Article Text

Statistics from Altmetric.com
Introduction
Appropriate handling of ‘critical’ laboratory test result values is an essential component of timely, quality patient care. While interinstitutional variability exists,1 critical values have historically been defined as potentially ‘life-threatening’ if not attended to quickly,2 necessitating prompt notification of a responsible clinician. Given patient safety implications, timely communication of results to a provider is a common regulatory element, including: (1) Joint Commission patient safety goals,3 (2) Clinical Laboratory Improvement Amendments4 and (3) the International Organization for Standardization.5 Inpatient values comprise a significant proportion of notifications,6 and among inpatients, oncology inpatients typically constitute a substantial volume.7
After laboratory result generation, contacting a responsible clinician can be complicated by multiple barriers. Previous approaches to improve this process include using call centres, automatic pager notifications and automatic personal digital assistant (PDA) telephone notifications.8–11 In our hospital, the inpatient haematology/oncology/stem cell transplantation (H/O) service had an overall notification success rate substantially lower than the hospital average as an effect of the large volume of critical results that typically returned in a short time period at certain times of day, leading to a multidisciplinary initiative to improve the notification process.
Methods
In our free-standing 360-bed paediatric hospital, ‘overall’ successful critical result notification must: (1) be acknowledged by a licenced individual provider (LIP) and (2) meet criteria for ‘timely’ notification, indicating that both outgoing notification from the laboratory/call centre and LIP acknowledgement occur within 30 min of result generation. H/O inpatients account for 15%–20% of all inpatient critical values but had a significantly lower overall successful notification rate than the hospital average. Timely outgoing notification occurred >90%, but timely LIP acknowledgement was <5% for H/O inpatients.
A multidisciplinary group with representatives of the H/O division, call centre, laboratory and patient safety analysed key drivers. Our group aimed to increase the overall successful notification rate to >40%–50% (the hospital-wide success rate) within 6 months of implementation. Process analysis demonstrated difficulty identifying appropriate LIPs and having efficient closed loop communication with them, especially during early morning hours.
We aimed to address multiple drivers simultaneously with one intervention: using hospital-owned smartphones designated for specific inpatient teams, smartphone messaging was used for both the outgoing notification and subsequent LIP acknowledgement. Using a privacy-compliant smartphone messaging programme present on their computers, laboratory and call centre personnel transmitted manually acquired screenshots of critical values, reference ranges and patient identifiers directly to LIPs caring for H/O inpatients, and LIPs acknowledged receipt via a return message through the same messaging system. Phones were assigned to inpatient clinician teams as a group, rather than specific providers, eliminating the need for laboratory and call centre personnel to search for individuals to message. Phones were already present on the unit, as they are also used as the primary communication device by nursing staff and systems for their maintenance and storage were therefore already in place. A group of LIPs received training and written materials on the new system prior to its implementation by members of the implementation group and were expected to inform and train subsequent new team members themselves, as part of orientation to the role. Run charts were used to track the proportion of successful notifications for inpatient units.
Our Institutional Review Board determined this project did not meet the definition of human subjects research. This manuscript was prepared using SQUIRE 2.0 guidelines. The public was not involved in project design due to its focus on internal communication.
Results
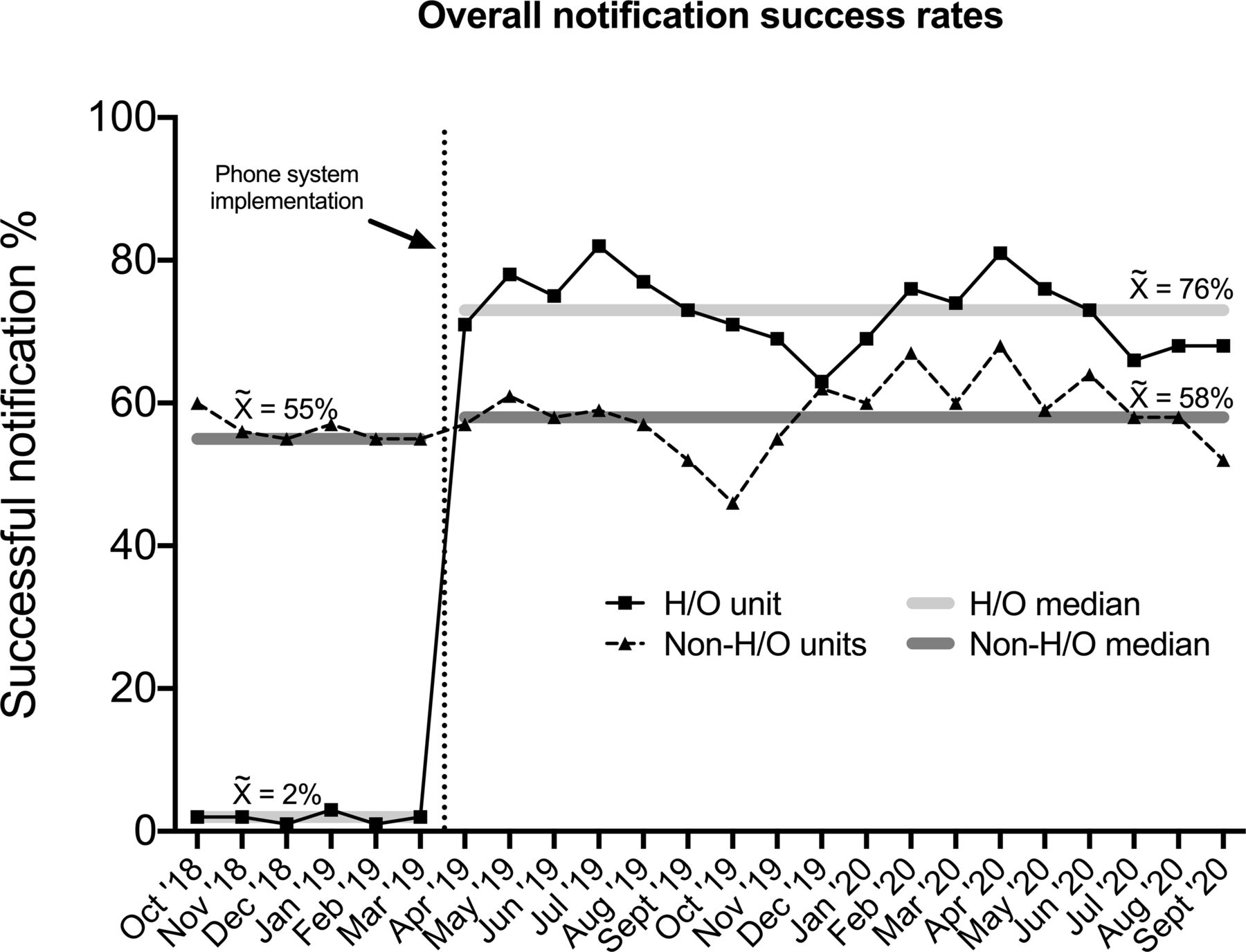
Preimplementation, median monthly overall success rate for H/O inpatient notifications was 2%, while the median for all non-H/O units was 55% (see figure 1). After implementation of the new system on 1 April 2019, the overall success rate for H/O increased from 2% to 71% in a 1-month period. The median overall success rate for H/O has been 76% since implementation, while the median for all non-H/O units has remained 58% (figure 1). A decrease in overall success rate was seen in late 2019 that was posited to be due to a combination of a need to retrain frontline providers (including new resident physicians) as well as an increase in hospital-wide patient volumes, leading to an increased number of patients on the H/O unit that were being cared for by non-H/O services and thus not participating in the phone intervention. New training sessions were provided for frontline providers around the same time period as patient volumes diminished and overall success rates subsequently increased.
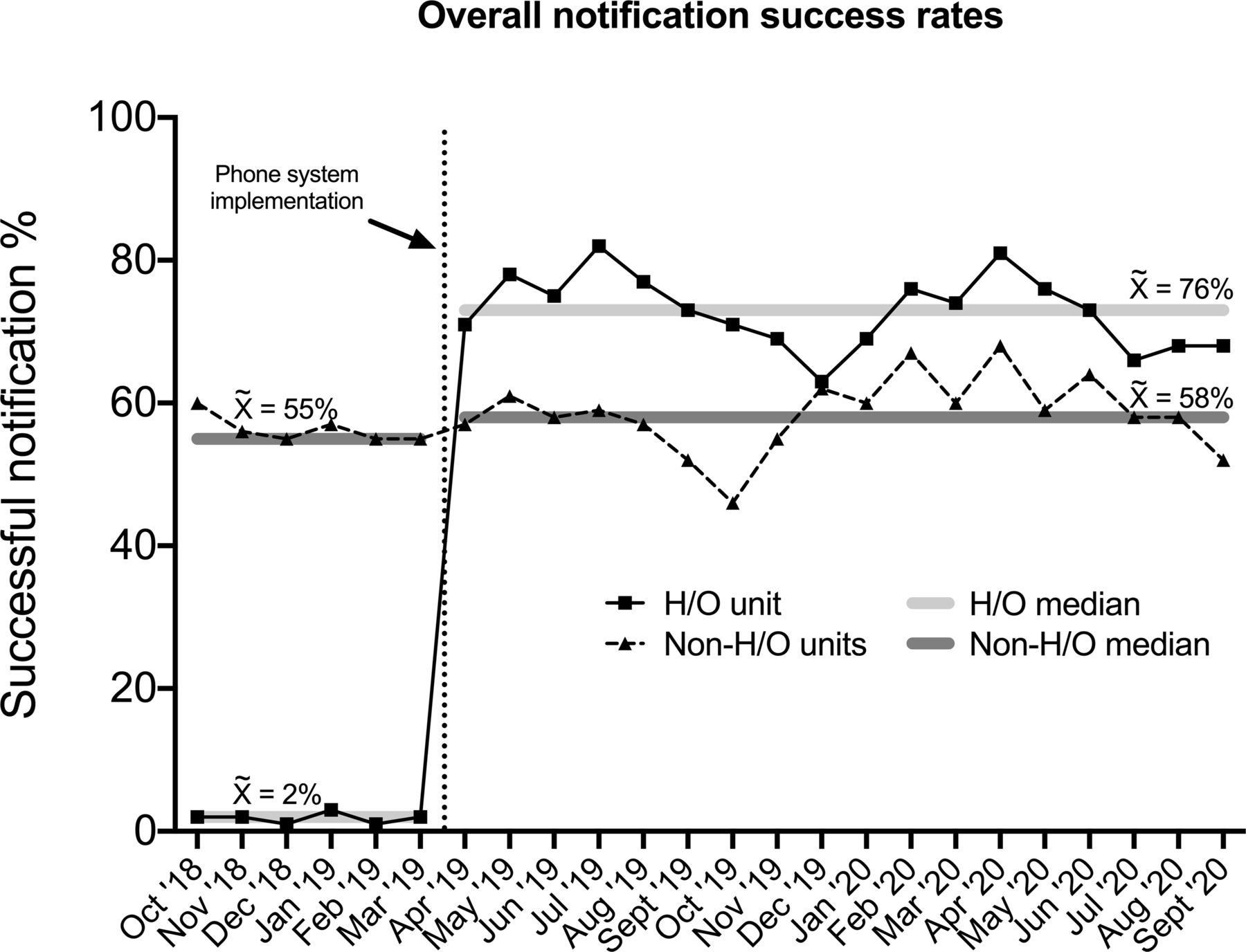
Overall success rates for notification of critical laboratory values for haematology/oncology (H/O) inpatients is increased with use of a smartphone-based communication system. The percentage (calculated per month) of critical value notification results that were successfully received and acknowledged by licenced individual provider (LIP) in the appropriate 30 min time period are indicated by the lines with monthly symbols (squares/solid line indicating H/O notifications and triangles/dashed line indication for the rates for all non-H/O units in aggregate) with the percentage indicated on the left-hand y-axis. The median ( ) success rates for the H/O unit (light grey horizontal bar) and the non-H/O units (dark grey horizontal bar) both before and after the intervention are as indicated. The vertical dotted line indicates the time point when the new notification system was implemented.
) success rates for the H/O unit (light grey horizontal bar) and the non-H/O units (dark grey horizontal bar) both before and after the intervention are as indicated. The vertical dotted line indicates the time point when the new notification system was implemented.
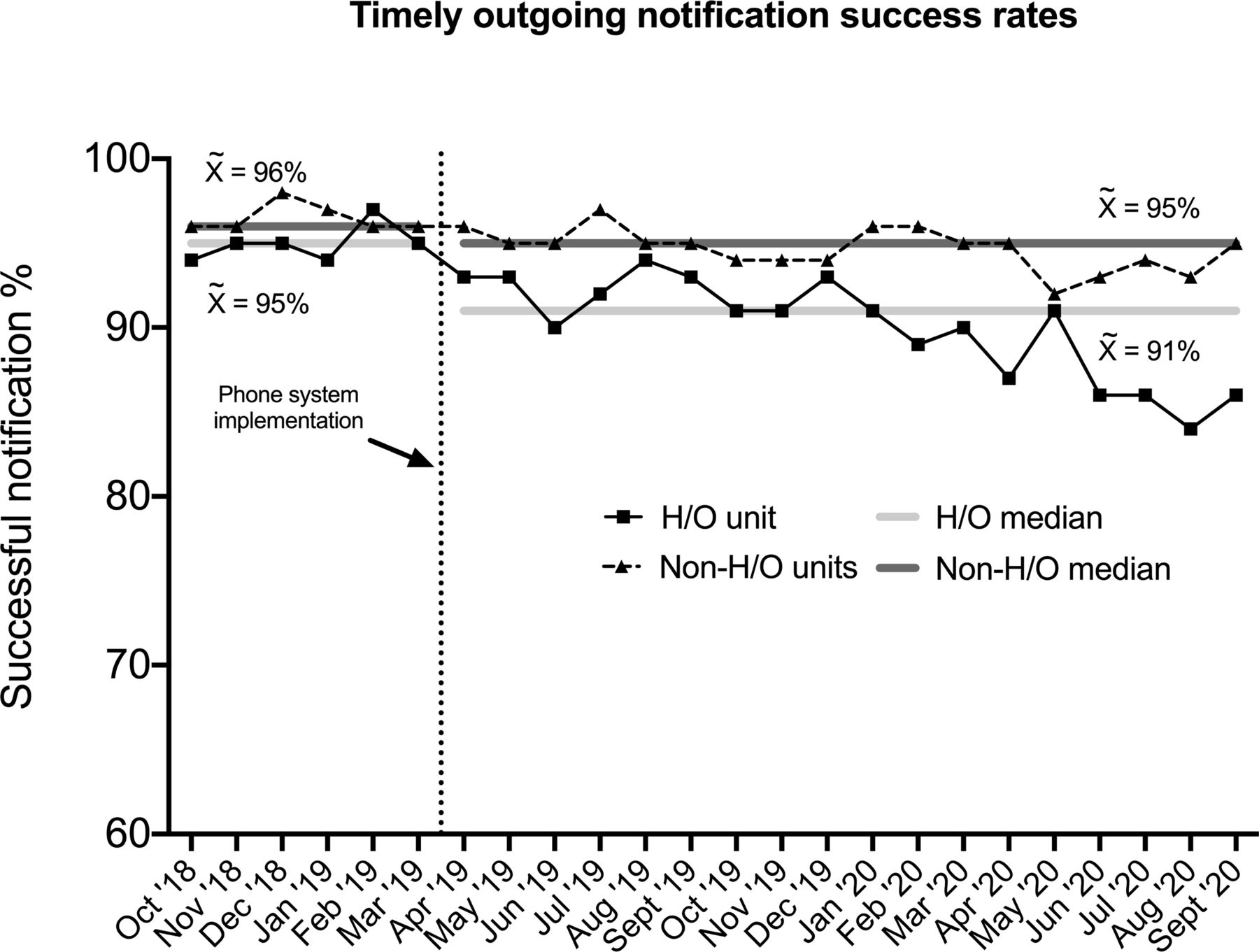
The percentage of timely outgoing notifications was tracked as a process measure and demonstrates a small but sustained decrease for H/O patients (from 95% preimplementation to 91% postimplementation, see figure 2), compared with 96% and 95%, respectively, for non-H/O units. No difference was seen before and after our intervention in the frequency of assessments by Intensive Care Unit (ICU) teams of H/O patients for transference of their care to the ICU (data not shown).
{kind=link}
{kind=link}
Implementation of a smartphone-based communication system for critical laboratory values is associated with a decrease in timely outgoing notification generation. The percentage of outgoing notifications of critical laboratory values that were successfully generated within 30 min (calculated per month) are indicated by the lines with monthly symbols (squares/solid line indicating H/O notifications and triangles/dashed line indicating the rates for all non-H/O units in aggregate) with the percentage indicated on the left-hand y-axis. The median ( ) success rates for the H/O unit (light grey horizontal bar) and the non-H/O units (dark grey horizontal bar) both before and after the intervention are as indicated. The vertical dotted line indicates the time point when the new notification system was implemented. H/O, haematology/oncology.
) success rates for the H/O unit (light grey horizontal bar) and the non-H/O units (dark grey horizontal bar) both before and after the intervention are as indicated. The vertical dotted line indicates the time point when the new notification system was implemented. H/O, haematology/oncology.
Discussion
Using hospital-owned smartphones designated for clinical teams to both communicate and acknowledge critical laboratory results, we demonstrate a significant, sustained increase in successful notification rates in H/O paediatric inpatients. Prior to our intervention, the overall success rate for the H/O unit was markedly lower than that of other units. This was credited to the fact that daily labs were typically drawn on the majority of H/O patients during the early morning hours resulting in a large volume of critical values (many of them for low haemoglobin, platelet and neutrophil counts) resulting shortly thereafter and causing challenges with timely closed loop communication with LIPs.
Our institution’s mechanism for tracking calls is aggregated by floor. While the H/O population is usually restricted to a single floor, we cannot control for the effect of a small percentage of non-H/O patients roomed on the H/O floor or H/O patients roomed on other floors. This effect is believed to have been at least partially responsible for the decrease in overall success seen in late 2019, as patient volumes increased throughout the hospital and the non-H/O patients on the H/O unit were not cared for by teams taking part in the phone notification system.
Prior to our intervention, the rate of timely outgoing notification for all inpatients was consistently high, suggesting the major issue was in reaching LIPs and receiving timely acknowledgement, a theory supported by the mapping of key drivers by our multidisciplinary group, as well as the fact that no difference was seen in the frequency of ICU assessments of H/O unit patients before and after our intervention. After implementation, there has been a slight but sustained decrease in timely outgoing notification, suggesting that the new process requires more time and/or effort for laboratory and call centre personnel. However, with an approximately 70% increase in overall success, the improvement in identification and timely acknowledgement by LIPs clearly outweighs that decrease.
Conclusion
In our free-standing paediatric hospital, use of a smartphone-based system to disseminate and acknowledge critical laboratory values resulted in a striking and sustained increase in the proportion that met institutional goals for successful notification.
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors contributed to the conception and design of this project and its intervention. LB, RF, LF, SG, CK, JM, SM, SH and DC tested and troubleshot the intervention, coordinated with laboratory and communication personnel and collected and provided data. KW, MH and KLM provided education and coordination with clinical providers. MH and KLM prepared and edited the main text and figures. KW edited the text and figures. All authors approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.