Article Text

Statistics from Altmetric.com
Introduction
Patient safety has become a global priority to support reducing harm associated with healthcare delivery.1 In Canada, patient safety incidents (PSI) are the third leading cause of death behind heart disease and stroke and are associated with an additional cost to the healthcare system of $2.75 billion each year.2 PSIs occur across the healthcare continuum, but over half are associated with surgical care, which consists of preoperative, intraoperative and postoperative care.3 4 Globally, four main threats to surgical safety have been identified: (1) insufficient recognition of safety as a public health concern, (2) lack of available data related to surgical outcomes, (3) the inconsistent implementation of existing safety practices, and (4) the complexity of the surgical setting.5 The WHO Guidelines for Safe Surgery, published in 2009, have increased and highlighted the importance of surgical safety worldwide. However, key gaps related to complexity of surgical processes still remain to be addressed. A leading cause of these events is communication failure between care providers during surgical care, and between transition points during ‘hand-offs’ or ‘handovers’.6 Information shared at these transition points is required to facilitate continuity of information and patient care, and to prevent medical errors.7 This has resulted in national organisations, such as the Canadian Patient Safety Institute (CPSI), identifying surgical safety as a key priority.
In a joint review by the Canadian Medical Protective Association (CMPA) and the Healthcare Insurance Reciprocal of Canada (HIROC), data from 2004 to 2013, which consisted of 2974 legal cases, were reviewed and nearly half of the incidents occurred due to system-level factors, rather than physician or healthcare provider (HCP)-level factors.8 A frequent system-level issue was lack of adherence to protocols, such as use of the surgical safety checklist (SSC), which is intended to improve team communication.8 9 In addition to incidents that cause patient harm, PSIs also include events that do not lead to patient harm as well as near-miss events.10 Hamilton and colleagues report that near misses and adverse events are under-reported, particularly within the operating room (OR) setting suggesting that exploration of how teams communicate in all phases of surgical care is necessary.11
The purpose of this narrative review is to identify and summarise leading practices, tools and resources for effective communication and teamwork during surgical care including the immediate preoperative, intraoperative and postoperative phases.12 This review addressed the following questions:
What practices, processes and tools are currently being used to improve communication and teamwork during surgical care?
How are these practices, processes and tools being implemented into surgical practice?
Methods
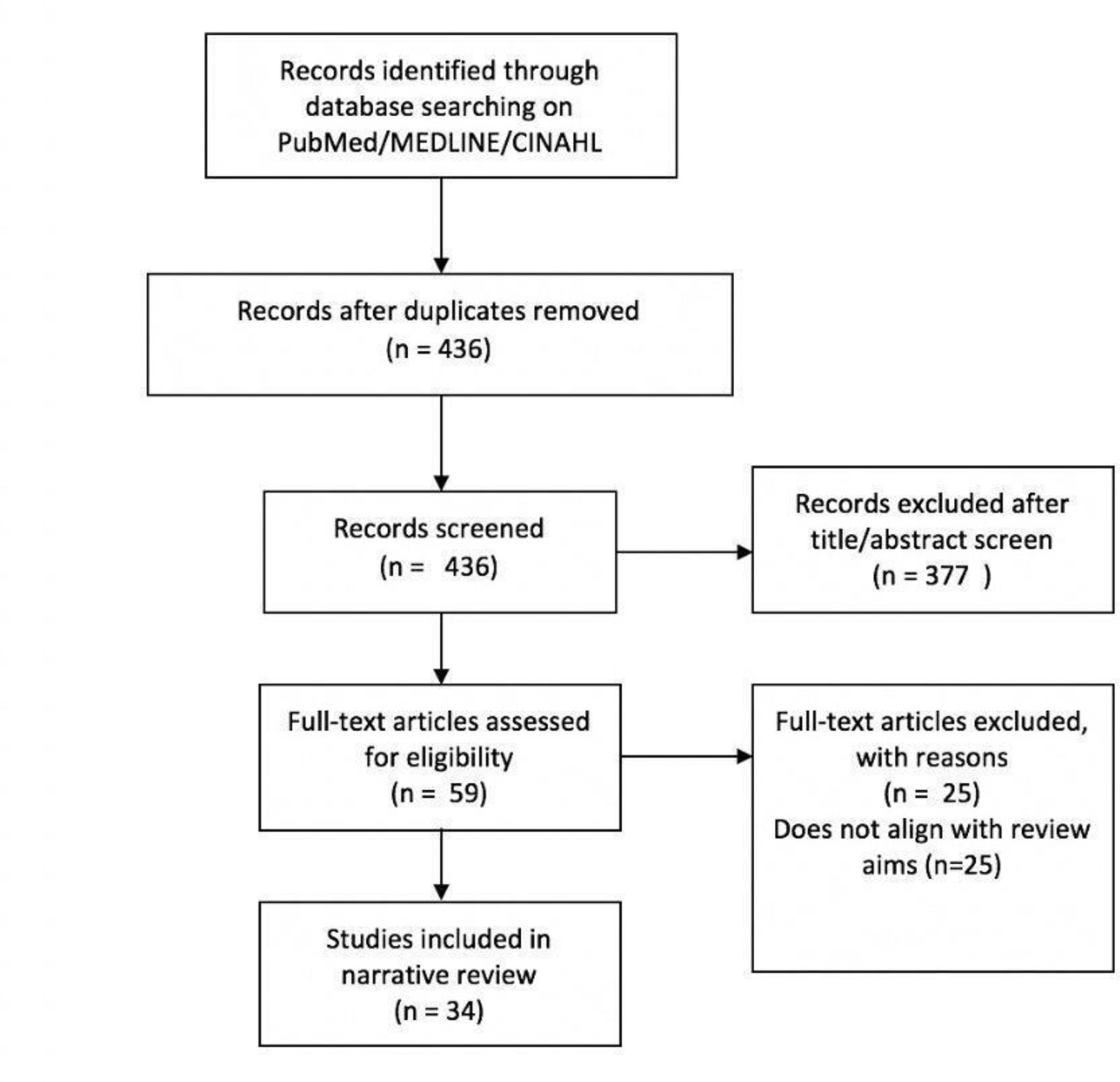
We conducted a narrative review to explore existing practices, processes, tools and resources available to improve communication and teamwork during all phases of surgical care.13 14 We searched the databases PubMed, MEDLINE and CINAHL using a variety of search terms associated with preoperative, intraoperative and postoperative care (table 1). Online supplementary file 1 provides detailed information related to the search strategy.
Supplemental material
Summary of search terms
Included articles were peer-reviewed journal publications and contained a sample or direct link to a process or tool intended to improve communication or teamwork during surgical care. We excluded articles not published in English. Two authors screened the articles based on title, topic and publication type. The content from the articles was organised into a table to allow for comparisons of article type, year, country and process or tool. In keeping with narrative review methodology,13 the articles were not critiqued or assessed for quality. This type of review process therefore allows for the summary of literature in common themes, but does not necessarily facilitate the provision of practice recommendations.13
Results
Thirty-four articles, published from 2007 to 2017, were included. Figure 1 Four articles were related to all phases of surgical care, 3 focused on preoperative care, 8 on intraoperative care and 19 on postoperative care. Half of the papers were from the USA, with additional perspectives from the UK, Canada, the Netherlands, Germany, India, Singapore, France and China. Detailed information related to the bibliographic information, descriptions of processes or tools, countries and clinical settings is located in table 2. The results have been organised into three categories: (1) modifications of processes or tools, (2) facilitators and barriers of process or tool use, and (3) description of theory underpinning processes or tools.
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Table 2Description of included studies
Modifications of processes or tools
The reviewed work included processes or tools that were modified to accommodate the needs of particular contexts prior to implementation. The most commonly described tool to facilitate communication and safety during the intraoperative period was the SSC.9 Literature for the intraoperative period was predominantly related to the implementation or modification of the SSC or the evaluation of its effectiveness. The checklists were available in write-in formats,15 electronic versions16 and posters.17 18 A shared responsibility in completing the checklist was described; however, the team member leading the implementation of the SSC varied. For example, the surgical residents led the checklist in one study19 whereas the nurses led the checklist completion in another.20 A few studies suggested that the implementation of the SSC in the perioperative setting improved patient outcomes, improved patient safety, improved communication and teamwork and decreased complications.18 21–25 Limitations were related to the human factors that affected the implementation of the SSC.26 27
The SSC was adapted to the specific setting by adding or changing items, although the removal of items was not recommended.15–17 28 29 For example, the SSC was systematically adapted for use in robotic urological surgery, using a systems evaluation tool to identify potential causes of error.15 The checklist was developed presuming that it would undergo further iterations, given the innovative and dynamic nature of the field of robotic surgery.15 A similar tool was developed and implemented for robotic gynaecological surgical procedures, which led to significant reductions in 30-day readmission rates.16 Furthermore, displaying the tool on a large monitor in the OR provided a focal point for the team to gather and could contribute to team cohesiveness.16
Other studies also commented on the applicability of the SSC to unique perioperative settings, such as small ambulatory surgical settings; therefore some created a modified SSC version that would be applicable to their case population,17 29 or frequent patient needs such as advanced age or obesity.28 Literature supported the creation of intraoperative-specific pathways for surgical settings, which reflected the specific communication needs of these types of teams.16 19 30 31 In one instance, the SSC was adopted in addition to a flow checklist designed to follow the patient trajectory throughout the surgical journey from induction to the postanaesthesia care unit (PACU).32
Additional articles described the development of checklists distinct from the SSC, which were also modified in terms of content or delivery. For example, the SURgical PAtient Safety System (SURPASS) checklist was intended to decrease adverse events for surgical patients, from admission to discharge.33 The authors validated this tool through a process of observing procedures and noting deviations from checklist use, which often corresponded to variations in personnel and logistics.33
The engagement of all team members, particularly nurses, was described as a facilitator of success when a process and checklist were implemented to improve handovers between the OR, intensive care unit (ICU) and PACU settings.34–36 Some articles described modifications that participants made to checklists during the implementation period. Most often, participants appeared to strategically omit particular checklist items; for example, a subset of items continued to be routinely omitted in two studies,37 38 which could suggest that these items are perceived as non-essential during handover.39
Tool implementation appeared to contribute to longer time spent on handovers, which could be viewed as a deterrent to tool usage.37–41 Particularly, a lack of compliance to use the checklist by anaesthesiologists could be contributed to a gap in training on checklist use.37 Furthermore, some anaesthesiologists expressed that they would not likely integrate the checklist into their practice, as they described it as ‘insulting’ to their years of training, which could indicate a need for education to address attitudes towards standardisation and safety.37 In contrast, two handover processes did not significantly increase handover time, but improved team communication and information transfer.42–44
Facilitators and barriers to uses of processes, tools or resources
Education and training
In a subset of the selected articles, the implementation of a checklist or procedure was paired with a varied educational intervention to facilitate the change. To facilitate the implementation of the SWITCH (surgical procedure, fluids, instruments, tissue, counts and questions) tool, it was discussed at in-service meetings, HCPs were provided with opportunities to use the tool in role-play activities, and resources were made available in the OR. An educational intervention was developed to accompany the implementation of an ISBAR (identification/introduction, situation, background, assessment, request/recommendation) tool for handovers between the OR and PACU.45 These comprised 30 min education sessions and the provision of visual cues on unit walls, which led to mixed results for compliance rates.45 The authors suggest augmenting education and acknowledging the impact of leadership and culture in different contexts.45
Multiple theory-informed educational interventions, including webinars, simulation scenarios and refresher courses, were developed to ease implementation of a standardised, electronic PACU handover tool.46 The authors reported that improvements in the quality of PACU handovers were sustained up to 3 years after the intervention.46 Similarly, month-long training and practice trials were referenced as a contributor for improved outcomes related to information exchanges and improved patient outcomes, in relation to the handover process from the OR to the paediatric cardiac ICU.47
Staff buy-in
Some of the described interventions incorporated input from HCPs prior to implementation. For example, front-line HCPs from the OR and ICU settings were consulted when developing a protocol and checklist to improve patient handoffs between these settings.41 In a study that examined the postoperative handover process, the importance of eliciting feedback throughout the implementation process was emphasised, as this opportunity provided staff with a sense of ownership in regard to the change.48
Staff buy-in could also be a factor in who participates in the intervention. In a study that described the development of a postoperative anaesthesia tool, the anaesthesia residents did not participate in the research; therefore, only handoffs between CRNAs (certified registered nurse anesthetists)and PACU registered nurses (RN) were evaluated.49 The researchers suggested that long-term implementation would be strengthened by buy-in from all HCP groups.49 In another study, tool use was improved when a particular nurse circulator was present, and the need for staff buy-in to support implementation was noted.16
Regarding the implementation of a modified SSC for ambulatory surgical facilities, it was suggested that poor tool uptake was due to introducing it as an institutional requirement without previously consulting stakeholders.29 A hierarchical culture might have contributed to RNs feeling hesitant to use the checklist, if not supported by the attending surgeon.29 Similar cultural barriers during the original SSC implementation such as culture and organisational hierarchy were referenced.15
Contextual factors such as high nurse turnover were described as a barrier.36 With support from leadership and administration, the process of improving a preoperative assessment clinic was described by improving staffing levels, aligning processes with best practice procedures and modifying space to improve efficiency.50
Staff well-being
To improve the functioning of a preoperative assessment clinic, changes to patient-facing policies and staffing structures were re-examined, which led to positive staff-related outcomes, such as decreased sick time, decreased overtime and better staff morale.50 The importance of measuring non-clinical outcomes, such as teamwork and nurse satisfaction, was acknowledged.51 Improved non-clinical measures, such as teamwork, were linked to successful clinical outcomes.51 The professional differences in communication between HCPs when developing a face-to-face handover process from the OR to the paediatric cardiac ICU were described.52 Engaging all stakeholders improved HCP satisfaction with handovers and contributed to the ‘feeling of a team approach’.52
Safety culture
Improved outcomes associated with their electronic checklist were not solely attributable to the tool, but also to discussions generated by the tool in relation to safety-focused attitudes and behaviours.53 Additional studies attributed successful tool implementation to contexts with strong safety cultures; conversely, non-compliance could be in part related to local attitudes towards safety culture.33 54
The implementation of a 19-item SSC resulted in a decrease in patient death from 1.5% to 0.8%, and a 4% decrease in inpatient complications.18 The authors suggested that the introduction of the surgical pause for a multidisciplinary briefing could be linked to improved attitudes towards safety.18 In another study, which described a series of evidence-based clinical care pathways specifically for patients having total joint replacement surgery, all staff were trained in Lean Sigma Six principles.30 This could promote a culture that values improving performance by leveraging a team approach.30
Ease of use
Multidisciplinary team members that implemented the SURPASS checklist suggested that integration with the hospital electronic system could promote tool use.33 The implementation of a standardised electronic checklist was described to improve intraoperative handoffs between anaesthesiologists and transfers of paediatric surgical airway patients to medical settings.53 55 The electronic format was particularly convenient, as the described patient transfers were between institutions.53 Some authors emphasised the importance of selecting tools that were short, to balance ease of use with team engagement.44 For example, the rationale for selecting the SSC was based on simplicity and cost-effectiveness; whereas other tools such as the SURPASS checklist were viewed as difficult to implement due to additional items.18 In contrast, some interventions were easy to implement, but de-emphasised the role of team communication during the handover process.
Description of theory underpinning processes or tools
Few studies gave explicit reference to theory to support the development of handover processes or tools. However, safety theory was noted in the development of the SURPASS checklist to decrease adverse events for surgical patients, from admission to discharge.33 The SURPASS tool is built on safety and human factors literature within the field of aviation.33 Two studies included reference to high-reliability organisations.49 51
Theory was also used to understand the effects of tool implementation. For example, the use of 40.6% SURPASS checklists was linked with one or more intercepted errors.56 The authors referenced Reason’s Swiss cheese model to describe that the success of the SURPASS checklist could be attributed to ‘spreading out’ the safety checks over the course of the surgical trajectory.56 A few studies referenced the use of quality improvement methodologies, such as Six Sigma.40 57 Team theory was referenced when describing the use of the ‘I-5’ mnemonic to create a shared mental model during OR to cardiac ICU handoffs.58
Discussion
This review provided an overview of the existing processes, tools and resources used to improve communication in perioperative settings, as well as a description of the ways in which they are used. More than half of the papers described tools to improve intraoperative team communication, such as modified versions of the SSC. In a recent editorial, Urbach et al highlight that although current evidence does not conclude that patient mortality was decreased at the population level given SSC use, it has been shown to improve team dynamics and staff satisfaction; however, the consideration of contextual factors impacting the SSC implementation is critical to success.59 Recent work has highlighted that the adoption of the SSC is informed by factors related to the surgical team members’ perceived importance of the tool, the profession leads the SSC use (eg, surgery, anaesthesia or nursing), and differences in workflow.60
Similar to this review, CPSI reported that most tools or processes seek to structure or standardise communication, often in accordance with processes from high-reliability industries, such as aviation, with a need to shift patient safety culture.61 In our review, patient safety culture was often referred to as a barrier to process or tool implementation. For example, the implementation of the same tool could lead to different patient outcomes in different hospitals, and was attributed to different attitudes towards safety culture.33 54
In exploring the role of culture, it appears that the promotion of safety culture could inadvertently promote staff well-being or engagement. Some improved staffing policies, among other changes, in an effort to improve patient outcomes at a preoperative assessment clinic.50 This led to unanticipated positive staff-related outcomes, which suggests that what is good for patients can also be good for staff.62 For example, better patient outcomes can translate into staff that feel less frustrated and therefore can better focus on care quality and safety.50 The importance of measuring outcomes related to staff satisfaction and teamwork was emphasised.51 These insights align with current conversations to expand the Triple Aim framework to attend to the well-being of the healthcare workforce.63 64
There was limited exploration of the nature of teamwork either before or after implementation. Few studies explicitly measured teamwork and few studies alluded to professional hierarchies or ways of working as barriers. This is a clear area for further study given the lack of available information within the context of the implementation of a communication tool within a perioperative setting.
Joint recommendations were issued by CMPA and HIROC following a comprehensive review of surgical safety.8 To address system-level factors, recommendations were to implement standardised protocols, measure outcomes in order to evaluate protocols, support a culture of safety that promotes open communication and to provide multidisciplinary education to build skills related to teamwork and communication.8 From our review, it appears that there has been successful implementation of a range of standardised protocols to improve perioperative communication and distinct effort has been made to evaluate the impact of patient outcomes. However, the need to improve safety culture and provide multidisciplinary education persists. In the reviewed literature, the education offered was more akin to training, as it was focused towards implementing a specific tool or process. Education could be improved if understood more broadly and acknowledge existing professional tensions that hinder teamwork, and ultimately the push towards a culture of safety.
Conclusion
This review highlights the importance of effective communication within surgical settings, as well as the difficulties of communicating within surgical teams. The large number of processes and tools developed to improve team communication during all aspects of surgical care highlights efforts to promote structured, yet open communication. This balances the comprehensive nature of information transfer, while maintaining spaces for team members to comfortably ask questions or dialogue. The findings indicate that seminal tools, such as the SSC, are widely adopted and are frequently modified to suit the particular needs of the surgical specialty or used in conjunction with additional processes. In addition, contextual factors such as education, staff buy-in, staff well-being, safety culture and ease of tool use can function as facilitators or barriers to implementation. The use of safety or team theory could be more explicitly addressed either in the development of implementation of these processes or tools. This information could be useful for clinicians seeking existing tools or processes to improve teamwork and communications in surgical settings or for those looking to enhance the implementation process.
Acknowledgments
Carla Williams, RN, MHSM, GNC(c), senior programme manager, Canadian Patient Safety Institute, Ottawa, Canada.
References
Footnotes
Contributors SE and MD conceptualised and planned this review. MG and AL conducted the initial literature search and summarised the findings. AI updated this literature search, constructed themes in consultation with SE and MD, and drafted the manuscript. SE and MD provided critical revisions of the manuscript.
Funding We acknowledge the funding support from the Canadian Patient Safety Institute.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.