Article Text

Abstract
The theatre sterile surgical unit (TSSU) is an essential core to support the operating theatres in National University Hospital. Surgical instruments and supplies are processed, packaged and sterilised safe for surgical procedures. A rapid improvement event adopting lean methodology was conducted with the TSSU team to streamline the workflows in this area.
The project aimed to identify TSSU work processes that can be streamlined or automated, improving timeliness while identifying potential for role redesign and maximising human resource.
The team successfully implemented initiatives to eliminate unnecessary workflows and achieve workload levelling. This reduced instrument processing time by 5%, while replenishment times of surgical supplies to the operating theatres decreased by 29%. The team successfully redesigned the TSSU job roles, converting several nursing staff to non-nursing roles. Long-term initiatives such as the use of disposables and an improved theatre instrument management system were planned for as well.
Initiatives derived from this project can be spread to other sterile supply units within the hospital, further optimising the use of resources at a hospital level. The concept of role redesign was found to be applicable to healthcare, highlighting its potential in other areas of the hospital.
- Continuous quality improvement
- Healthcare quality improvement
- Lean management
- Quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The National University Hospital (NUH) is an academic acute hospital that is part of the western medical cluster, National University Health System in Singapore. The theatre sterile surgical unit (TSSU) plays an important role in the daily function of the hospital’s operating theatres (OTs). The TSSU ensures that surgical instruments used in the OTs are cleaned and sterilised, replaces instruments which are no longer serviceable and restocks the OTs with the appropriate instruments for the day’s surgeries. The TSSU’s function is crucial to the success of surgical departments, serving an important role in the hospital.
Cleaning surgical instruments after each surgery removes existing blood or tissue, while sterilisation prevents the spread of diseases by bacteria or other pathogens.1 Studies have shown that the average rates of error in packing surgical instruments are around 1%–3%.2 3 Although there is no conclusive evidence of these errors leading to detrimental patient outcomes, complications resulting from the delays may have a negative impact on surgeries. These errors may also result in the contamination of the surgical instruments which then require rework, causing delays to the workflow. Moreover, the TSSU’s operations were tedious and labour intensive, resulting in long turnover times and high manpower costs. The process requires a total of 28 nursing-trained staff working in the TSSU to support the operating theatres 7 days a week.
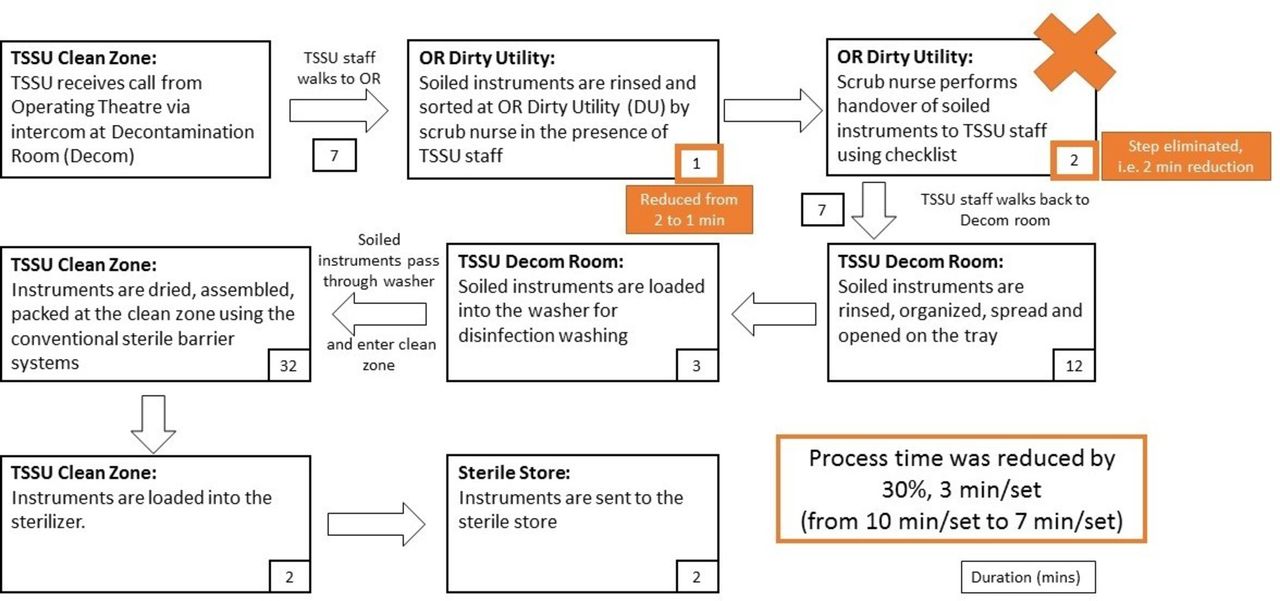
Through random observation, audit and interviews with staff, workflow inefficiencies were noted in the existing TSSU’s operations (figure 1). Currently, both the TSSU staff and the scrub nurse would check for completeness of the instruments together and carry out the handover process. The TSSU staff would be stretched during peak periods while idling at other times (depending on the OT timings), resulting in suboptimal use of resources. Similarly, both parties have to investigate when an instrument was found missing, resulting in the TSSU staff being unable to carry out other tasks despite having just taken over the instruments. On preparation of instruments, TSSU staff would prepare a generic set of instruments and consumables for orthopaedic elective surgeries. The generic cart prepared by the TSSU may have instrument sets that were not required for the specific procedure, resulting in time wasted packing them in.

High-level workflow for TSSU. A workflow of the current process was drawn to identify wastes and inefficiencies. OR, operating theatre; TSSU, theatre sterile surgical unit.
In terms of documentation, physical forms and documents were used to account for the instruments’ movements. Such manual methods have greater potential for errors and delays during the recall process. In terms of communication, while high priority sets have to be turned around quickly to serve more operations, this special arrangement relied solely on verbal feedback and communication among staff which again could be error-prone.
Background
Singapore has seen a 50% increase of citizens aged above 65 years in the last 10 years, resulting in exponential growth in demand for healthcare services.4–6 With a shrinking workforce to support the ageing population, pressures are placed onto the existing healthcare infrastructures. Singapore’s Ministry of Health (MOH) announced the Healthcare 2020 Master Plan in 2012, highlighting measures to enhance the accessibility, affordability and quality of healthcare.7 Healthcare institutions have started automating labour-intensive activities, streamlining workflows, upskilling the existing workforce, to empowering patients and families to self-care.8 9
In the area of sterile supply unit, the common challenge faced by most hospitals has been how to cope with the increasing demand while managing the multifaceted constraints. The Singapore General Hospital implemented the TSSU instrument management system (TIMS) which improved inventory, supply and quality management of the instruments.10 Besides exploring automation, other studies discussed the benefits of outsourcing the function to create greater value within the OT team.11 These practices were assessed by the team, considering factors such as higher costs, longer logistics loop to determine its suitability for application in NUH.
Baseline measurement
First, the team generated data from Systems Applications and Products (SAP) software and hospital records between May and July 2017 to have an understanding on the work volume demanded of the TSSU. An estimated total of 89 sets were processed each day with an average of 979 sets each month (assuming 22 workdays per month). The data included the number of sets used in elective and emergency surgeries carried out between 08:00 and 22:00 on weekdays.
To understand the efficiency of the existing workflows and the outcomes of the interventions eventually, the following indicators were selected and measured prior to the project.
Time spent on handover and processing
A random observation and audit was conducted to capture the amount of time spent. This process accounted for approximately 890 min (10 min/set, 89 sets) a day.
Time spent on case cart preparation and restocking
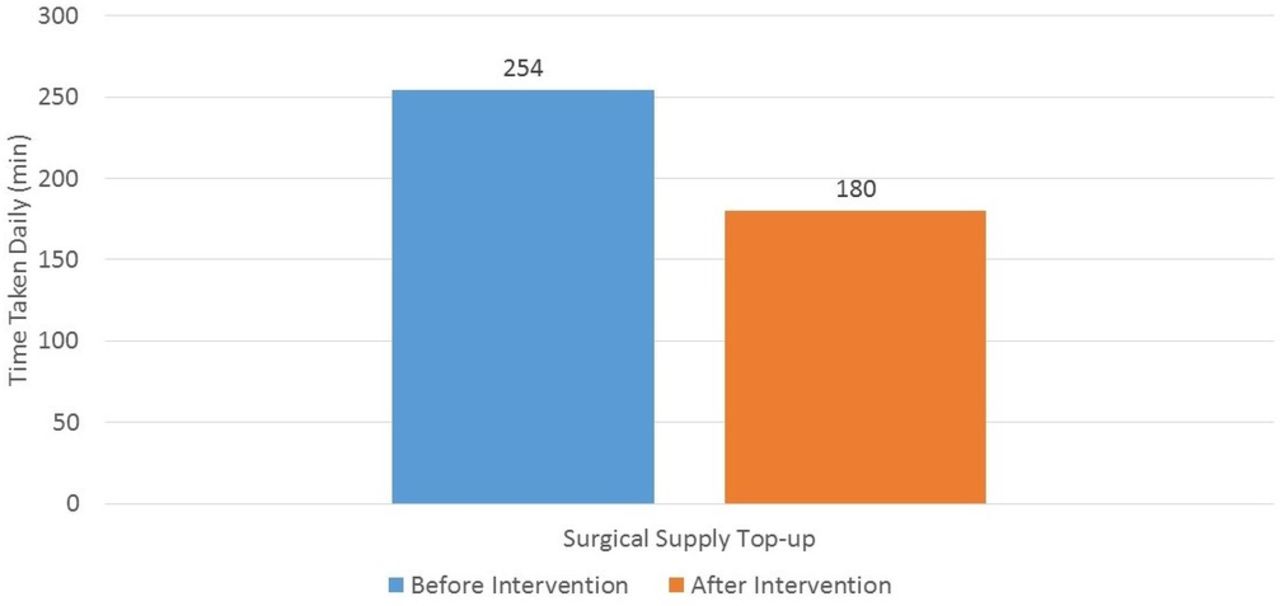
Similarly, a random observation and audit was conducted to measure the time spent on preparation and restocking. This process required about 4 hours (254 min) for the TSSU staff to prepare, distribute and restock (when necessary) the consumables and receptacles across all the OTs.
Workload distribution
The team also recognised the importance of analysing how manpower was deployed to manage the workload. With data obtained from hospital records, the number of instruments processed per hour was juxtaposed with the staffing per hour for analysis (figure 2). There was a lower workload from 07:00 to 09:00 as compared with 18:00 to 22:00, and the manpower deployed may not be proportionate to the demand at the hour.

14-hours period (07:00–22:00). Uneven workload levelling was observed, especially at 08:00–10:00, 13:00–17:00 and 17:00–22:00. A mismatch was noted between the number of staff deployed and the trend of instrument sets used throughout a day.
Design
This project was primarily a nursing initiative which was highly supported by senior management, with nursing directors assuming the role of project sponsors. The planning team included nurses of different seniority, with senior nurses being the team leaders. The team leaders led, managed and guided the team, bearing responsibility for the improvement process and outcome. Team members, contributed actively in the improvement process, working to deliver the desired results. On encountering roadblocks, the team would seek the support of the sponsors. ‘Fresh eyes’ (administrative staff from a different department) were embedded in the planning team to encouraging fresh perspectives and challenge existing ideas.
Through a series of brainstorming exercises during the rapid improvement event (RIE), such as paradigm shift, ideal state and cell concept (refer to online supplementary annex), the team developed strategies to address issues identified in the process mapping. A future process map and detailed implementation plan were subsequently developed to guide the execution.
Supplemental material
The team focused on five key areas to achieve its goals of improving the processing time and surgical supply distribution:
Streamline processes by eliminating wastes.
Optimise manpower allocation and utilisation.
Role redesign.
Explore alternative resources.
Future plans.
Strategy
An RIE using lean methodology tools and following the plan-do-study-act framework was convened to improve the processes in September 2017.
Streamline processes by eliminating wastes
Handover process
After reviewing the process, the team decided that the handover of soiled instruments between two staff can be eliminated. Moving forward, the scrub nurse places the used instruments in a tote box in the dirty utility (DU). The TSSU staff would then collect the box from the DU within 45 min of being informed. This reduces the waiting time for both parties as they will not need to wait for one another to conduct the handover. Moreover, the scrub nurse would have the responsibility of ensuring that all instruments used during the surgery have been accounted for, detecting missing items earlier in the process. The TSSU staff would check the completeness of the sets before loading them into the washer and highlight any discrepancies to the scrub nurse.
Case cart
The team proposed the use of customised case carts catering to the needs of each discipline. By referencing the listings of the following day, TSSU staff will pick out the relevant instrument sets and consumables according to disciplines. For ad hoc surgical listings on the same day, the scrub nurses will prepare their case carts for the procedure. Case cart preparation by TSSU staff relieves the scrub nurses from this responsibility, giving more time for patient interaction and care.
Optimise manpower allocation and utilisation
Staffing by demand
With the new roster scheduling, staff will be better distributed to match the workload throughout the day, with 5–16 staff members on duty at any one time. An analysis of the hourly workload showed an increase in activities during the peak hours of 11:00–18:00, requiring 7–9 staff to operate effectively. This reduces the idle time during non-peak hours and shifts the manpower needs to when it is required, optimising manpower resources.
Role redesign
Job role redesign
During the RIE, the team sought review the entire TSSU process, such as decontamination, packing, sterilisation and storage. The processes were assessed that it may not require a trained nurse and can be executed by trained technicians. If achievable, it would free up the existing nursing staff to fill nursing-related jobs in the hospital.
Explore alternative resources
Outsourcing–single use items
Reprocessing of reuseable items and instruments are time consuming and labour intensive. The autoclaves used for sterilisation are limited in quantity, causing a bottleneck to form during this process. Therefore, the team explored converting certain items to disposable variants,11 which will require less staff to complete the sterilisation during the later shifts.
Future plan
Improved instrument management systems (IMS)—projected 2019
To improve accuracy and efficiency, the TSSU is looking to engage external vendors to set up electronic documentation for the instrument management process. Leveraging on information technology eliminates the reliance on manual documentation, streamlines the process and enables the traceability of instruments in real time (up to the point of patient use). Serviceability of instruments will be greatly improved, with accurate data to track their usage and for scheduling of maintenance. This will also result in better management of priority sets as the TSSU will know which equipment to prioritise, leading to better management, efficient case scheduling and reduced scheduling conflicts. Additionally, monitoring of instrument usage patterns will result in more informed procurement decisions for the OTs.10
The use of technology also allows for the enhancement of the training materials used to teach new staff. Instead of relying solely on a senior staff’s knowledge, standard materials can be made available online to guide the new staff. In addition, video training detailing packing of complex or unfamiliar sets can be uploaded onto an e-learning resource for existing staff to refresh their knowledge.
Results
The results below were gathered through sampling in March 2018. The team had undergone three review meetings and continuous improvements prior to the results being gathered.
Handover process
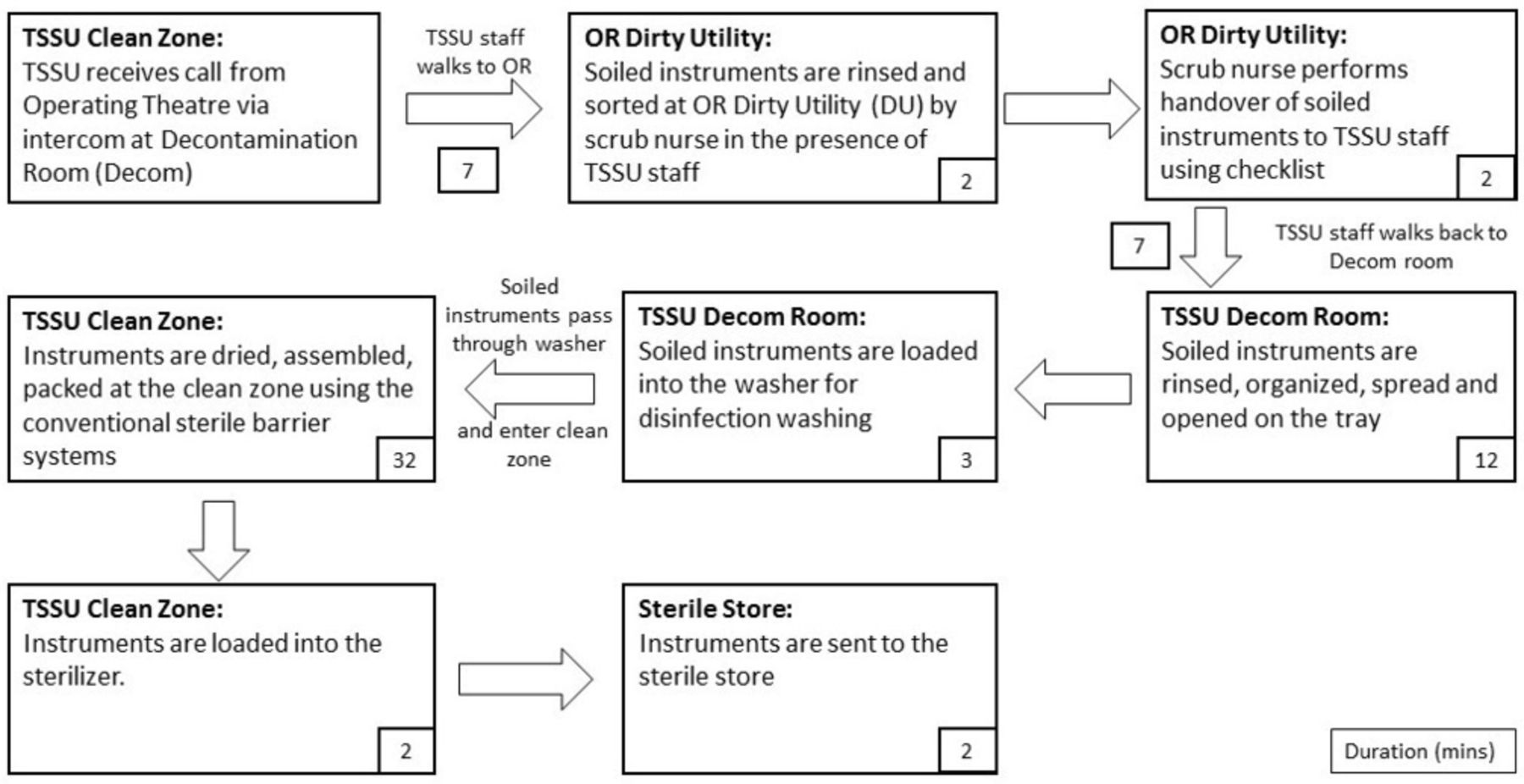
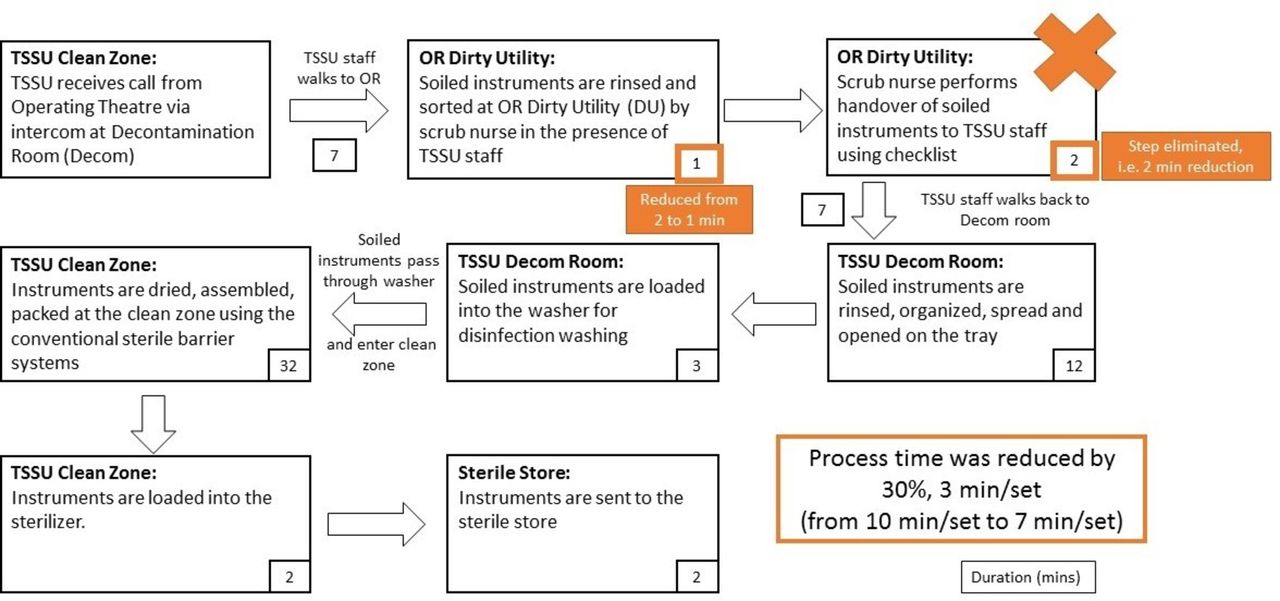
By streamlining the handover, process time was reduced by 30%, 3 min/set (from 10 min/set to 7 min/set), as the scrub nurse does not have to go through each instrument with the TSSU staff (figure 3). This results in substantial time savings of 267 min a day from an estimated 89 procedures daily (5% reduction of time spent). Accounting for the optimisation of manpower allocation and utilisation (figure 4), each decontamination staff eliminated 14.3 hours of waste from the handover process every month (assuming 22 working days per month) (figure 5).
Revised high-level workflow for TSSU. A revised workflow of the current process was drawn to illustrate the elimination of wastes and inefficiencies, resulting in time saving. OR, operating room; TSSU, theatre sterile surgical unit.
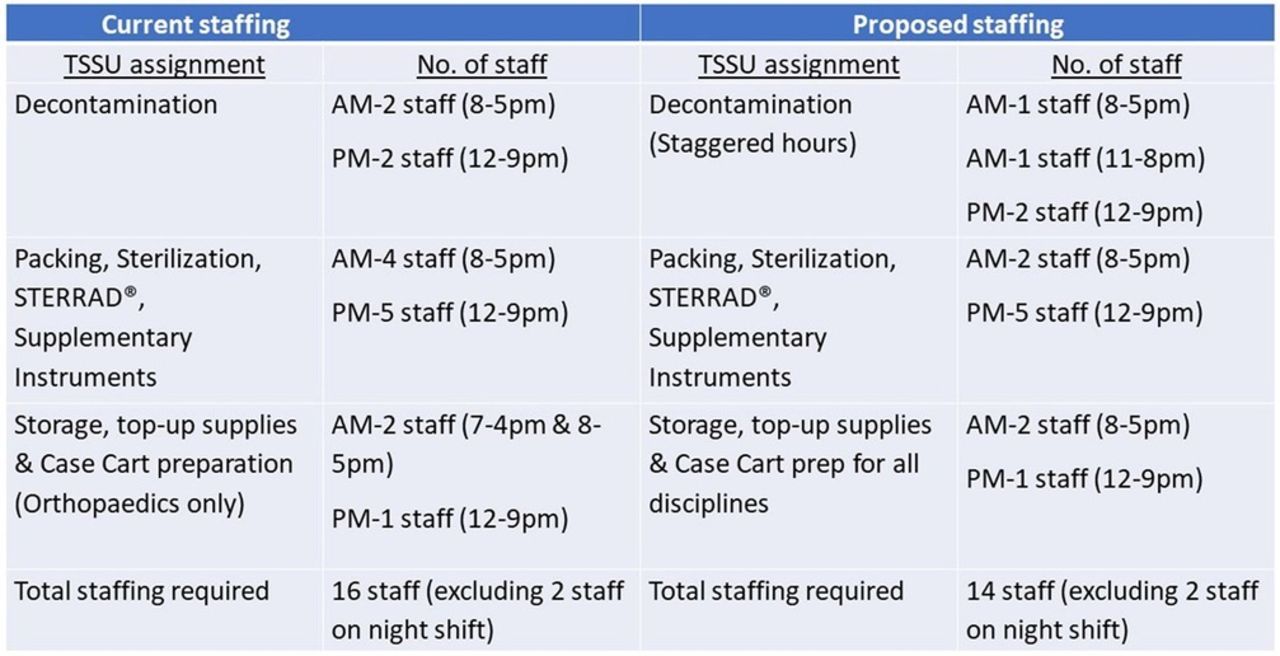
Current versus proposed staffing. The TSSU relooked and rearranged the staffing according to the demands in the theatre. This reduces the idle time during non-peak hours and shifts the manpower needs to when it is required, optimising manpower resources. TSSU, theatre sterile surgical unit.

Handover process time saving. The graph shows the contrast in time spent per month per staff in the handover process before and after improvement.
Case cart
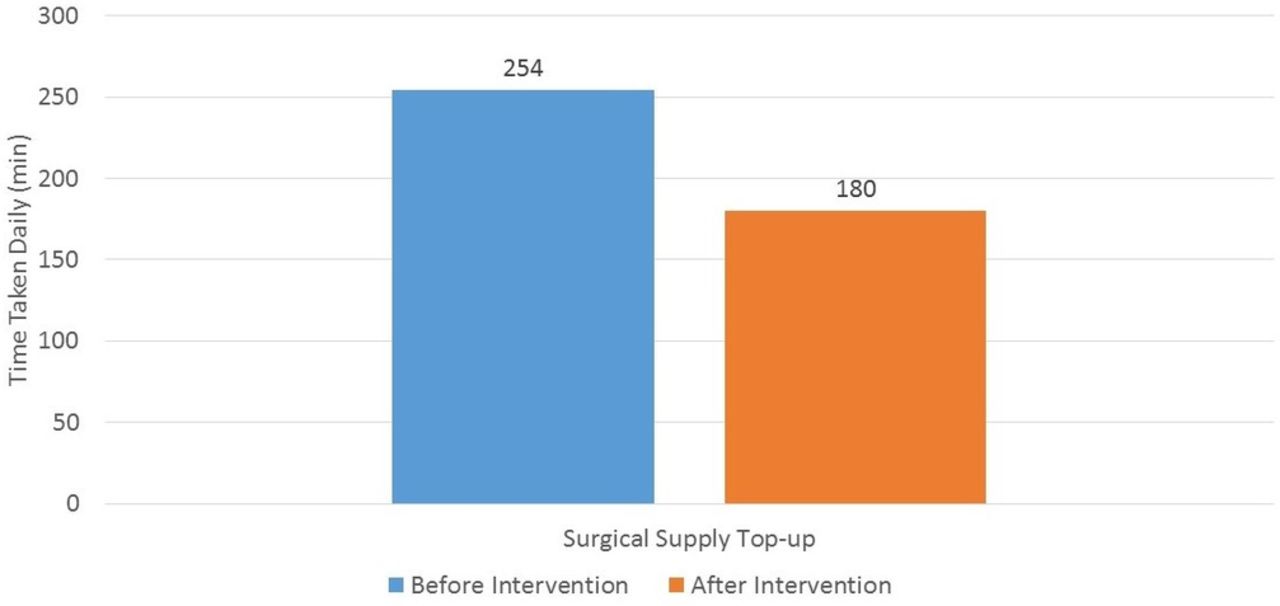
Time taken for the process of topping up surgical supplies has reduced by 29%, from 254 min to 180 min across two sessions each day for the 18 OTs (figure 6). The top-up is now done once at 10:00, coinciding with the manpower peaks in the TSSU. Through this workflow, a total of 27.1 hours a month (assuming 22 working days per month) have been saved.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case cart top-up time saving. The graph shows the contrast in time taken per day in the process of case cart top-up before and after improvement.
Workload levelling
An analysis of the hourly workload showed an increase in activities during the peak hours of 11:00–18:00, requiring 7–9 staff to operate effectively. This reduces the idle time during non-peak hours and shifts the manpower needs to when it is required, optimising manpower resources (figure 4).
Role redesign
The team analysed the tasks in the TSSU to identify those that do not require nursing trained staff. The following functions were subsequently identified: decontamination, packing, sterilisation and storage. The procedural and repetitive nature of these tasks allows for its execution by trained technicians instead of nurses. Hence, the team decided that seven nursing roles would be filled by non-nursing staff in the TSSU.
During the initial phase of implementation, each technician is paired with a nurse as part of their training process. The remaining nursing staff are assigned to more complex tasks, such as washing of complex instrument sets, steam sterilisation, verifying load and being preceptors to new trainees. This shift will allow some nurses to move to clinical areas to resolve any manpower needs and allow the nurses to hone their nursing skills.
Lessons and limitations
As the technicians become more proficient after a year of training, they will be able to execute their tasks independently and begin to train new technicians.
Obtaining sufficient data for the project has been challenging. The lack of an automated system results in the unavailability of big data, making comprehensive analysis of the baseline and assessing the impact of the changes difficult. Furthermore, the data collected for this experiment was based on manual documentations; the relatively small sample size could limit the reliability of the data collected due to sampling bias. Hence, the team could glean more insights and adopt more scientific approach towards process improvement with the support of IMS moving forward.
IMS and ‘single use items’ have not been implemented at the time this paper was written. The team is continuing to explore the usage of single use items to reduce processing time and are looking towards implementing the IMS system in 2019.
The team faced challenges implementing the procedure-specific case carts, due to the lack of agreement on the new approach and the delay in understanding what each discipline required. Obtaining the buy-in from all of the surgical disciplines took substantial effort and time before confirming the list of necessary instruments for their respective surgeries.
The approach of role redesign was sensitive as some staff misconstrued the exercise as a headcount cut. The team ensured that the transition to non-nursing staff would only occur on natural attrition. Moreover, the process of role redesign requires a period of time before its impact is felt. The technicians require on-the-job training period of approximately 1 year where they are paired with a nurse for various tasks. The exercise requires the support and understanding from the TSSU team during this period of time.
The sustainability of the project could have been further improved with better implementation of change management principles in the transition. Having a new process would invariably result in the team’s morale dipping during the teething period—especially among the staff who were not part of the planning process. Additionally, there was a lack of forcing function to complement the process. This could possibly affect the compliance to the new processes and its effectiveness in streamlining the processes in the TSSU.
Conclusion
The delivery of healthcare excellence is a concerted effort. TSSU is the core in providing behind the scene support to the OTs to provide optimal surgical care to the patients.
Approaching the problem using lean methodology tools, the team was able to review the entire process, breaking it down to identify the value-added steps and waste, eventually reducing the latter to streamline the process. The streamlining of the workflow has allowed the TSSU to maximise its manpower efficiency, reducing the processing time for both the TSSU staff and the scrub nurse in the OT. The changes not only improve the quality of life for the staff but also improves safety for patients as well: a more effective system to account for equipment, ensuring sterilised equipment are properly packed for surgeries and that staff can have more time to interact with patients.
Furthermore, the RIE process enabled the team to identify the potential for role redesign in the TSSU. Although the concept of role redesign is not often explored in the context of a hospital, it is a potential avenue to further optimise the hospital’s workforce. This would involve matching the right skills to the right job scope, providing sufficient challenge and reducing the monotony of their tasks. This translates to an increase in job satisfaction, with the staff understanding that technicians can be up skilled to undertake the non-nursing tasks, allowing nursing staff to focus on nursing tasks. This maximises the potential of both job groups and optimises the organisation’s resources. Although this could be a subject of much debate, this is imperative in face of slower workforce growth and higher demands presented in healthcare with a faster ageing population.
Acknowledgments
The authors wish to thank Joann Pang Wei Shen, Tan Cheng Hong, Tong Kim Loo, all those involved in the RIE in the TSSU, the senior leadership and the NUH staff for their contributions towards the programme.
Footnotes
Contributors All the authors listed have contributed in one way or another to the work described in the article. HMP, HLY and CT led a team to plan and conduct the project described in the article. BL, BS and YHL contributed to the reporting and writing of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.