Article Text

Abstract
Background Frail elders in residential skilled nursing facilities (SNFs) have high rates of emergency department (ED) utilisation and hospitalizations. We sought to implement and iteratively specify an intervention to improve utilisation and cost outcomes for frail elders in rural SNFs.
Objectives (1) To reduce unwanted and avoidable ED utilisation and hospitalizations; (2) to reduce related costs.
Methods Adopting evidence based practices, we iteratively developed an implementation approach including the following key elements: (1) advanced directives; (2) a dedicated closed-call team of providers following SNF residents; (3) a biweekly case review of all ED referrals and hospitalizations; and (4) a standardised triage communication process. We conducted three PDSA cycles over a 6 month period and assessed clinical and cost outcomes using inferential statistics and statistical process control (SPC) methods.
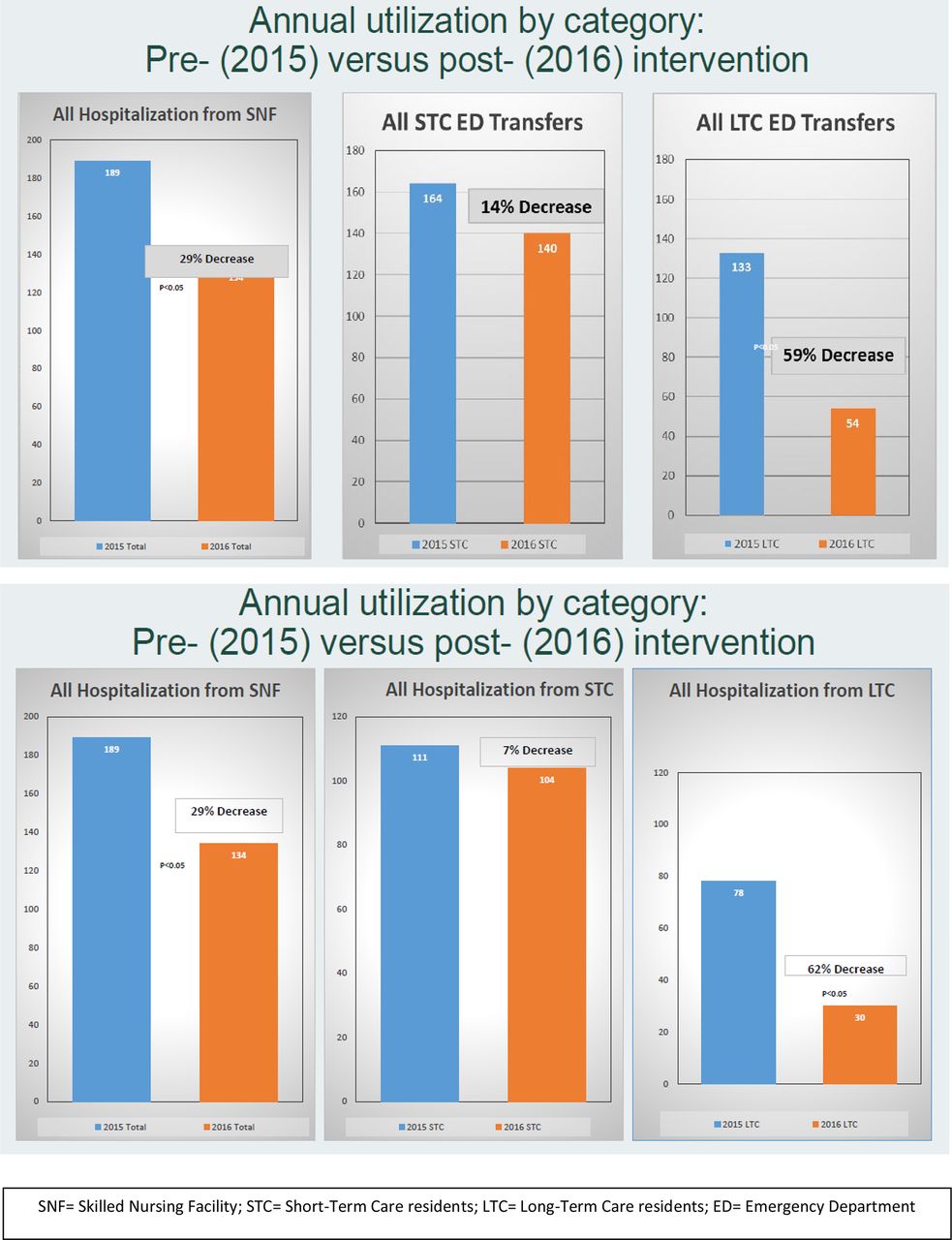
Results Three rural SNFs participated in the intervention from January-June 2016. Three PDSA cycles were conducted. Monthly hospital-based care utilisation for long term care (LTC) residents reduced from 10 to 3.3 episodes (p<0.05). ED transfers reduced by 59% (p<0.05), and hospitalizations reduced by 62% (p<0.05), without associated changes in overall mortality or quality performance indicators. SPC analysis suggests that PDSA Cycle 2 was temporally related to the onset of improvement. Estimated cost savings calculated based on utilisation reductions is approximately $7 million annually.
Conclusions This initial pilot was feasible, achieved significant outcomes, and is an example of the use of improvement methods to iteratively develop and optimise an implementation approach. This approach has potential to significantly impact outcomes, utilisation and cost and is worthy of continued study.



{kind=link}
{kind=link}
{kind=link}