Article Text

Abstract
Background Medicines optimisation and adherence support are essential to secondary prevention after myocardial infarction (MI). Following successful implementation of a consultant pharmacist-led post-MI medicines optimisation clinic, the service was expanded by training advanced clinical pharmacists to manage clinics (with appropriate multidisciplinary team support).
Methods Key steps in the development process were: definition of a key competency framework based on relevant qualifications and experience, knowledge, skills and clinic management practicalities; creation and enaction of trainee-specific development plans to address gaps (including independent learning, teaching from multidisciplinary colleagues and shadowing in clinics); establishment of relevant protocols and proformas to ensure consistent standards (eg, a patient self-reporting tool for identifying adherence barriers, consultation proforma, directory of clinical parameters and pathway for onward referral when needed); phased clinic roll-out, initially under supervision; and gathering of feedback from patients and colleagues. Clinic letters from 50 attending patients were reviewed to quantify resulting interventions; the first 50 anonymously completed patient feedback questionnaires were also analysed.
Results Expansion of the service initially doubled capacity. A review of clinic letters from attending patients demonstrated that various interventions were recommended, including further investigations, medication changes, lifestyle adjustments and onward referrals. Most respondents to the patient feedback questionnaire thought the clinic was patient friendly and welcoming (n=48/50; 96%); felt listened to (n=48/50; 96%); considered that adequate explanation was given (n=47/50; 94%); and felt clear plans were provided (n=45/49; 92%). Most agreed that it was valuable (n=44/50; 88%), and the mean rating was 4.48 (on a scale of 1 (very poor) to 5 (excellent)).
Conclusions A person-centred post-MI medicines optimisation service was successfully delivered by appropriately trained advanced cardiology pharmacists. A structured competency framework and training programme were required, but once completed, the clinic was highly valued by patients. A similar model could be rolled out elsewhere with adaption to local requirements.
- Pharmacists
- Health professions education
- Hospital medicine
- Healthcare quality improvement
- Patient-centred care
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Pharmacists
- Health professions education
- Hospital medicine
- Healthcare quality improvement
- Patient-centred care
WHAT IS ALREADY KNOWN ON THIS TOPIC
Medicines optimisation and adherence support are essential to secondary prevention after myocardial infarction (MI) but are often suboptimal.
WHAT THIS STUDY ADDS
A person-centred post-MI medicines optimisation clinic was successfully delivered by appropriately trained advanced cardiology pharmacists (underpinned by a structured competency framework and training programme). This doubled overall capacity. Patient feedback on the service was highly positive.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
A similar model could be rolled out elsewhere with adaption to local requirements—offering potential to improve patient management and reduce the burden on busy cardiology outpatient clinics.
Introduction
Secondary prevention through risk factor modification is essential to long-term patient care following myocardial infarction (MI).1 2 This requires meticulous optimisation of drug therapies and risk factors to ensure that all of the required treatment classes are prescribed—and are maintained at appropriate doses. However, many patients in the UK and elsewhere receive suboptimal secondary prevention.3–5 Indeed, a recent European study showed that only 58% of those with previous MI were receiving the full package of guideline-recommended secondary prevention medicines (SPMs).5 Furthermore, adherence is often poor6 7; local data from our area of the UK showed that almost half of patients with coronary artery disease were not adherent to at least one SPM.8 9
This led us to establish a novel, person-centred medicines optimisation clinic for individuals who had recently been discharged following MI, run primarily by a consultant cardiology pharmacist with access to a cardiologist when required. Launched in 2015, the aims of this clinic were to provide patients with a comprehensive review of their SPM needs; to facilitate discussion of their medicines-taking experience and potential barriers to adherence; and ultimately to improve outcomes. An analysis of 270 patients who attended the clinic during its first 15 months in operation demonstrated that these aims were being met: the proportion receiving optimal SPM was significantly increased, adherence rates were significantly improved and hospital readmission rates had declined.10 Furthermore, despite having access to a cardiologist if needed, over 95% of patients were seen only by the consultant cardiology pharmacist—thus freeing up cardiology outpatient clinic time. Patient feedback was highly positive.10
However, despite successful implementation, the capacity of the clinic was limited by the availability of only one consultant pharmacist. To make the service accessible to a greater number of patients with post-MI, we therefore set out to train advanced clinical pharmacists to run some clinics (with appropriate support from a cardiologist and/or a consultant pharmacist). A further expected benefit of this expansion was to broaden the range of pharmacists potentially able to lead such clinics. This could facilitate adoption of the model at other centres nationally.
The purposes of the present paper are to describe the training process and key competencies required to upskill advanced clinical pharmacists, and to provide preliminary patient feedback.
Methods
Overall process
A simple process overview is provided in figure 1, showing the key steps that were taken to enable two advanced clinical pharmacists to conduct post-MI medicines optimisation clinics.

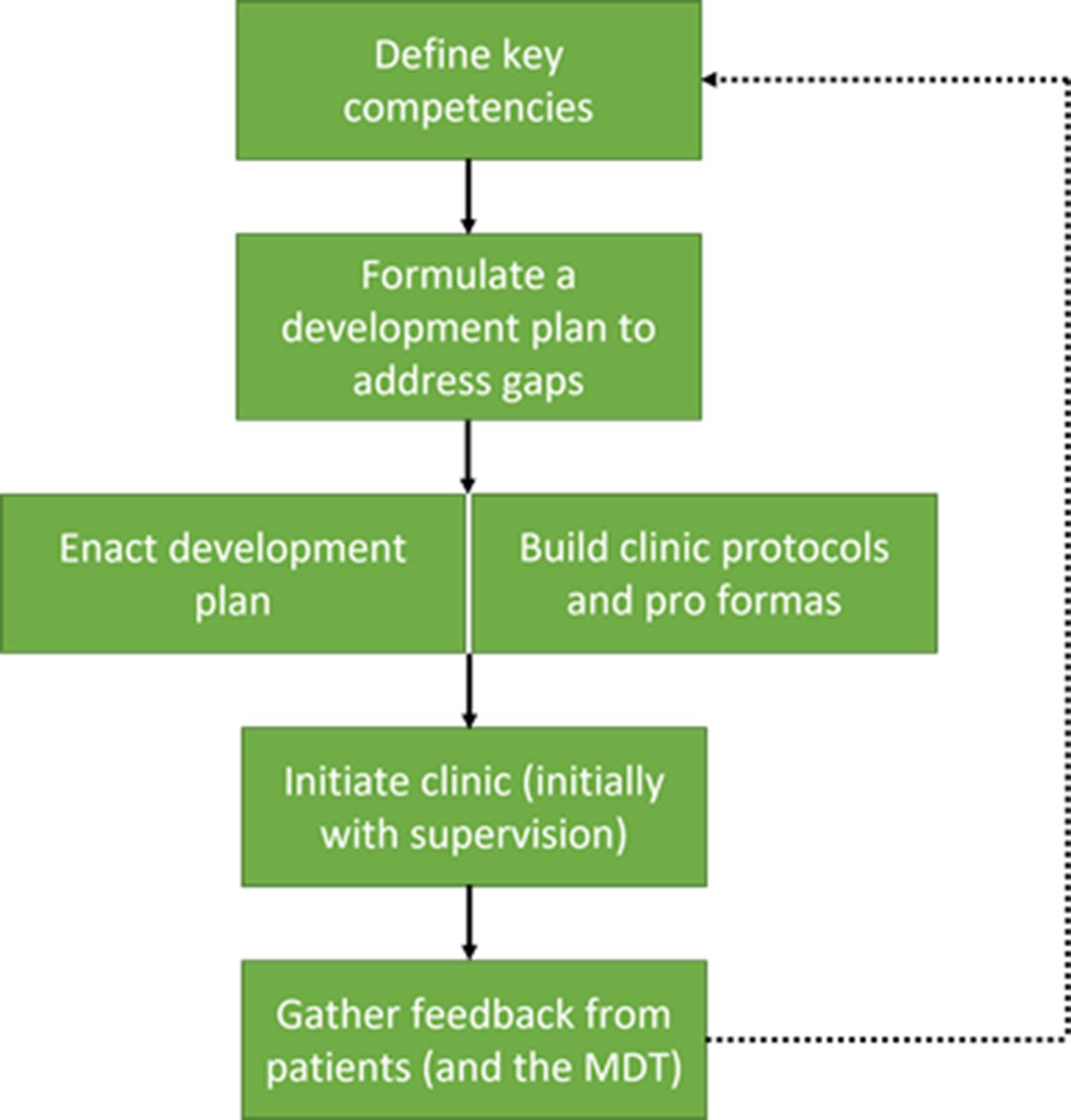{kind=link}
Key steps in training advanced clinical pharmacists to conduct post-MI medicines optimisation clinics. MDT, multidisciplinary team; MI, myocardial infarction.
As a first step, the key competencies required were defined. This was accomplished through extensive discussion with a consultant cardiology pharmacist and cardiologists already running such clinics at our centre, and by shadowing their work. The full competency framework developed from this process is shown in online supplemental table 1 and is described in more detail below.
Supplemental material
In the second step, trainee-specific knowledge and skill gaps within the competency framework were identified and development plans were established to address these gaps (table 1).
Example training plan and relevant methods
Then, in a third step, the development plan was enacted based on appropriate training methods, including independent reading and learning, teaching from multidisciplinary colleagues and shadowing in clinics. Importantly, the plan remained somewhat fluid to allow for adaptation throughout the process. At the same time, various protocols and proformas were established to ensure consistency of standards once the new clinics were launched. These included:
A patient self-reporting tool for identifying modifiable adherence barriers, known as the ‘My Experience of Taking Medicines’ (MYMEDS) questionnaire.11
A consultation proforma to ensure that all relevant topics are discussed with each patient.
A predefined directory of key clinical parameters, targets and monitoring requirements (eg, relating to blood pressure, lipid profiles, diabetes, etc).
Assessment criteria for consideration with each type of SPM.
A cardiac symptoms management pathway to facilitate appropriate assessment and onward referral when needed.
Letter templates for communication with patients, general practitioners (GPs) and any other relevant parties.
An anonymous patient feedback questionnaire to inform ongoing development of the clinic.
Once all of this had been completed, clinics were initiated led by the trained advanced clinical pharmacists. At first, these were observed by a consultant cardiology pharmacist or cardiologist to ensure that the required standards were achieved. Once training was complete, clinics were conducted independently (with onward referral if needed). Patients were asked to provide feedback via the anonymous questionnaire.
Based on all of these experiences, a training manual has been produced (including many of the standardised protocols and proformas described above) and this is available from the authors. The manual provides many of the tools needed for other advanced clinical pharmacists in the UK to develop and implement a similar service—although it will of course need to be adapted to local requirements.
Core competency requirements
The core competency framework for a pharmacist running a post-MI medicines optimisation clinic was divided into four main areas: qualifications and experience; knowledge; skills; and practicalities of clinic management (online supplemental table 1).
With regard to qualifications and experience, the pharmacist must be a registered independent prescriber with a secondary care clinical diploma, have experience of working on cardiology wards and be integrated into the cardiology multidisciplinary team with an understanding of each member’s role.
A strong understanding of various knowledge areas is required, including cardiac physiology and pathology, clinical presentations of cardiac conditions, the recovery process following MI, interpretation of investigations and results, the medications used in cardiac disease and relevant local, national and international guidelines.
Pharmacists running a post-MI medicines optimisation clinic may also need to develop their existing skills—and acquire new ones. These skills include taking histories of cardiac symptoms; ordering/taking and recording clinical observations and investigations; designing patient-specific management plans (in collaboration with patients); applying principles of medicines optimisation; using adherence assessment tools like MYMEDS11 and addressing non-adherence behaviours in line with current guidance; communication and consultation skills to support shared decision-making; and time management skills specific to outpatient consultation.
Finally, any pharmacist running a post-MI medicines optimisation clinic needs to understand the local practicalities around outpatient care, including information technology and record-keeping systems and clinic management.
Development planning for attaining key competencies
Development plans were personalised to the individual pharmacist based on a variety of training methods, including independent learning, teaching from relevant colleagues and various forms of shadowing within clinics (table 1).
Two aspects that were particularly challenging at our centre—and may also be challenging for other pharmacists coming from inpatient care—were (1) clinic-based consultation skills and (2) symptom management and escalation.
With regard to clinic-based consultation skills, a key requirement was to upskill experience with inpatients (based primarily on providing information about the rationale for medicines use, monitoring requirements and possible side effects) to an outpatient setting. This necessitated more in-depth discussion of complex topics, such as explaining tests and their results, and conducting sensitive conversations around the prognosis and management of their condition. The training process began with observation of clinics led by cardiologists and a consultant cardiology pharmacist. Trainees then proceeded to run clinics themselves under strict observation to allow for constructive feedback. Another key consultation skill that required development was around the exploration of medicines-taking behaviours; inpatient pharmacists are rarely required to delve deeply into a patient’s beliefs about medicines, but this is a core aspect of the medicines optimisation clinic. Again, training was based around close observation by a consultant pharmacist and cardiologist. The aim was to develop a consultation style that was open, non-judgemental and person centred, that encouraged patients to discuss their medicines-related concerns and possible effects on adherence and that facilitated a shared decision-making process. A consultation proforma was created to ensure that key topics are always covered with each patient, and the MYMEDS questionnaire has been routinely used to assess adherence barriers.
With regard to symptom management and escalation, training was required around clinical examinations—such as obtaining a history of cardiac symptoms, taking manual blood pressure and heart rate measurements, assessing ankle oedema and chest auscultation using a stethoscope. To develop these skills, a nurse clinical educator gave a workshop, and the methods learnt were then practised with patients. A similar process is recommended for other pharmacists looking to develop these skills (table 1). In addition, the consultation proforma provides prompts on relevant topics with regard to symptoms assessment, test results, medications and action planning. Furthermore, a management pathway was put in place for patients presenting with cardiac symptoms post-MI to facilitate assessment and appropriate referral when needed (eg, to their GP, cardiologist or accident and emergency). This was based on the five cardinal symptoms of chest pain, breathlessness, palpitations, peripheral oedema and dizziness/syncope, and was essential in ensuring that ‘red flags’ were identified and acted on.
Within the training process, a number of observed and supervised consultations were undertaken. This was adapted according to the existing expertise and progress of the trainee based on the following template:
Step 1: 20× observing patient consultations led by a consultant pharmacist or cardiologist.
Step 2: 10× patient consultations led by the trainee and observed by a consultant pharmacist or cardiologist.
Step 3: 10× independent patient consultations by the trainee with support from a supervisor if required for specific queries (although the supervisor was not present in the consultation itself).
Step 4: independent clinical practice.
Resulting interventions
Clinic letters from 50 non-consecutive patients who attended the clinic between April 2019 and January 2020 were selected from the electronic outpatient clinic notes system (several letters per month). The advanced pharmacists were working independently during this period, following completion of their training. These letters were reviewed in order to quantify the resulting interventions (further investigations, medication changes, onward referrals, etc).
Patient feedback
After attending the post-MI medicines optimisation clinic led by an advanced clinical pharmacist, patients were asked to evaluate their experience using an anonymous feedback questionnaire. This could be returned at their convenience using a prepaid envelope. The questionnaire included 12 statements for which patients were asked to assess their level of agreement on a 5-point scale (strongly agree, agree, neutral, disagree, strongly disagree), and one further question asking them to rate the clinic on a scale of 1 (very poor) to 5 (excellent). There were also two free-text questions that invited respondents to describe ‘what you liked best about the service’ and ‘what you would like us to improve about the service’. Responses were manually organised into key themes.
The present analysis is a retrospective review of data from the first 50 questionnaires received between December 2018 and April 2019. The advanced pharmacists were working independently during this period. The analysis was conducted in accordance with the Declaration of Helsinki. This was a service development project and hence no ethics committee approval was needed as per local policy.
Patient and public involvement
A patient self-reporting tool for identifying modifiable adherence barriers, known as the MYMEDS questionnaire, was posted to patients with their outpatient clinic appointment letter and patients could choose to complete this questionnaire in advance of the appointment if they wished to do so. We sought feedback from patients who attended this new service by sending them feedback surveys to complete and post back to us using a prepaid envelope. It was then up to the patients if they wanted to complete the survey and send it back.
Results
Initially, two advanced clinical pharmacists were trained to (independently) run clinics, each with capacity to see eight patients per week. This allowed the consultant pharmacist (who previously had capacity to see eight patients per week) to step aside from day-to-day clinic management. Thus, the overall capacity was doubled from 8 to 16 patients each week.
Clinic letters from 50 patients who attended the advanced clinical pharmacist-led clinic were reviewed. Most required only a single session (n=41; 82%), although a small number required additional review(s) within the clinic setting, for example, for adherence issues, polypharmacy or difficulty in controlling risk factors.
Review of clinic letters revealed that a variety of different interventions were recommended (table 2). These included: further investigations (most commonly a full lipid profile); a wide range of medication changes (including starting or stopping medicine classes, dose adjustments and/or switching between medicines); discussions around lifestyle (smoking cessation) or comorbidities (diabetes); and various types of onward referral. Some of these recommendations would have been actioned by the pharmacist (eg, requesting blood tests and other investigations) while others (eg, medication changes) would have been actioned in primary care, as per standard local practice. Independent pharmacist prescribers are able to prescribe medications, but local policy is for non-urgent medication changes to be recommended in the clinic letter for primary care to action. In eight cases (16%), the patient was discussed with the in-house cardiology team, for example, to gain advice on residual disease, red flag symptoms or ECG.
Interventions resulting from the post-MI medicines optimisation clinic
With regard to patient feedback, responses from the first 50 returned questionnaires are summarised in table 3. The majority agreed or strongly agreed that the clinic was friendly and welcoming (n=48/50; 96%); that they felt listened to (n=48/50; 96%) and reassured (n=45/50; 90%); that adequate explanation (n=47/50; 94%) and information (n=44/50; 88%) was given; and that clear plans were provided (n=45/49; 92%). Furthermore, the majority of respondents (n=44/50; 88%) agreed or strongly agreed that it was a valuable clinic and they would recommend it for patients with heart disease. Respondents were also asked to rate the clinic on a scale of 1 (very poor) to 5 (excellent). Forty-four patients (88%) rated it a 4 or 5 (table 3), and the mean score was 4.48.
Patient feedback on the clinic
Thirty-nine respondents provided free-text comments on what they liked best about the service. These fell into the following broad categories:
Helpful appointment and information delivered clearly, with their concerns addressed and their questions answered (n=29).
Friendly staff and good clinic environment (n=11).
Happy about waiting times (n=8).
Example comments included: ‘All my questions were answered in a clear, informative manner’; ‘Pharmacist took time to listen and explain what would happen in the future’; ‘Polite, efficient and well led. Given plenty of opportunities to discuss health and medications, seen on time in the clinic and given time in the appointment to ask questions’; and ‘Put my mind at rest regarding medication’.
A further 28 respondents commented on the free-text question about what they would like to see improved within the service. Of these, 19 said that no changes or improvements were required. Among the remainder, three individuals had concerns about waiting times. There was also feedback on wheelchair availability (n=1), using fewer acronyms in the clinic letter (n=1), preferring to see a consultant rather than a pharmacist (n=1), wanting more information about their heart condition (n=1) or the reasons for medication changes (n=1) and improving communication (n=1).
Discussion
This paper describes the principal steps required to upskill advanced clinical pharmacists to conduct independently run, person-centred medicines optimisation clinics for patients who have recently experienced an MI. By increasing the number of clinical pharmacists able to deliver these clinics, the service was made available to a greater number of patients with post-MI. Initially, capacity was doubled by the introduction of two advanced clinical pharmacists, with the consultant pharmacist stepping aside from day-to-day management of the post-MI clinic to develop other services (eg, a novel proprotein convertase subtilisin/kexin type 9 inhibitor clinic12). Additional personnel were subsequently trained, allowing the post-MI service to expand further.
Key elements of the upskilling process included a competency framework, individualised training plans and practice proformas for maintaining consistency of standards. Other centres wanting to implement a similar model could adapt much of this material according to local requirements; a training manual providing many of the required tools is available from the authors.
Analysis of clinic letters from patients attending our clinic suggested that it had a substantial impact on the quality of care provided (by helping to optimise patient management) and may also have improved safety (eg, by ensuring appropriate onward referral and reducing unnecessary polypharmacy). We have previously shown that a post-MI medicines optimisation clinic led by a more senior (consultant) cardiology pharmacist was well received by patients—and resulted in improvements in SPM optimisation, increased adherence and decreased readmission, and freed up cardiology outpatient clinic time.10
Our service addresses well-recognised issues in post-MI patient care. Indeed, previous analyses have shown that SPM prescribing is often suboptimal,3 5 with a recent European study finding that fewer than 60% of patients with post-MI were receiving recommended combinations of antihypertensives, statin, aspirin and antiplatelet agents.5 In addition, adherence with preventive medicines for cardiovascular disease is often low,6 despite the known links between reduced adherence, failure to achieve targets and inferior outcomes (including death).7 13 14 Thus, the benefits of our medicines optimisation service may be highly significant for patients and for the healthcare system as a whole and can be delivered without compromising safety.
Furthermore, there is growing evidence from other centres in the UK and elsewhere that pharmacist-led models of post-MI medicines optimisation can improve adherence and risk factor control, and that patients appreciate the opportunity such clinics provide for discussing and resolving care-related concerns.15–20
Our model also aligns with guidance on medicines optimisation from the UK’s National Institute for Health and Care Excellence, which highlights the importance of structured review, potentially led by a pharmacist when deemed locally appropriate.21 In addition, the upskilling of advanced clinical pharmacists to conduct these clinics in patients with complex needs fits with the concept of ‘advanced pharmacy practice’ advocated by leadership bodies such as the Royal Pharmaceutical Society.22
The model puts a high level of responsibility on the pharmacist leading the consultation, requiring them to take the lead in medicines recommendation and decision-making. This is a key difference from inpatient pharmacy practice and requires advanced training—but underscores the value of pharmacist independent prescribing in optimising patient care in cardiology.
In the present work, 84% of cases were managed solely by an advanced pharmacist. Nonetheless, although our clinic is driven primarily by pharmacists, it remains fully multidisciplinary and patients have access to a cardiologist whenever necessary. This is particularly important for individuals presenting at the clinic with cardiac symptoms. Service-level guidance was already in place regarding which patients should be escalated to a consultant pharmacist or to a consultant cardiologist, but the existing triage criteria were reinforced to ensure appropriate management. Generally, patients were invited to attend the medicines optimisation clinic if they are not awaiting further revascularisation or ischaemia testing, but inevitably some develop new symptoms between hospital discharge and clinic attendance, necessitating assessment and escalation of those with ‘red flags’. In collaboration with consultant cardiology colleagues, a referral pathway was therefore developed based on various presentations of five cardinal symptoms: chest pain, breathlessness, palpitations, peripheral oedema and dizziness/syncope.
An important aspect of building the advanced clinical pharmacist-led model was to develop their clinic-based consultation style. Key aspects of the consultation include: careful tailoring to individual patient needs; the use of open questions to encourage sharing of concerns; taking time to listen to and acknowledge patients’ views about their condition and their medicines in a non-judgemental manner; holistic discussion of the benefits and risks of treatments; and provision of accessible and understandable information. In line with current guidance,23 patients should also be given an opportunity to take part in decision-making around their medicines (although the level of involvement may vary depending on their personal preferences). The consultation should conclude with a summary that reiterates key points, reinforces the agreed action plan and checks patient understanding.
Patient feedback on the model was highly positive based on 50 anonymously completed questionnaires. Some had previously lacked understanding of the roles of pharmacists beyond dispensing medicines and were initially apprehensive about a pharmacist-led consultation. However, most patients were grateful for the opportunity to have an open and honest discussion—and almost all respondents ultimately had no significant concerns about seeing a pharmacist rather than a cardiologist. The overwhelming majority said that they had been listened to and that their medicines-related concerns were addressed, felt involved in decision-making and considered that the clinic provided them with a clear plan about their medicines. Furthermore, these patient–practitioner relationships became progressively more constructive as the advanced clinical pharmacists gained experience and their consultation style developed.
We must acknowledge the limitations of the present work. In particular, the patient feedback results were based on a retrospective review of data from a modest number of questionnaires (n=50). Furthermore, we cannot rule out the possibility that individuals who were satisfied with the clinic were more motivated to provide feedback than those who were not, which could have biased the results. However, anecdotally, we have not had significant amounts of negative feedback around this clinic model. Nonetheless, it would be valuable to undertake a prospective, randomised trial to compare our service versus a more ‘standard’ model of post-MI medicines optimisation in routine practice. We should also acknowledge that a pharmacist-led model of medicines optimisation would not be possible in some countries—particularly those that do not allow non-physician prescribing or where the clinical pharmacist role is less well developed.
Conclusions
We have demonstrated that a person-centred post-MI medicines optimisation service can be delivered by appropriately trained advanced cardiology pharmacists with support from the multidisciplinary team. A structured competency framework and training programme are required to facilitate development of the required knowledge and skills. However, once that has been completed, the model is highly valued by patients and offers potential to improve adherence and provide greater control of cardiovascular risk factors, while reducing the overall burden on busy cardiology outpatient clinics.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
We thank the Biological Communications Limited for medical writing support.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrRaniKhatib
Contributors The project steering committee who overlooked the project was composed of RK (project lead), AH, CP, GM and UL. The delivery of the service, the collection of data and analysis involved RP, FW, RK and AH. The article was planned by RP and RK. FW contributed to the article content. All authors reviewed the paper and made suggestions and amendments around content. RK is the guarantor.
Funding Funding for the proof-of-concept phase of the service was partly funded by AstraZeneca within a joint working agreement. The success of this phase led to the service being fully commissioned by the Leeds Clinical Commissioning Groups and it became the new standard service offered for our patients with myocardial infarction.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.