Article Text

Abstract
Teledermatology is an important subspecialty of telemedicine that continues to evolve with advances in telecommunication and mobile phone technology. A 19-week primary care quality improvement project collected baseline data and tested three change ideas, using the Model for Improvement method, with primary and secondary aims: to increase the weekly percentage of remote dermatological consultations with supporting images that were successfully concluded remotely to greater than 80% and to reduce the weekly percentage of dermatological face-to-face consultations to less than 50%. We hypothesised that by improving the quality of patient images and the confidence of reception staff in triaging skin complaints, there would be a decrease in the weekly number of face-to-face dermatological appointments, thereby decreasing the risk of COVID-19 transmission within the practice and community. Two change ideas focused on supporting patients to improve image quality by introducing ‘4 Key Instructions’ and a patient information leaflet (PIL). The third focused on increasing reception staff confidence in triaging skin complaints by introducing a triage pathway guidance tool. A total of 253 dermatological consultations were analysed: 170 of these were telephone consultations with 308 supporting images. Process measures showed clear improvements in the quality of images provided by patients which likely contributed to an increase in completed remote consultation. Our primary outcome measure was achieved. Our secondary outcome measure suggested that in the absence of high-quality images, it might not be possible to reduce dermatological face-to-face consultations much below 50% in primary care. Process measures showed clear improvements in the quality of images provided by patients which likely contributed to the increase in remote consultation. The implications of these findings for the theory of change are discussed.
- Healthcare quality improvement
- GENERAL PRACTICE
- Control charts/Run charts
- COVID-19
- Patient safety
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic?
Teledermatology has been the subject of recent reviews, practice guidelines and position statements. General practitioners (GPs) can make a correct diagnosis in up to two-thirds of images taken by a dermatologist. Our aim was to maximise the ability of GPs to make a dermatological diagnosis based on images taken by patients.
What this study adds?
We show that over 80% of dermatological consultations in primary care can be dealt with remotely if patients provide high-quality supporting images.
How this study might affect research, practice or policy?
Dermatologists now routinely request images as attachments to referral letters to aid in decision-making in secondary care. Our project extends this practice to primary care by showing that good quality images taken by patients can improve decision-making by GPs.
Problem
Teledermatology is an important subspecialty of telemedicine that continues to evolve with advances in telecommunication and mobile phone technology.1 Patients with skin disorders, which account for over 13 million primary care consultations each year,2 3 have been targeted for this new way of working, as the skin is uniquely visible to the naked eye. The COVID-19 pandemic has led to several changes to the way we deliver healthcare, none more so than in general practice which has made every effort to reduce contact between staff and patients by efficiently triaging and switching to consultation by telephone.4 The use of smartphones to send clinical images was a new concept for our medical practice: a 3836-patient teaching general practice in a rural Galloway town in Southwest Scotland. During the first wave of the pandemic fewer than 60% of the weekly dermatological consultations with supporting images were dealt with remotely and 67% of all dermatological consultations were seen face-to-face. We felt this was likely because of inappropriate triage or after an unsatisfactory telephone consultation with poor quality supporting images. Accurate dermatological diagnosis cannot be achieved without high-quality images, and it is therefore in everyone’s interest to improve this.5 Remote consulting may also improve patient experience in other ways: not only by reducing travel time and time spent waiting for an appointment but also by widening access to specialist care for patients who live in rural areas.6
Specific aims
The primary aim of our quality improvement project was that by 15 April 2021 more than 80% of weekly dermatological consultations with supporting images should be diagnosed and dealt with remotely, in keeping with COVID-19 guidance from Health Protection Scotland.4 Secondary aims were to reduce all dermatological face-to-face consultations to less than 50%; to improve the quality of supporting images; and to improve the confidence of reception staff. We hypothesised that by improving the quality of patient images and the confidence of reception staff in triaging skin complaints, there would be a decrease in the weekly number of face-to-face dermatological appointments, thereby decreasing the risk of COVID-19 transmission within the practice and community.
Background
Teledermatology has been the subject of recent reviews, practice guidelines and position statements.1 7–10 There are two main methods for its delivery: first, ‘store-and-forward teledermatology’ where images are received and sent to a dermatologist to be reviewed asynchronously; and second, ‘real-time teledermatology’ where there is synchronised delivery of consultation and diagnosis between physician and patient remotely.1 Restrictions imposed by the COVID-19 pandemic have further increased its application and use as a tool for the rapid and effective diagnosis of skin disorders.11 Recent reports have shown that a self-selected group of general practitioners (GPs), looking exclusively at photographs taken by a dermatologist using a Samsung J7 smartphone, were able to make a correct diagnosis in 64% of skin lesions.3 In another study, patient images which were taken by GPs using specialist magnifying devices and sent to a consultant dermatologist, were assessed within 48 hours. The Leeds dermatology service found it was possible to deal with 67% of 12 294 skin referrals in this way.12 Kroemer and colleagues compared the diagnostic accuracy of clinical and dermoscopic images from 113 skin tumours with face-to-face examination and histopathology. They found that 104/113 (92%) skin tumours could be evaluated in this way and that a diagnosis based on imaging alone was correct on 84% of occasions.13 It is against this background that we chose to assess the ability of GPs to make a dermatological diagnosis based on images submitted by patients. To our knowledge, this approach has not been published before.
Measurement
We defined measurements as outcome, process or balancing as follows:
Percentage of dermatological patients who sent in supportive images that were diagnosed/dealt with remotely (primary outcome).
Percentage of dermatological patients seen face-to-face (secondary outcome).
Percentage of dermatological patients who sent in images with acceptable framing (process).
Percentage of dermatological patients who sent in images that used a scale (process).
Percentage of dermatological patients who sent in images where the anatomical location was obvious from the images alone (process).
Percentage of dermatological patients who sent in at least one image that was well focused (process).
Reception staff confidence level in triaging dermatological patients (process).
Time of average telephone interaction between reception staff and patient booking an appointment for a skin complaint (balancing).
Patient feedback response to patient information leaflet (PIL) questionnaire (balancing).
Analysis
Data were collected weekly by reviewing Egton Medical Information Systems (EMIS) and Docman records and used to create run charts to monitor change over time. Patient feedback was used to assess the helpfulness of the PIL and gauge the population’s engagement with smartphone use. Reception staff confidence levels were measured using a 10-point Likert scale to evaluate more subtle differences between staff.
Baseline measurements
Three baseline measurements were completed over 6 weeks between November 2020 and January 2021. The first used the EMIS appointment system to identify the weekly number of dermatological appointments. The percentage of dermatological consultations with supporting images that were dealt with remotely and the percentage of all dermatological consultations that were seen face-to-face were plotted on run charts so that outcome data could be monitored weekly. The second baseline measurement was an assessment of patient-sent images. We used ‘4 Key Instructions’ to judge their quality, based on UK Guidance on the use of mobile photographic devices in dermatology.5 Patient images were assessed for framing, flash, scale, focus and plotted as a percentage on separate run charts. The third baseline measurement used a reception staff questionnaire to assess reception staff confidence in triaging skin complaints. A Likert scale allowed for more subtle differences compared with a yes/no answer and found an average of 7.5/10 (10 the more confident).
Design
We formed a quality improvement group which included a medical student (KJ), a GP (EL) and a receptionist (KM). AMillar provided quality improvement methodology coaching. We used the Model for Improvement (MfI) as the framework for testing change.14 Qualitative data and analysis of patient records highlighted the challenges of the move to telephone consulting. We witnessed at first hand staff frustration with the number of no or poor-quality images being sent to support telephone consultations. Face-to-face appointments had to be arranged as a result, many of which contributed to unnecessary patient–staff contact during the second wave of the pandemic. Several quality improvement tools (fishbone diagram, process mapping, stakeholder analysis (online supplemental material slides 3–5) were used to analyse the problem.15 A driver diagram (online supplemental material slide 6) articulated our theory of change and helped make decisions regarding the following key change ideas:
Supplemental material
Provide key instructions for staff to give to patients to improve image quality.
Introduce a PIL to support patients to take good-quality images at home.
Improve reception staff confidence in triaging dermatological patients.
Strategy
Interventions
The diagnostic work completed with stakeholders generated three main change ideas which are included in the driver diagram. The aim of the first change idea was to standardise, and therefore improve, images sent in by patients to support their telephone consultation by encouraging reception staff to provide the same ‘4 Key Instructions’ to patients. The instructions focused on the following:
Framing—asking the patient to take at least one image up close and one further away.
Flash—educating the patient that a flash can help produce a sharper image, but not to use too close.
Focus—asking them to allow time for the camera to engage in auto-focus.
Scale—encouraging the use of a ruler or a coin to help determine size.
The second change idea aimed to create a PIL comprising the ‘4 Key Instructions’ alongside study rationale and disclaimer. We posted the PIL on the practice website, Facebook and waiting room television to reach a wider audience.
For the third change idea, we aimed to improve confidence of reception staff triaging skin complaints by introducing a triage pathway, with help from the pharmacy team who had previously implemented a change project based on the Pharmacy First Scheme.16 Triage guides that included examples of different skin conditions were placed in reception. We used a questionnaire with a Likert scale to assess whether this had been successful.
Study of the interventions
Using the MfI we established three series of plan-do-study-act (PDSA) cycles, each focused on a change idea within the driver diagram and assisted with problem solving when carrying out small scale testing
PDSA series 1: defining better images
The purpose of our first cycle was to determine whether making a small change to conversations between receptionists and patients calling to book an appointment, would improve the quality of images. Advice aimed at health professionals on taking high-quality images5 was adapted to help patients take optimal images at home. In this way we hoped to support a seamless switch to telephone consulting by increasing clinician likelihood of an accurate diagnosis remotely.5 This small-scale change was tested by obtaining opinions and approval of the ‘4 Key instructions’ from consulting staff in the practice (doctors, advanced nurse practitioners and medical students).We then created a colour poster for reception staff, highlighting the ‘Scale’ instruction as probably the most useful advice for patients. We displayed the poster in reception to act as a visual reminder. After 1 week of testing, we found that less than half of dermatological telephone consultations included patient sent images and so it was decided that all clinical staff, who were also booking patient appointments should be encouraged to promote the ‘4 Key Instructions’ alongside the receptionist. During the second week of testing, we found that a greater number of images and higher quality of images had been submitted.
PDSA series 2: PIL
Our receptionists suggested that patients might not be retaining verbal information, for example, if they phoned from their car or work. Our PIL therefore aimed to provide patients with a tool to understand how to better participate in their own care. The PIL was adapted from NHS Forth Valley PIL for patients attending skin photography clinics.17 Further helpful feedback from clinical staff, improved the original leaflet design by prompting patients for extra data (name, date of birth, site, symptoms) and modifying the disclaimer paragraph. Several different formats were created based on the leaflet design and posted, on separate test weeks, on Facebook, practice website and waiting room television. We learned that the Facebook page could reach a high volume of patients quickly and this inspired posting on the practice’s webpage as a permanent source to signpost patients. Patients entering the branch dispensing practice for prescriptions were targeted for feedback.
PDSA series 3: receptionist confidence in dermatological triage
Our third cycle of change was designed to improve receptionist confidence in dermatological triage by introducing a triage pathway. The practice pharmacy team helped refine the pathway by suggesting common conditions that could be signposted to pharmacists and commented on the need for brief clinical descriptions for non-medical understanding. Using a red, amber, green traffic light system we encouraged the receptionist to decide if the patient had an urgent problem (red)—for example, a widespread rash with breathing difficulties or red-hot shiny skin—and direct them to accident and emergency or a same day face-to-face appointment. If the problem was non-urgent (green)—for example, cold sores, itchy scalps, fungal nail—they were asked to signpost to pharmacy. Our triage pathway further advised that routine complaints (amber)—for example, inflammatory skin conditions, other skin lesions and rashes—should be offered a telephone consultation with supporting images. If the patient was unable to provide images, or the complaint was in a sensitive area, a routine face-to-face appointment should be arranged first. The triage pathway was shared with reception staff in the last 3 weeks of testing.
Our failure to reduce dermatological face-to-face appointments below 50% despite sustained image quality triggered revision of our change theory with probable influence from cultural and environmental factors as lockdown restrictions eased. However, all receptionists found the tool helpful, and we learned it could replace verbal handover of tasks for new staff to feel confident.
We recognised that certain dermatological presentations must be seen face-to-face to ensure safety and dignity. The practice thus continued to have a low threshold for seeing patients, the interventions acting as an aid in decision making. Further, because it was new for the practice using photography in this way, we had to consider image storage and confidentiality.18 For this reason, the informative disclaimer paragraph was added to the PIL.
Primary outcome measure: percentage of dermatological patients who sent in supportive images that were diagnosed/dealt with remotely
Figure 1 is a run chart showing the percentage of dermatological telephone consultations with supporting images that were managed over the telephone. Telephone consultations with no supporting images were excluded from these data. Where images are provided by patients, the change ideas that improve the quality of images and receptionist confidence are associated with an increasing proportion of consultations being managed via the telephone alone. The goal of increasing the percentage of patients with supporting images who were dealt with remotely to more than 80% was met on 11 of 13 improvement weeks (averaging 6 patients/week).
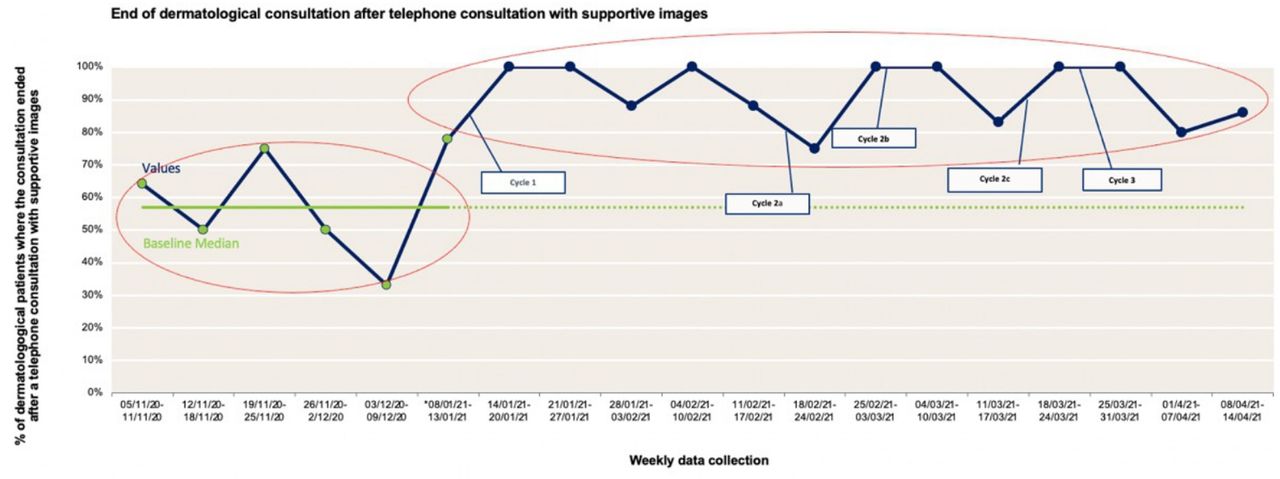
Percentage dermatology consultations that ended after a telephone call with supporting images. Data shown are based on the 115 consultations that were dealt with by telephone and accompanied by images.
Secondary outcome measure: percentage of dermatological patients seen face-to-face
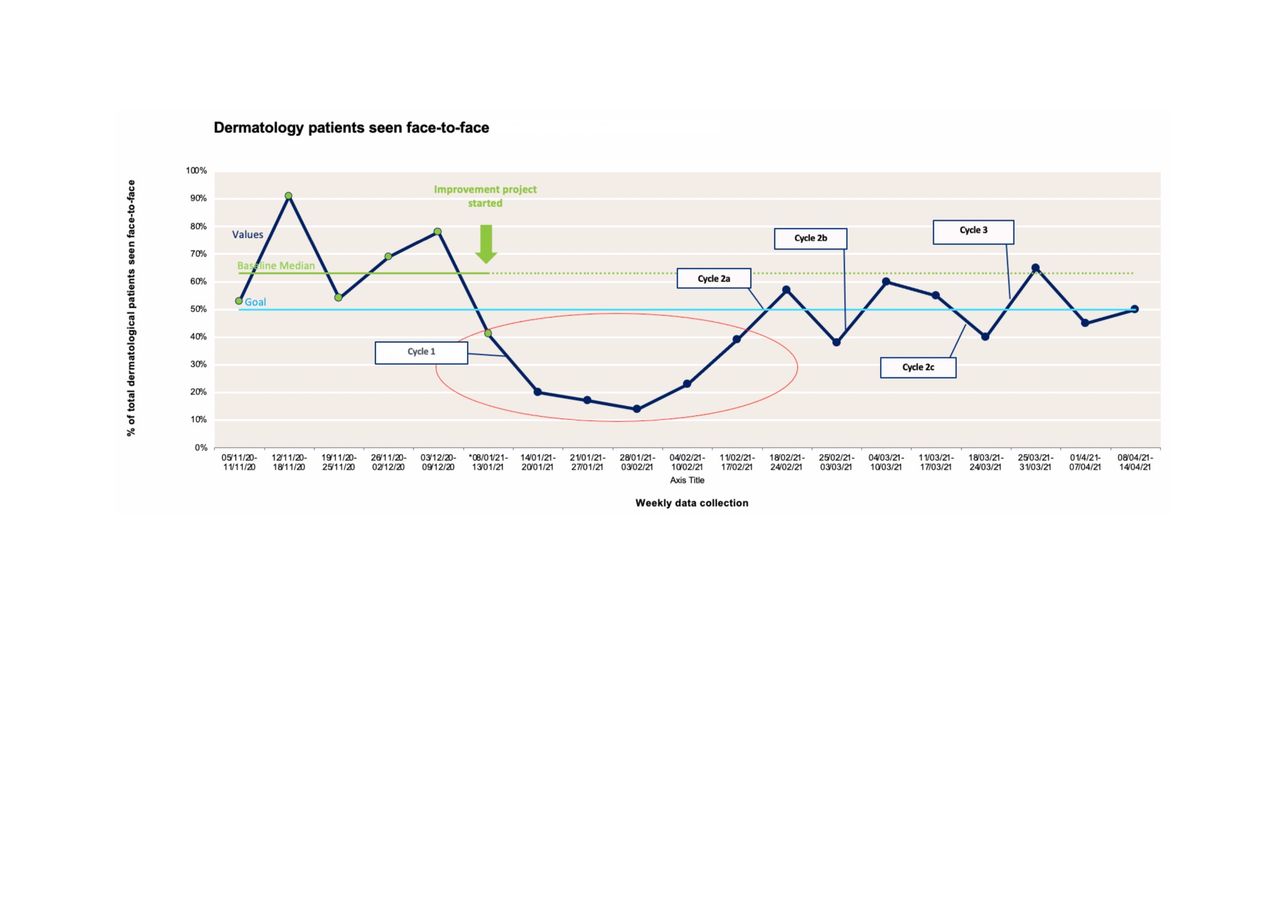
Figure 2 is a run chart showing the percentage of dermatological patients seen face-to-face weekly. These data include patients who did not send supporting images. The green points represent baseline data, the green line the baseline median (63%) which was frozen and extended to detect variation early. The blue line represents our aim that fewer than 50% dermatological referrals should be seen face-to-face. The change ideas were associated with reduced percentage of patients being seen. The largest fall in face-to-face consultations occurred after the introduction of the ‘4 Key Instructions’. Thereafter we observed a fluctuating pattern in the proportion of patients seen face-to-face with no clear further improvement following cycles 2 and 3. The goal of reducing weekly face-to-face appointments below 50% was met on 9 out of 13 improvement weeks (averaging 13.5 patients/week).
{kind=link}
{kind=link}
Percentage dermatology consultations that took place face-to-face. Data shown are based on 122 consultations, 83 of which were seen face to face initially and 39 of which took place first by telephone.
Process measures
Patient images were assessed individually and showed an improvement in image quality when compared against baseline data (table 1).
Process measures before and after interventions. Data shown are based on the 170 consultations that were dealt with by telephone initially, 115 of which were accompanied by images
Receptionist confidence in triaging dermatological patients increased from an average of 7.5–9.2 on a 10-point Likert scale with 100% (5/5) of reception staff agreeing that the pathway guide was helpful. One staff comment expressed: ‘regardless of length of time working here—a great tool for support and training’.
Balancing measures
The time taken to complete a phone call between receptionist and patient booking a dermatological appointment had no adverse effect on time pressures for receptionists, the most accessible members of the team.19 Most reception staff said the phone call lasted less than 3 minutes prechange and postchange. Twenty-seven patients, ages ranging from 24 to 86 years, were targeted over a single day for feedback via a questionnaire on the PIL. Results confirm its value as a helpful resource: 25/27 said they found the leaflet helpful, 27/27 found the leaflet easy to understand and 24/27 said they had access to a smartphone. When asked ‘where would you prefer to access this information?’, and given the option of more than one answer, the 27 patients responded as follows: leaflet (11), Facebook (10), website (8) and waiting room television (6).
Discussion
Interpretation
Our primary outcome measure shows that telephone consultations with supporting images enabled over 80% of weekly dermatological patients to be managed remotely. Our secondary outcome measure suggests that if patients do not send high-quality images, then it may not be possible to reduce dermatological face-to-face consultations much below 50% in primary care. Our process measures show significant improvement in the quality of patient sent images and an overall increase in staff confidence level in dermatological triage. Face-to-face appointments were still sometimes necessary, even with supporting images. For example, one patient had expressive dysphasia which meant difficulty communicating over the telephone. Another patient was brought in for a face-to-face consultation to rule out a deep vein thrombosis.
In the first months of 2021, the practice was operating restricted services due to local lockdowns associated with the number of COVID-19 in the community and potential impact on healthcare staff. Some of the main considerations included controlling access to the practice by locking doors, sending prescriptions to the chemist instead of patients collecting them, encouraging remote consulting unless absolute necessary, and stopping all non-essential practice activity. It is likely therefore that the initial reductions in face-to-face consultations seen in figure 2 were associated with these measures rather than the change testing. The results of this quality improvement project strongly suggest that the driver diagram should be revisited. Greenhalgh and colleagues20 have recently published a qualitative study related to video consultations in primary care. Work should be undertaken to explore drivers for change in teledermatology. For example, factors such as changing infection control measures, climate conscious choices and clinical job satisfaction may be underplayed in the project reported here. Future quality improvement projects should explore these drivers.
Lessons learned
Our quality improvement methodology taught us that identifying key stakeholders early was crucial to the project’s development. To make a sustainable change in healthcare systems stakeholders with a vested interest in change must be approached.21 It also encouraged a ‘show me’ approach to problem solving which benefited staff engagement. Mapping the ‘ideal’ patient journey, from initial phone call to end of consultation, created a process map template that could be edited as insight into the system developed. The map identified discrepancies within the current system and thus targeted areas for change. The fishbone diagram helped brainstorm further probable causes, but implied they were equal in cause.22 However, recognising primary and secondary drivers meant we could guide change testing based on the prospective impact on the system. The PDSA iterative method allowed for quick assessment and adaption of the changes in a busy clinical environment.23
The first test of change assessed whether verbal instructions would improve image capture. We selected four of the nine photography tips from teledermatology guidelines5 so as not to overwhelm patients with too much information. Cognitive tasks can only be completed successfully if instructions are held as they are processed, and this working memory capacity can be as low as three to five items.24 To maximise provision of the ‘4 Key Instructions’, receptionists were asked to document the date of the telephone conversation and each patient’s community health index number as they gave the instructions over the phone. Daily repetition created strong learning and promoted behavioural change.25
It is possible that patients who did not send images were in situations that did not allow retention of instructions (eg, phoning from work). A PIL allowed an alternative form of communication. We did not think it would be feasible to send all patients a leaflet by post, so instead the design was edited and posted on the waiting room television, website and Facebook. The Facebook page, with 550 likes and 584 followers, showed we could reach a large proportion of patients in a short period of time. Furthermore, our project was discussed at a regional meeting of primary care colleagues who expressed a desire to share the PIL and posters within their own practices.
The red-amber-green pathway was welcomed by reception staff who said it gave them confidence regarding the decision whether a patient required to be seen face-to-face or not. The pathway acted as an effective way of communication, the most important factor for organisational change,26 and empowered staff to adopt new ways of working in response to the challenges created by COVID-19. Comments on the booking system like ‘unable to send pics’ show reception staff have offered the patient a telephone consultation and justifies face-to-face appointments. However, the data from this project does not support this as a key change that influences the outcome measure.
We recognise that it may not be possible to reduce dermatological face-to-face consultations to below 50% in primary care. A survey of 829 GPs across the UK in early July 2020 found that 61% of all appointments were being conducted by telephone with only 11% by face-to-face (the rest remotely as either telephone triage, video, email or SMS).27 By the end of July 2020, the Royal College of General Practitioners Research and Surveillance Centre reported an increase in face-to-face appointments to 40% in England.27 Eighty-eight per cent of 622 GPs in September 2020 felt that face-to-face appointments were key to forming trusting patient–doctor relationships.28 GPs have been following guidelines to work remotely wherever possible, but an increase in face-to-face consultations towards prepandemic levels seems inevitable as lockdown restrictions are relaxed.
Good quality dermatological images can benefit patient care in other ways, for example, by facilitating a useful baseline from which to measure disease change over time such as for atypical melanocytic lesions as recommended by the National Institute for Health and Care Excellence.29 Teledermatology can also assist the assessment of skin disorders in secondary care, as already discussed.12 Evidence suggests cost savings in consultant time and material costs of unnecessary procedures.12 Teledermatology will likely persist as an alternative to face-to-face as general practice pressures rise. Some will always prefer to be seen face-to-face by a doctor, whatever their complaint, though for many patients it seems likely that skin disorders are uniquely suited to remote consultation if accompanied by high quality images.
Application of learning
As system pressures increase, the dermatologists in Dumfries and Galloway now request images as attachments to all referral letters to aid in decision-making in secondary care. The quality improvements described in this paper may help general practices in the region to increase the number of high-quality images submitted by their patients.
Limitations
We felt it was important to gain patient feedback for the PIL, but on reflection a larger patient sample would have been preferable as only 27 (less than 1%) of 3836 patients were approached. The leaflet was introduced as a student project which may have increased engagement by patients who wanted to be supportive. Presenting outcome measures as weekly percentages in run charts may be a limitation because the variation in data points often represented a difference of only one or two patients.
The study design did not permit analysis of whether the ‘4 Key Instructions’ and PIL were equally useful and effective regardless of skin colour. Finally, the project timescale meant that the third pathway had limited test time and possibly contributed to triage behaviours not being sustained.
Conclusion
We have shown that over 80% dermatological consultations in primary care can be dealt with remotely if patients provide high-quality supporting images. It seems likely that patient education to provide better quality images, a PIL and measures designed to increase the confidence of reception staff when triaging skin complaints contributed to this improvement. We recognise however that in the absence of high-quality supporting images it may not be possible to reduce dermatological face-to-face consultations below 50% in primary care.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Approval for the project was sought and granted by the practice’s Caldicott Guardian. We did not seek ethical approval as no patient identifiable data were included in our analyses, in keeping with our health board’s policy. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to extend our thanks to the entire medical practice team who helped facilitate the project and provided feedback enabling change.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KJ healthcare quality improvement project lead and guarantor. Participated in project design, research, tests of change, data analysis, drafting and editing of paper. EL participated in project design, data analysis and facilitated tests of change. KM participated in project design and facilitated tests of change. AMillar provided quality improvement methodology coaching, and review and editing of the paper. CI cowrote the second draft and helped edit subsequent drafts. AMcFadyen provided statistical analysis. HS provided critical review and editing of paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.