Article Text

Abstract
In 2016, the Older People’s Mental Health Service (OPMHS) within Bedfordshire and Luton (provided by East London Foundation National Health Service Trust) faced considerable challenges in providing an accessible service for assessment of suspected dementia. Those referred to the Memory Assessment Service (MAS) encountered waiting times exceeding national recommendations. A quality improvement (QI) project was initiated by OPMHS Psychologists within all four multidisciplinary MAS clinics in Bedfordshire and Luton. The project aimed to reduce the time from the date of referral for within-team neuropsychological assessment to finalisation of the report to 6 weeks (42 days) by April 2017. In parallel to the initiative, the wider impact of the QI project was investigated. Through the combination of change ideas tested and implemented, all four MAS clinics were successful in meeting the primary project aim. The combined mean time between referral received by psychology and report finalised reduced by 28.76 days from 65.1 to 36.34 days, and with reduced variation across the clinics. These changes were sustained throughout the duration of the project and beyond, and successful change ideas were incorporated into routine practice with control methods developed. Exploring the wider impact, a focus group with six psychology staff members involved in the project was also completed. Thematic analysis identified three themes from the focus group: staff impact, service impact and service user impact. Further subthemes were identified regarding both desirable and undesirable impact across the system. The approaches used may be useful for other services embarking on reduced wait time initiatives for access to care. Additionally, understanding ongoing areas of impact on staff, the wider service and service users can help reduce or mitigate undesirable or unintended consequences and work towards sustainability of such changes.
- dementia
- waiting lists
- process mapping
- control charts/run charts
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
In 2016, the psychology staff within a National Health Service Older People’s Mental Health Service (OPMHS) in Bedfordshire and Luton faced challenges in providing timely neuropsychological assessment to people referred to the memory assessment service (MAS). While staff felt that some of the difficulties were at least in part due to resource capacity issues in the face of increasing demand, they also felt that alternative approaches might reduce the completion time for neuropsychological assessments and reports within the MAS pathway. As a result, the OPMHS psychologists embarked on a quality improvement (QI) project to reduce waiting times in July 2016.
Bedfordshire and Luton services cover a general population area of approximately 670 000 people. Four locality based MAS clinics were developed from 2004 onwards, primarily from within existing funding for community mental health services for older people. Psychologists work as part of multidisciplinary community teams which provide both MAS and Community Mental Health Teams (CMHT) services, and additionally provide in-reach to older adult inpatient services. They offer psychological and neuropsychological assessment and a range of psychological interventions, including individual and family interventions and working with carers in community residential settings. At the time of the project, staffing across the four localities consisted of a part-time consultant clinical psychologist lead, 2.7 clinical psychologists, 3 assistant psychologists and part-time trainee clinical psychologists on temporary placement. Managing the resource effectively across competing demands with an increasing ageing population and national drivers to improve early detection of dementia provided a significant challenge.
The MAS clinics offer a service for people referred for assessment of suspected dementia. In line with National Institute for Health and Care Excellence guidelines and Memory Services National Accreditation Programme (MSNAP) standards, specialist neuropsychological assessment is provided in a minority of cases where diagnosis cannot be satisfactorily established through an initial assessment, history taking and cognitive screen; and/or when the unusual or complex nature of presenting symptoms would benefit from greater assessment to assist individualised care planning.1 2 A recent 6-month audit of our four clinics found 9% of cases referred for neuropsychological assessment (ranging from 6% to 11% across the four clinics). The majority of neuropsychological assessments are undertaken by assistant psychologists, with supervision of interpretation and reporting required by the supervising clinical psychologist. In order to facilitate more timely access to accurate diagnosis, the QI project aimed to reduce the time from the date of referral for neuropsychological assessment to completion of the neuropsychology report to 6 weeks by April 2017.
Background
Improving timely access to early diagnosis has been a consistent national priority since the publication of the National Dementia Strategy in 2009.3 Diagnosing and treating dementia early has been shown to result in better adjustment, slowing of progression, planning ahead and savings to the health economy due to prolonged independence and delayed need for care home or hospital admission.4
At the time of the project commencing in 2016, the MSNAP5 stipulated that assessment begin within 6 weeks of referral, and diagnosis given within twelve weeks of referral unless further specialist assessments or investigations were required. Updated MSNAP standards and national policy since then has set the bar yet higher to increase the numbers of people diagnosed within 6 weeks of referral.2 6 7 While acknowledging that in cases with complexity requiring specialist investigation, the time to reach a diagnosis will often be longer.6
At the same time, with further national targets to increase the proportion of people formally diagnosed and an ageing population, memory clinics are in ever-increasing demand. The second audit of England showed an increase of 31% in people being seen in memory clinics between two annual national audits in 2013 and 2014.8 Audits have also revealed large variation across services in pathways and time to assessment and diagnosis. The second national audit revealed an average waiting time of 5.4 weeks from referral to initial assessment and a further 8.6 weeks between assessment and diagnosis.8 Variation across clinics was large, with time to assessment varying from 1 to 32 weeks, and referral to diagnosis ranging from 2 to 56 weeks. Both the averages times and ranges had increased compared with the previous audit, demonstrating the challenge that is faced nationally and indicating variation in practice. A Dementia Clinical Network established in London aims to reduce variation in local memory services through targeted service improvement projects.9 Their published audit again reported large variation in waiting times (average waiting times from referral to diagnosis ranging from 5 to 23 weeks), and additionally described variation in pathways including numbers referred for neuropsychology (ranging from 4% to 19%; average 11%). They highlight the clinical implication of the need to review and streamline pathways in an effort to reduce waiting times and variation. The present project was undertaken with a similar view of streamlining local pathways within existing resource to reduce variation and overall waiting time.
In addition to measuring whether or not QI efforts lead to the desired change, it is also important to examine the impact on different parts of the system.10 Ganz et al highlighted the potential concern of initiatives intended to improve healthcare quality, such as reducing wait times, generating unintended negative consequences.11 QI projects may encourage professionals to focus mostly on measured care at the expense of unmeasured care.11 12 For this reason, a focus group was also undertaken as part of the present project to collect staff narrative on the wider impact of the project.
Measurement
The project spanned neuropsychology provision across four MAS clinics, with some variations in multidisciplinary staffing profile, organisation and pathways. The following primary outcome measure was agreed and defined across the four clinics as follows:
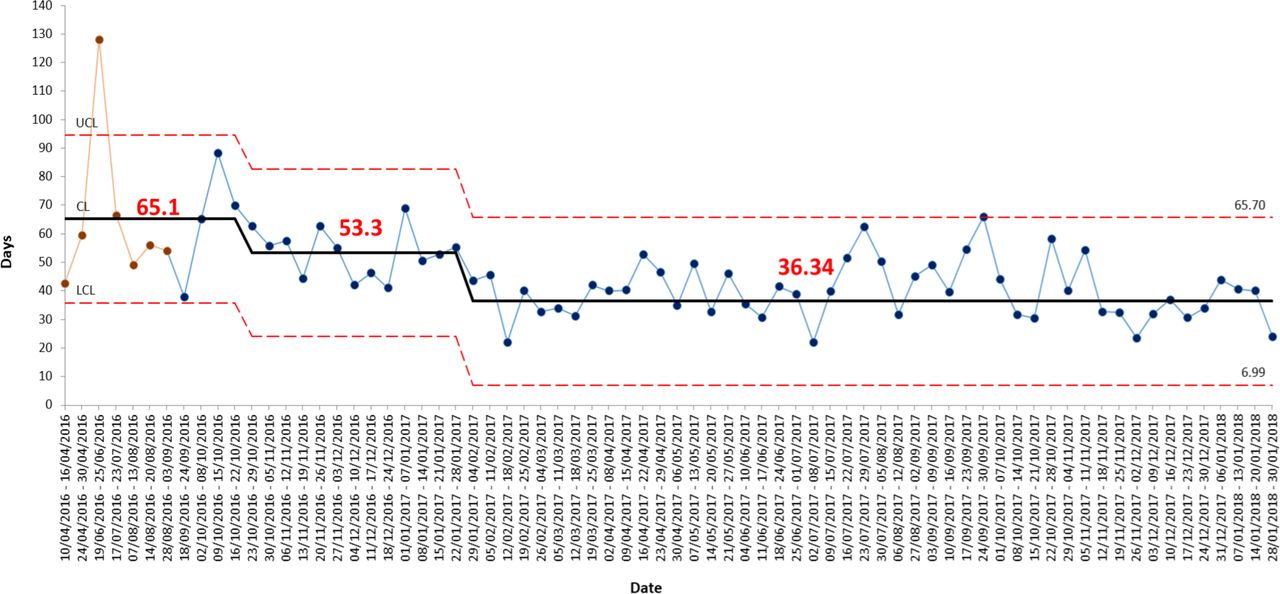
Number of days between referral received by psychology and report finalised. This was operationalised as the date psychology were first made aware of the referral, to the date the report was finalised by the qualified psychologist in the team. Baselines were established from available historical data for each clinic by plotting sequential referrals. The mean baseline for each clinic was 60.27 days in Luton, 65.29 days in Bedford, 84 days in South Bedfordshire and 43.36 days in Mid Bedfordshire. Combined weekly mean baseline data were calculated and plotted across the four clinics over a period of 5 months, with a mean of 65.11 days from 60 referrals.
Process measures of time between interim pathway points were used to identify variation and bottlenecks, and measure subsequent change in different parts of the neuropsychology pathway corresponding to specific change ideas.
Number of days between neuropsychological assessment completed to draft report completed. This was measured from the date the service user attended for assessment to the date that the draft report was completed by the assistant psychologist. At baseline, this was an average of 26 days in Luton, 16.57 days in Bedford, 28.14 days in South Bedfordshire and 14 days in Mid Bedfordshire.
Number of days between draft report completed to report finalised. This was measured from the date of completion of the draft report to the date the report was finalised by the supervisor. At baseline, this was an average of 16.43 days in Luton, 10.43 days in Bedford, 5.79 days in South Bedfordshire and 3.36 days in Mid Bedfordshire.
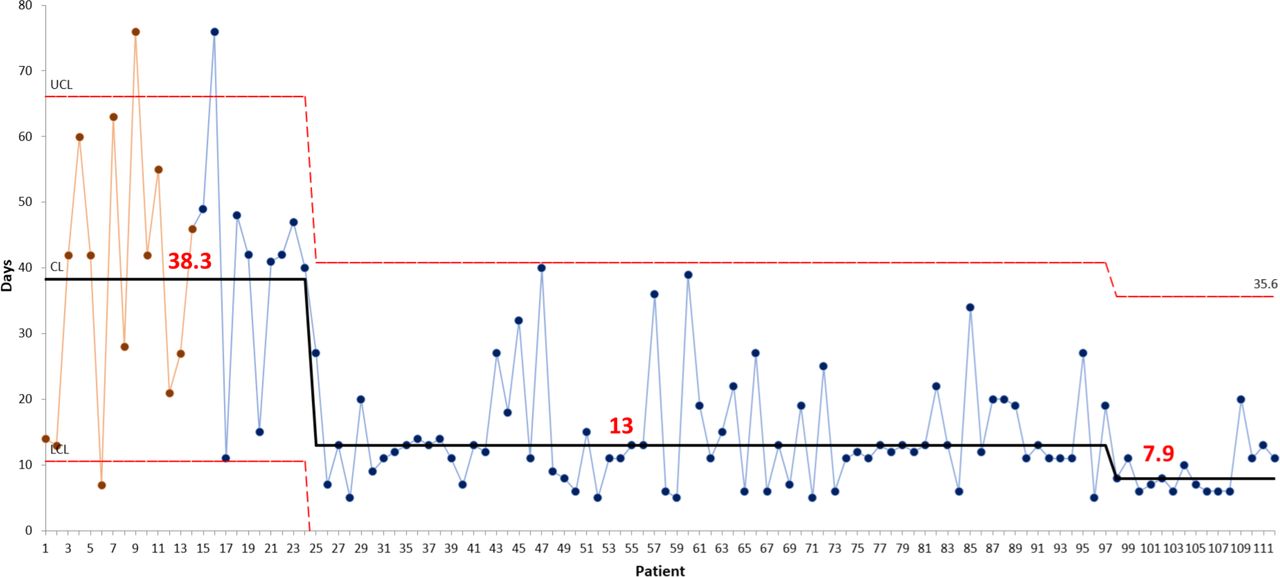
Number of days between referral received by psychology to neuropsychology assessment. This additional process measure was reported for the Bedford MAS clinic, as it was identified that there was a specific delay in this clinic in the initial assessment documentation and formal referral onward to psychology being completed. This was measured from the date psychology were first made aware of the request (usually verbal or email communication) to the date the service user attended for neuropsychological assessment. At baseline for the Bedford clinic, this was an average of 38.29 days.
The data were collated electronically for each clinic through creating and completion of spreadsheets which captured common pathway points. The dates were inputted by assistant psychologists, and number of days between key pathway points automatically calculated. The dates were either known to the assistant psychologists, who initiated most neuropsychological assessments and followed the process throughout, or accessed on the shared electronic care system ‘RiO’. These data provided both outcome and process measures.
Design
Completing the neuropsychological assessments and reports in a timely manner was an identified common work pressure for the psychologists across teams. In our regular 6–8 weekly psychology meetings, we identified that there was a degree of variation in both time and practice, and were all keen to find more effective and efficient ways of working. As a group, we regularly reviewed practice (not using QI methodology) to reduce variation and agree standards of practice (eg, referral criteria, standardised assessment protocols and report writing). We therefore had an established shared purpose and culture of improving and sharing common practice, and were enthusiastic about the opportunity to use QI methodology.
Three of our group (EE, AC and ET) were attending a 6-month QI training with the Trust which coincided with the early phases of the project, and two of these took on key roles of project leadership (EE) and coordinating the data (ET). The project sponsor was also trained in QI and involved in leading early stages of the project development (HD). A trained QI coach was available to support the project. We chose to meet fortnightly throughout the project. As the four team bases were up to an hour’s travel apart, we used teleconference and videoconference facilities with screen sharing for project meetings between the usual psychology meetings. This was effective in supporting regular high attendance to maintain group momentum while minimising impact on usual work.
The project used the Model for Improvement framework13 to agree and clearly define the aim, the measures to be collected, and change ideas to be tested and refined using Plan-Do-Study-Act (PDSA) cycles. In the early stages of the project, a process mapping exercise was completed to understand commonalities and variation in the pathway for neuropsychological assessments across the four teams, and to identify the key common pathway points that would be used for data collection of both outcome and process measures. The collected knowledge about variation across teams informed our theories about barriers and opportunities for change. Divergent and convergent thinking techniques were used to identify and group the range of issues impacting waiting times into drivers. From this, the team was able to generate and agree the selection of change ideas, completing the driver diagram. As a group we selected initial change ideas to test that we believed were likely to have highest impact and were easiest to implement (i.e. those over which we felt we had most control).
As the project progressed along some months, we also undertook a force field analysis to consider the driving and restraining factors. This was a helpful tool following the initial burst of change and enthusiasm to maintain momentum and creatively broaden focus.
Patient and public involvement
We did not directly involve patient and public involvement in the project. A questionnaire of service user and carer experience was devised and used during the project to generate change ideas to improve experience. Some respondents then took part in semistructured interviews with a trainee clinical psychologist to provide in-depth feedback on their experience of neuropsychological assessment, reported in a separate evaluation project.
Strategy
PDSA cycles
We used a series of PDSA cycles to test change ideas expected to standardise or streamline practice. We then met to feedback learning from these cycles, and look at data to understand whether the changes resulted in improvement.
Standardising referral criteria for neuropsychological assessment
Clarifying and disseminating information regarding appropriate referrals: initially an assistant psychologist drafted a list which was then brought to the team meeting to discuss points of difference and achieve consensus (eg, level of alcohol intake we would accept). This was tested initially in one MAS team to gain multidisciplinary feedback, and then rolled out to the remaining MAS teams. This resulted in a more consistent stance of referral acceptance.
Reducing administration time in booking appointments
Editable letters on the electronic records system: these inputted patient details automatically from their electronic record, saving valuable time in appointment letter and report writing. The completed letters could also then be automatically uploaded onto the system. The editable letters were first drafted by an assistant psychologist and brought back to the team meeting for feedback. These were then adapted for each service by the remaining assistant psychologists, and sent to the relevant area to be made available on the electronic records system (RiO) for all teams.
Reduce time between the neuropsychological assessment and draft report completed. A change idea was developed and tested through cycles as follows
Scheduling slots for scoring and writing of reports at the time of booking the assessment: this was initially trialled by one assistant psychologist for 1 week. The next cycle involved all assistant psychologists testing and feeding back to agree the most effective approach. Once agreed, the approach was scaled up to be used on an ongoing basis by all assistant psychologists.
Reduce time between draft report completed and report finalised. Two change ideas were developed
Flexibility across teams to supervise reports; this was in order to provide cover for annual leave across teams.
Supervisors to define slots in their calendar to check reports; initially, one supervisor defined a block of 2 hours in their calendar for checking of reports, and the assistant psychologist would input names into the slots that required checking. This was scheduled to run for 1 week and then feed back. It was found that other more urgent matters took priority and therefore this was not successful. The next phase involved colour coding the shared spread sheet so the supervisor was able to prioritise reports for checking, the name of the person and report was also embedded into the table. This proved to save time and was easier to stick to. However there were still often times when a non-MAS report that needed to be prioritised took precedent.
In Bedford MAS, reducing time between referral discussion and the date of neuropsychological assessment.
Gathering information from the initial MAS assessment without waiting for the written report: this involved a PDSA cycle of (1) the assistant psychologist using a proforma, (2) gathering relevant information from verbal feedback during the multidisciplinary team meeting and (3) photocopying the clinician’s handwritten notes from the initial assessment. This was so an assessment plan could be decided promptly either during or promptly following the multidisciplinary meeting and assessment appointment booked in.
Qualitative information
To understand the team’s experience of the wider impact of QI initiative, a focus group was undertaken by a trainee clinical psychologist on placement with the service during part of the project duration (LC). Eight members of the team were invited to participate, and six agreed to take part (three clinical psychologists and three assistant psychologists) in a 1-hour group interview. A semistructured interview schedule was developed; the following questions were open ended in order to elicit detailed feedback.
What were your thoughts when the QI of reducing wait times was introduced?
How have you found the process up to now?
What do you think the impacts have been on other areas of your work?
What do you think the impact has been on non-MAS services?
What do you think the impact of the changes has been on service users?
Thinking about the QI overall, what do you think about the impact that this has had for you, the service and the team?
The group session was recorded and subsequently transcribed. Thematic analysis was undertaken following Braun and Clarke’s guidelines.14
Results
Primary outcome measure
Through the combination of change ideas tested and implemented, a reduction was achieved in the mean time taken in the neuropsychological pathway across the four clinics, and this fell below the target time of 42 days in all services. Luton reduced by 27.38 days to a mean of 32.89; Bedford reduced by 25.15 days to a mean of 40.14; South Bedfordshire reduced by 55.5 days to a mean of 28.5 and Mid Bedfordshire reduced by 7 days to a mean of 36.3. Combined this resulted in a reduction of 28.76 days to a mean of 36.34 days. Control charts of the primary outcome measure were developed for each of the four teams; the control chart of combined data demonstrates the desired reduction in time across the four clinics, and this being sustained over a period of 12 months (figure 1).

Primary outcome measure: time taken from referral received to neuropsychological assessment report finalised across four clinics (I chart).
Process measure: completing the draft report
The PDSA testing cycles relating to completion of the draft report was found to have the largest impact on reducing the overall time, and additionally reduced variation across teams (figure 2). The reductions achieved were 21.6 days in Luton to a mean of 4.4 days, 9.3 days in Bedford to a mean of 7.3 days, 20.8 days in South Bedfordshire to a mean of 7.3 days, and 5.7 days in Mid Bedfordshire to a mean of 8.3 days. Aside from the benefits to service users, the assistant psychologists reported that this change led to greater efficiency in writing reports, as the information was fresher at the time of writing, and involved holding fewer people in mind at a time. Assistant psychologists also reported that the new structure helped to manage the workload and clear any backlog.

Time in days from neuropsychological assessment undertaken to draft report completed (I charts).
Interrogation of outlier data points in this process measure revealed a range of reasons for longer completion times including; (1) assessments completed by staff new to the service in a learning phase, (2) competing work demands, (3) staff leave and (4) a clinically complex case presentation requiring assessment by the clinical psychologist rather than assistant.
Process measure: time between referral and assessment date in Bedford MAS
Bedford MAS identified a particular bottleneck between the date the referral was discussed with psychology and the date the assessment was completed. Through PDSA cycles of obtaining relevant information about the referral in the multidisciplinary meeting, and photocopying the initial assessment handwritten notes, this allowed for the assessment plan to be promptly agreed. A reduction of 30.4 days to a mean of 7.9 days was achieved (figure 3).

{kind=link}
{kind=link}
{kind=link}
Time in days from referral discussed to neuropsychological assessment completed in the Bedford MAS (I chart).
Qualitative results: staff focus group
Staff identified both positive outcomes and challenges as a result of the project being undertaken. Three main themes (staff impact, service impact and service user impact) with eight subthemes were identified. The themes interrelate in many ways, for example, an impact on service provision can inevitably impact directly or indirectly on the service user. However, it was felt organising themes in this way provided useful different perspectives.
Staff Impact
Sense of agency
All six members (100%) of the focus group agreed that the QI project fostered a sense of agency in what could be achieved. On reflection of the changes occurring in the wider service, perhaps having an aspect which was measurable and positive changes visible was something the team valued.
‘We have made targets ourselves, nobody imposed this on us and it has felt rewarding in that sense.’ (P3)
Connectedness of team
Three members (50%) of the focus group felt the QI project brought an increased sense of connectedness in the team through working collectively towards service improvement.
‘All come together and meet regularly and just keep much more connected as a group, which I think I really like’ (P4)
Under the ‘spotlight’
All group members (100%) described a sense of anxiety and pressure around the QI project being measured and monitored by the wider Trust.
‘The spotlight is going to be on what we are doing and oh no, can we? Is this realistic to get it down’ (P2)
This was also linked to the comparing of self to others and experiencing a sense of fear of one’s own performance being the worst within the team.
‘We all have the fear factor, that common factor of one single person delaying everything for everyone.’ (P3)
Three members (50%) of the focus group spoke about the impact of the QI project around increasing a sense of pressure to achieve and as a result working additional unpaid hours.
‘One of the things I have felt a bit concerned about is the sense of pressure and how that might invite me to break my own boundaries and do more work from home’ (P4)
Service impact
Transferable skills in approaching other areas of service improvement
Three group members (50%) described a change in their approach to other aspects of service delivery, with the availability of a methodology which was transferable to other service issues arising. This seemed to indicate an impact across the service, staff and service users, with QI methodology directly impacting the way the service approached new challenges faced.
‘You were using your knowledge to advise a team to reflect on something before they started to change.’ (P3)
A changing perception of the team around the role of psychology
Three members (50%) of the focus group described the possibility of a shift in referral type, thresholds and numbers made to the Psychology Service as a result of the QI project. It was suggested that the non-MAS (inpatient and CMHT) referral pattern may have changed.
‘A lot of the perception is that we are there to do neuropsych assessments and assess for dementia rather than thinking more broadly around psychological difficulties, so I kind of wonder how our focus on the memory clinic can feed into a change in how we are perceived’ (P3)
Service user impact
The positive impact of reduced wait times for MAS service users
It was felt by two members (33.33%) that the QI project to reduce MAS wait times would be well received by MAS service users.
‘I imagine it is positive in terms of waiting because waiting is a concern for clients who come through MAS’ (P3)
Less certainty around diagnosis
In terms of an undesired impact of the QI project, three members (50%) described an impact of having less certainty around diagnosis in some cases.
‘We are definitely more uncertain sometimes in our conclusion’ (P3)
‘Quicker to do quicker to score and quicker to report’ (P4)
Taking your ‘eye off the ball’ for non-measured aspects of service
Three members (50%) of the focus group questioned whether an impact of the QI project led to paying less attention to other non-measured areas of work.
‘I am spending so much time thinking about getting this bit right. Am I actually taking my eye off the ball which is the other part of my work’ (P2)
Two members (33.33%) of the focus group described prioritising measured aspects of work over non-measured areas.
‘It has taken such a strong priority though in the last few months or the last year. I found it inevitable that if I have a report that has got to be done from the memory clinic or it is a report that needs to be done for the ward then it’s the one for the memory clinic that I get done’ (P4)
Lessons and limitations
The present QI project achieved its primary aim to reduce the time taken to complete the neuropsychological assessment pathway within four memory services in Bedfordshire and Luton. We have reflected that a number of factors appeared to contribute to the project’s success, and there may be lessons applicable to other similar projects:
We were an existing professional team that met regularly with an established culture of working towards common practice.
We used technology solutions for regular meetings to overcome the geographical challenge and ensure cohesion and momentum during the project.
The flow chart exercise early in the project identified common points for consistent data collection, led to clear operational definitions and also identified variation in practice for generating a specific change idea in the Bedford team.
Key roles of project lead (organising and chairing meetings) and data coordination (to develop the common spreadsheets and lead on uploading data to the Life QI system) were integral to the project’s momentum and effectiveness.
The team was well supported by a strong organisational QI structure in the Trust with training of team members during the project, and coaching and sponsor support regularly available.
Following sustained improvements, an implementation plan was devised to standardise and continue the new ways of working developed through our project. These included standard referral criteria, gathering referral information at multidisciplinary meetings, use of standard letters and booking slots for scoring, writing and reviewing the reports. Methods for reviewing adherence were also introduced, including a visual control method on the referral spreadsheet that highlights impending expected date of completion to prevent breaches.
Qualitative feedback in the focus group provided us with valuable reflections on both positive and negative aspects of undertaking the project. Aside from meeting the project aims, other positive consequences were noted by project team members in the focus group, which included a sense of increased agency, team cohesion and generalised skills in improvement being applied to other areas of work. During a time of broader service change and instability (i.e. consultation processes, service closures and staff movement), having a measurable target to work towards collectively and seeing positive change over time was valued by the team. The ability to use the QI framework in other aspects of their role seemed to also provide a coherent methodical approach towards addressing further challenges faced, which in turn enhanced a sense of hope for positive change during uncertain times in the service.
A number of limitations and areas for potential lessons were also identified in relation to unintended negative consequences of the project. The QI project appeared to foster a sense of pressure to perform, which led to some clinicians contemplating working additional unpaid hours to complete project-related tasks, a finding noted in another recent article on waiting time projects.15 Staff also felt that the focus on and measurement of time taken may have resulted in an impact on the quality of the assessment reports being completed which were unmeasured aspects of the service delivered.
In broader impact, the clinical psychology staff (who have a broader role across services) reported they were prioritising MAS work over their non-MAS work, and had reduced their focus on other aspects of their role. This finding fits with concerns highlighted by other authors about the potential for unintended consequences arising in improvement projects on unmeasured aspects of care provision.10 11 To mitigate this, QI projects ideally include balancing measures to monitor areas of possible unintended negative consequence, and a limitation of the present study is that balancing measures were not decided and collected during the process of the project. It is notable that a recent paper of qualitative interviews with improvement experts in Scotland similarly found that in spite of guidance regarding the inclusion of balancing measures, these were not routinely collected and reported in the improvement literature.16 This, therefore, appears to be a challenge our project faced which is common within the wider QI community, and warrants ongoing consideration at senior levels within organisations as well as project teams themselves. While we did not collect balancing measures, the inclusion of a focus group to reflect on the present project has provided valuable information to inform the project and provide insight for future projects.
A further limitation reflected on was the project team membership being limited to psychology staff, without including multidisciplinary colleagues or service users as full members of the team. The importance of gathering service users/carers’ experience was recognised as an area to generate information which may inform further change, and a participants’ experience questionnaire was devised and used during the project. Service users and carers who completed the questionnaire were also asked if they would like to take part in more in-depth interviews, and follow-up interviews were facilitated by a trainee clinical psychologist in order to obtain feedback on their experience of engaging in the neuropsychological assessment process (to be reported separately). Nevertheless, the project team feel it was a gap to not have had wider representation of perspectives in team membership.
Conclusion
The project led to the desired reduction in waiting times and variation across the four clinics. The changes were sustained and translated into routine protocol with visual control methods developed to promote ongoing adherence. Further positive consequences were identified by staff as individuals and as a group. For all staff involved, this was their first training and/or experience in a formal QI project, and on the whole was a valuable positive experience.
Learning from the project includes the importance of routine standard data collection and reporting across the system in order to monitor routine performance and impact of any changes. Since completion of the project, changes have been made in the use of the electronic records system to collect additional data relating to psychology waiting times, reducing the need for manual data collection.
The project also highlighted the importance of both project teams and managers at an organisational level being mindful of potential unintended areas of impact that wait time initiatives can bring. Monitoring areas of potential impact can help to reduce or mitigate undesirable unintended consequences and work towards sustainability of desired changes. In the current project, balancing measures were not agreed and collected as part of the project, which was a limitation. However, impact on other areas of work were identified through the focus group, which encouraged project team staff to reflect on and generate valuable feedback.
A final learning point is the potential for creatively generating a wider range of meaningful change ideas by including other disciplines and service users and carers in the project teams. Service user feedback was collected which influenced the project team, but we did not have a service user as a full member of the project team. While limiting the scope of the project and the membership of the project team to those staff directly involved in the delivery of the service enabled greater control over the project, we recognise this occurred at the cost of the value that diversity of views would bring.
Acknowledgments
With thanks to the following clinicians involved in the QI project at different stages: Rachel Wenman, Jeannette Fuller, Sarah Moulton, Sophie Venters, Wendy O’Neill, Becky Grace, Rachael Mellor, Lauren Taylor, Sarah Knapp, Kim Caldwell, Elizabeth Booth. Thank you to Amar Shah for guidance regarding publication.
Footnotes
Twitter @HelenDonovan_70
Contributors HD initiated the project and acted as project sponsor, contributed to project design, data collection and analysis and drafted and revised the paper. She is guarantor. EE acted as project lead, contributed to project design, data collection and analysis, and drafted and revised the paper. LC designed the qualitative project, collected and analysed qualitative data, and drafted and revised the paper. ET contributed to project design, data collection and analysis, and drafted and revised the paper. AC contributed to project design, data collection and analysis, and drafted and revised the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.