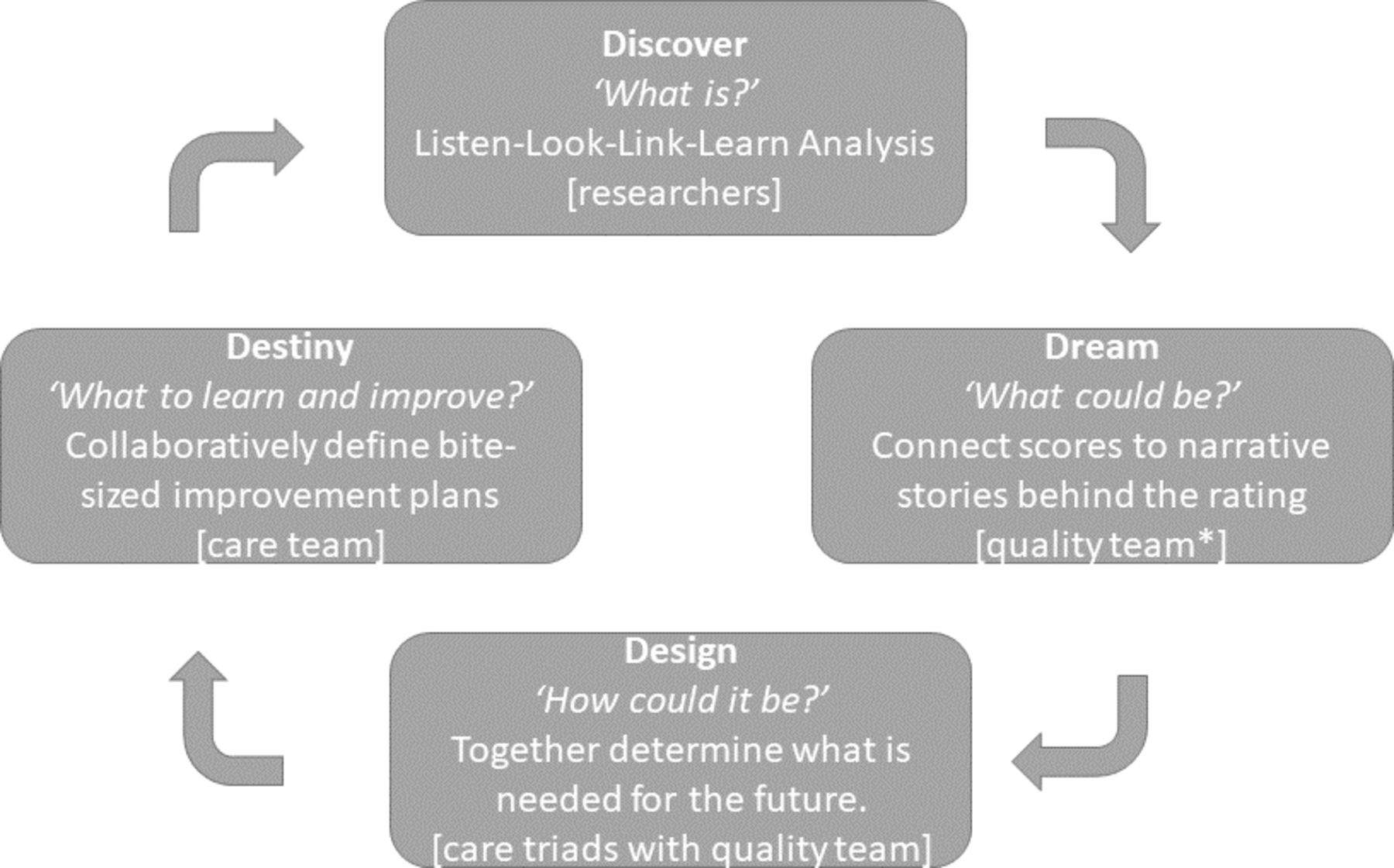
To support nursing staff to reflect on and learn from narrative quality data together with families and residents on an operational and tactical level, the 4-D cycle of appreciative inquiry can be used as portrayed in figure 3: discover and appreciate what is, dream and envision results, design and co-construct and sustain destiny.26 To achieve this, it is recommended to assign a representative group with the responsibility of addressing the 4-D’s, consisting of nursing staff working on the participating ward, family and residents living on the ward (hereafter called the quality team).11 The members of the quality team are assigned as champions, which could increase the chance of successful quality improvements.39 Together the quality team can identify what is going well and what could be improved on the ward based on the Connecting Conversations data. They can do this by discussing the findings in the graph (discover) and hereafter relating the positioning of the triads to the raw narratives elaborating on these scores (dream). They are also responsible for providing the scores and stories back to the triads in order for the actors to discuss and align their differences and similarities (design). Especially for triads with discrepancies between actors, it is recommended to have a meeting together aimed at discovering why there are discrepancies and what needs to be improved. Hereafter, learning objectives are formulated for future care provision, focused on what is going well and defining bite-sized improvement plans, keeping them achievable in busy care routines (destiny).40 On a strategic level, the quality team can report the valence-agreement graph with accompanied improvement plans back to management for transparency and accountability purposes. This operationalisation of the 4D framework should be tested in practice.
{kind=link}
{kind=link}
{kind=link}
The 4-D cycle to learn from and use narrative quality data for quality improvements. *The quality team consists of nursing staff, family and residents in the participating ward.
Several methodological considerations need to be addressed. First, Connecting Conversations is an assessment method adopting an appreciative inquiry (positive) approach. Questions asked are, for example, ‘what is the most positive experience in the nursing home?’ and not the most negative experience. One might expect this enhances positive results. However, when adopting this approach, the negative is also addressed, yet respondents tend to dwell less in this and think more in sustainable opportunities.41
Second, one should take into account that the approaches used in the data collection could have influenced outcomes. Interviewer bias was decreased by providing staff members 9 hours of interviewer training. Our feasibility findings confirm most interviewers were sufficiently skilled after the training, however this was not the case for all, as interviewing remains a skill that not everyone is equally good at. The risk for reporting bias was decreased by not just summarising, but also audio-recording all conversations with an application. This allowed the performed analyses to be based on transcripts instead of summaries. The content analysis was guided by the INDEXQUAL framework and was used to code the data collected with Connecting Conversations. In order to prevent interpretation bias, four different researchers were involved in this process.
Third, the cut-off for %-positive of 25% increments was manufactured. Henceforth, a resident with a 49% positive would be considered quite negative, whereas a resident with 51% positive quite positive. Therefore, it is important to not solely focus on the %-positive, but also focus on the relative difference in %-positive between the resident-family-caregiver in the triad. Fourth, coding %-positive and plotting the graph is time-consuming and prone to researcher’s subjectivity. It is not expected that nursing staff performs the look-listen-link-learn analysis steps. Therefore, it is desirable to explore opportunities to automate this process with, for example, text-mining and sentiment analysis.42 43 Additionally, this would allow for more distinction between words used. As now, ‘it is great’ and ‘it is quite good’ are both coded with the same weight of positive, whereas sentiment analysis could correct for intensities of words and word combinations being used, providing a more actual representation of the narratives.
In conclusion, narrative stories collected with Connecting Conversations contain useful information for triads and teams to reflect on, learn from and improve with. It would be beneficial to embed Connecting Conversations into a total quality management cycle of nursing homes and create a learning climate. Future research should however first focus on testing the use of valence and agreement scores in practice with the 4-D cycle.
Data availability statement
No data are available. The transcripts supporting the conclusions of this article are only available in Dutch and cannot be made publicly available to assure anonymity and confidentiality of the participants.
Ethics statements
Patient consent for publication
Ethics approval
The Medical Ethics Committee of Zuyderland (Reference number: 17-N-86) approved the study protocol.
Acknowledgments
The research team would like to thank all interviewers, participants and care organisations that participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors have made substantive contributions to the manuscript. KYJS, JER, JPHH, SZ, GO-S, JMGAS and HV were involved in the study design. KYJS, JER and EdV were involved in data collection and KYJS, JER and HV were involved in data analysis. All authors—KYJS, JER, JPHH, EdV, SZ, GO-S, JMGAS and HV—have read, reviewed and approved concepts and the final version of the manuscript.
Funding This research was funded by seven long-term care organisations within the Living Lab in Ageing and Long-Term Care: MeanderGroep, Cicero Zorggroep, Envida, Sevagram, Zuyderland, Mosae Zorggroep and Vivantes; and by the health insurance fund CZ, 201600132. This work is co-supported by Limburg Meet (LiMe).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.