Article Text

Abstract
Obstructive sleep apnoea (OSA) is more prevalent in patients with hypertension (HTN), and associated morbidities include stroke, heart failure and premature death. In the Internal Medicine Clinic (IMC), over 70% of the patients had a diagnosis of HTN and obesity. We identified a lack of OSA screening in patients with HTN. The aim of this quality improvement (QI) was to increase OSA diagnosis to 5% from the baseline rate of less than 1% in patients with HTN between the ages of 18 and 75 years over 6 months at IMC. We used the Plan-Do-Study-Act (PDSA) method. The QI team performed root cause analysis to identify materials/methods, provider and patient-related barriers. PDSA cycle included: (1) integration of customised workflow of loud Snoring, Tiredness, Observed apnea, high blood Pressure (STOP)-Body mass index (BMI), Age, Neck circumference, and Gender (BANG) OSA screening tool in the electronic health record (EHR); (2) physician education of OSA and EHR workflow; and (3) completion of STOP survey by patients, which was facilitated by nursing staff. The outcome measure was the percentage of OSA diagnosis in patients with HTN. The process measures included the percentage of patients with HTN screened for OSA and the increase in sleep study referrals in hypertensive patients with STOP-BANG score of ≥3. Increase in patient wait time and cost of sleep study were the balance measures. Data analysis was performed using weekly statistical process control chart. The average increase in OSA screening rate using the STOP-BANG tool was 3.88%. The significant variation seen in relation to PDSA cycles was not sustainable. 32% of patients scored ≥3 on the STOP-BANG tool, and 10.4% had a confirmed diagnosis of OSA. STOP-BANG tool integration in the EHR and a team approach did not result in a sustainable increase in OSA screening. OSA diagnosis was increased to 3.3% in IMC patient population within the 6-month period. The team identified multiple barriers to screening and diagnosis of OSA in the IMC.
- primary care
- quality improvement
- healthcare quality improvement
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Problem description
Currently, there are no guideline recommendations for obstructive sleep apnoea (OSA) screening in patients with hypertension (HTN).1–4 However, many patients with HTN have undiagnosed OSA. OSA increases the risk of HTN-related morbidities such as stroke, heart failure and premature death.5 6 Diagnosing OSA in patients with HTN and overcoming barriers to acceptance of a sleep study and treatment may result in improved blood pressure control and avoidance of complications associated with untreated and undiagnosed OSA.2 3 7 In Internal Medicine Clinic (IMC) population, over 70% of the patients have a diagnosis of HTN with a mean high body mass index (BMI) of 32 (obesity=BMI of 30 or greater8). Our baseline data showed that less than 1% of patients with HTN were screened and diagnosed with OSA. These data indicated that OSA screening and diagnosis in patients with HTN and obesity was underutilised in IMC. The aim of this quality improvement (QI) project was to increase OSA diagnosis to 5% from the baseline rate of less than 1% in patients with HTN between the ages of 18 and 75 years over a 6-month time period using the STOP-BANG sleep apnoea screening tool in IMC.
Background
HTN affects two-thirds of Americans over the age of 60 years and over 1 billion people worldwide.9 OSA affects 2%–4% of the adult population.6 10–13 Typical signs of OSA include snoring, nocturnal apnoea, daytime hypersomnia and poor concentration. OSA is classified as mild, moderate or severe based on an apnoea–hypopnoea index (AHI) of 5–15, 15–30 and greater than 30, respectively. Treatment for OSA is recommended for patients with an AHI greater than 15, or an AHI 5–15 associated with symptoms or cardiovascular comorbidities.14–16 Diagnosis is confirmed by polysomnography (sleep study), and continuous positive airway pressure (CPAP) therapy is the first-line treatment as per recommendations by the American Academy of Sleep Medicine.6 17
OSA is more prevalent in patients with HTN and obesity than in the general population.2 6 18 OSA has primarily been linked to HTN in sleep clinic populations, but little is known about the symptom profile of undiagnosed OSA in patients with HTN in a primary care setting. Only limited studies have examined the associations of undiagnosed OSA in patients with HTN in a primary care setting.19 Broström et al found that undiagnosed mild and moderate/severe OSA was seen among 29% and 30% of patients with HTN, respectively.20–22 The current guidelines by US Preventive Services Task Force (USPSTF) do not recommend any screening for OSA in asymptomatic patients due to insufficient research and data.1–4
The STOP-BANG screening tool has the highest sensitivity for OSA screening; therefore, we used this tool.23–28 The loud Snoring, Tiredness, Observed apnea, high blood Pressure (STOP)-Body mass index, Age, Neck circumference, and Gender (BANG) questionnaire is a validated screening tool for identifying OSA. STOP questionnaire refers to patient’s history questions and BANG questionnaire refers to demographics and physical examination. It is scored based on Yes/No answers (score: 1/0). Thus, the scores range from a value of 0–8. Score of 0–2 is low risk, 3–4 is intermediate risk and 5–8 is high risk for OSA.23–28 This OSA screening QI was designed to screen patients with HTN.
Methods
Setting
We conducted a QI project in an academic IMC, located within a tertiary care safety net hospital, Erie County Medical Center (ECMC). A safety net hospital provides a significant level of care to low-income, uninsured and vulnerable populations regardless of their ability to pay.29 The IMC is comprised of a multidisciplinary care team including attending physicians, residents, nurses, a social worker and administrative staff. IMC had about 25 clinic staff including nurses (Registered Nurses (RNs) and licensed practical nurse (LPNs)), medical office assistants, clinic manager and a social worker. The IMC patient population consisted of mostly urban and underserved. Patients used IMC as a longitudinal primary care clinic with average monthly visits about 700 and had consistent 80% show rate. Forty residents from the Internal Medicine Residency programme of the University at Buffalo, State University of New Yorkand five attending physicians served this ambulatory academic clinic.
Measurement
We used electronic health records (EHR) to create an electronic patient registry in collaboration with the information technology (IT) department. Retrospective review of the EHR database of patients seen within 6 months showed that less than 1% of patients with HTN were screened and diagnosed with OSA. We included male and female patients, between the ages of 18 and 75 years. The outcome measure was to increase the percentage of OSA diagnosis in patients with HTN to 5% from the baseline of less than 1% in IMC. Process measures included: (1) increase percentage of OSA screening in patients with HTN to 10 % from the baseline rate of less than 1%, using STOP- BANG screening tool; and (2) increase the number of sleep study/pulmonary referrals in patients with HTN with STOP-BANG score of ≥3. In the STOP-BANG tool, a score of ≥3 has shown a high sensitivity for detecting OSA: 93% and 100% for moderate and severe OSA, respectively.24–28 Those who qualify, a score of ≥3 on the STOP-BANG tool, were offered the sleep study/pulmonary clinic referral to confirm diagnosis of OSA. Increase in patient wait time and cost of sleep study were the balance measures.
We set a low improvement targets for outcome and process measures due to various reasons. (1) Clinic population had multiple comorbidities, with a limited time of 20–30 minutes for a follow-up visit. We had anticipated lack of sufficient time to address OSA screening in every patient with HTN in the clinic. (2) In a safety net IMC, patient population consisted of underserved, uninsured and vulnerable population. We had anticipated multiple barriers to acceptance of OSA screening and diagnosis. (3) Sleep studies were not performed in ECMC. Patients were referred outside of ECMC, with an anticipated long wait time for sleep studies. (4) This QI was for only 6 months in duration. We analysed data from electronic patient registry and created weekly statistical process control (SPC) chart for the process measure. Patients with HTN were eligible for OSA screening if they were not screened at any previous visits. During 6 months of this QI, patients were counted more than once if they were eligible during any clinic visit.
Design
We used the Specific, Measurable, Achievable, Relevant and Timely (SMART) technique to define the aim. We used the Plan-Do-Study-Act (PDSA) model for QI.30 The QI team consisted of attending physicians, residents, a social worker, nursing, administrative and IT staff. We performed root cause analysis in a small group discussion with a team to identify barriers to acceptance of OSA screening and diagnosis (figure 1). We identified the materials/methods, provider and patient-related barriers. The materials/method barriers included: (A) lack of electronic database; (B) lack of trackable documentation; and (C) unavailability of a customised STOP-BANG tool in the EHR. The provider barriers included: (A) lack of knowledge about the relationship between HTN and OSA; (B) lack of reminders to use screening tool; and (C) extra time needed during patient visits to complete the STOP-BANG screening tool. The patient barriers included: (A) lack of knowledge about OSA and a sleep study; (B) cost of the sleep study; (C) lack of transportation; and (D) lack of insurance coverage. We addressed the identified barriers and developed interventions to improve the screening rate (figure 1).
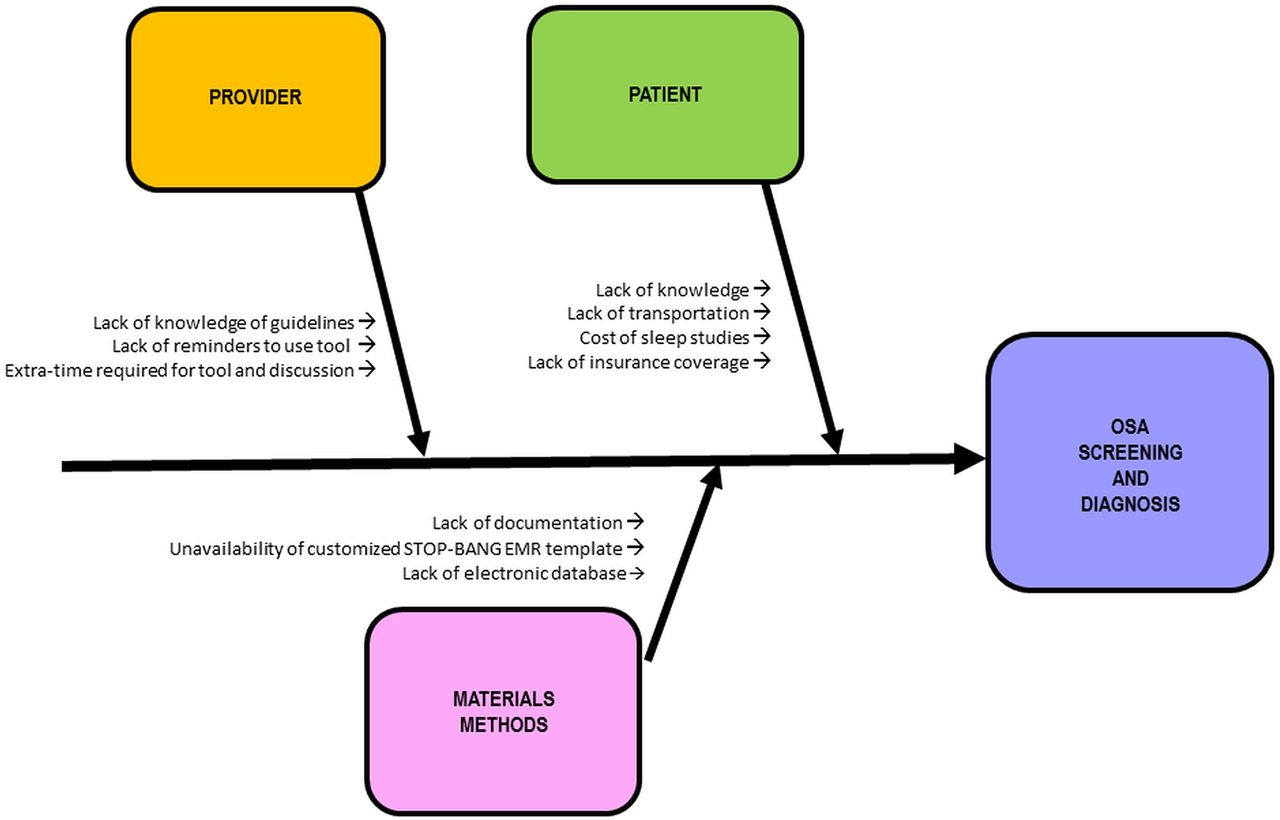
Fishbone diaphragm: root cause analysis identifying barriers to acceptance of OSA screening. OSA, obstructive sleep apnoea; STOP-BANG, loud Snoring, Tiredness, Observed apnea, high blood Pressure-Body mass index, Age, Neck circumference, and Gender.
Strategy
PDSA cycle 1 (June–July 2015: integration of customised workflow in the EHR)
In collaboration with the IT department, we created a customised EHR template to integrate the STOP-BANG screening tool in June–July 2015. Physicians were required to document the STOP-BANG score in EHR. The screening tool was incorporated into the ‘History & Physical’ section of the EHR. Physicians completed the STOP-BANG tool in EHR. We also created a customised template in the EHR to document patient-related barriers to acceptance of sleep study referral. Barriers of communication, knowledge, transportation and understanding of diagnosis and cost of a sleep study were included in the EHR checklist. Physician documented the barriers when patient disagreed for a sleep study.
PDSA cycle 2 (August 2015: physician education about OSA and EHR workflow)
In August 2015, we identified gaps in residents’ knowledge of OSA. We focused on educating physicians by PowerPoint presentation and small group discussions. We also provided education about EHR workflow for STOP-BANG tool documentation.
PDSA cycle 3 (20 September 2015: completion of STOP survey by patients, facilitated by nurses)
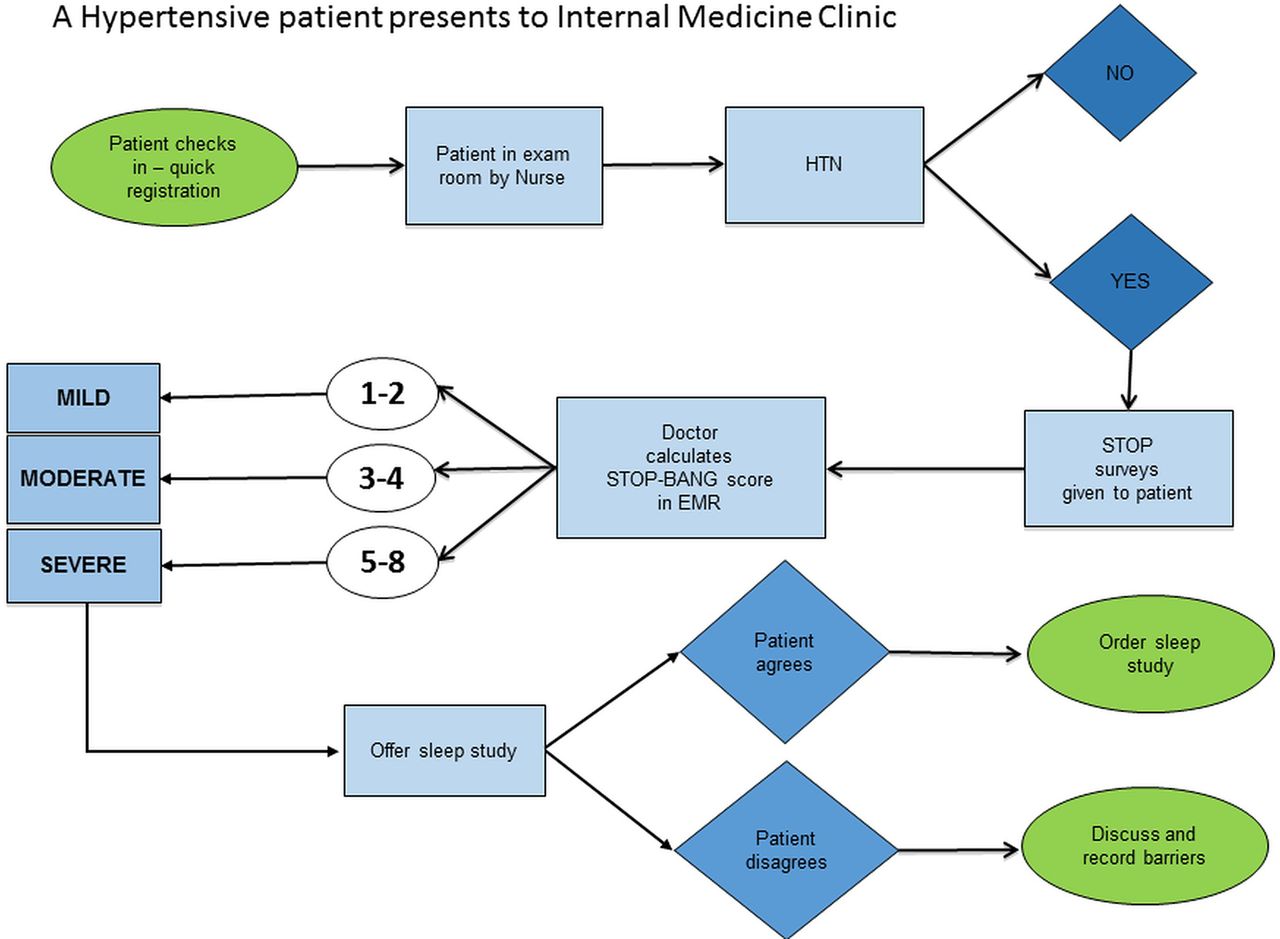
There was no automated EHR chart alert for physicians to perform STOP-BANG tool in EHR. We educated the nursing staff about the OSA screening project for the patient with HTN. We created a new workflow that included completion of the STOP survey by the patients on paper with facilitation by the nursing staff prior to the physician evaluation. This workflow was designed to remind physicians to use OSA screening tool and to improve efficiency. Physicians documented the results of STOP survey, completed by the patients and also completed BANG survey in the EHR. Physicians discussed the STOP-BANG score results with the patients. Physicians offered sleep study to patients with STOP-BANG score of ≥3 (intermediate to high risk) and discussed barriers for acceptance of a sleep study (figure 2). Physicians also educated the patients about possible complications of undiagnosed OSA. This patient-centred shared decision regarding sleep study occurred during the clinic visit. When patient refused a referral for a sleep study, the physician determined the reasons for refusal and documented in the EHR. The physician discussed various ways to overcome the barriers. Patients without insurance coverage for a sleep study were referred to a social worker for further assistance. When patients refused the sleep study when indicated by 3 or more STOP-BANG score, physicians discussed the need for a sleep study during subsequent follow-up visits. Physicians referred the patient, once the patient agreed for a sleep study. Once diagnosis of OSA was confirmed, physician referred the patients to sleep medicine or pulmonary medicine specialist for the treatment.
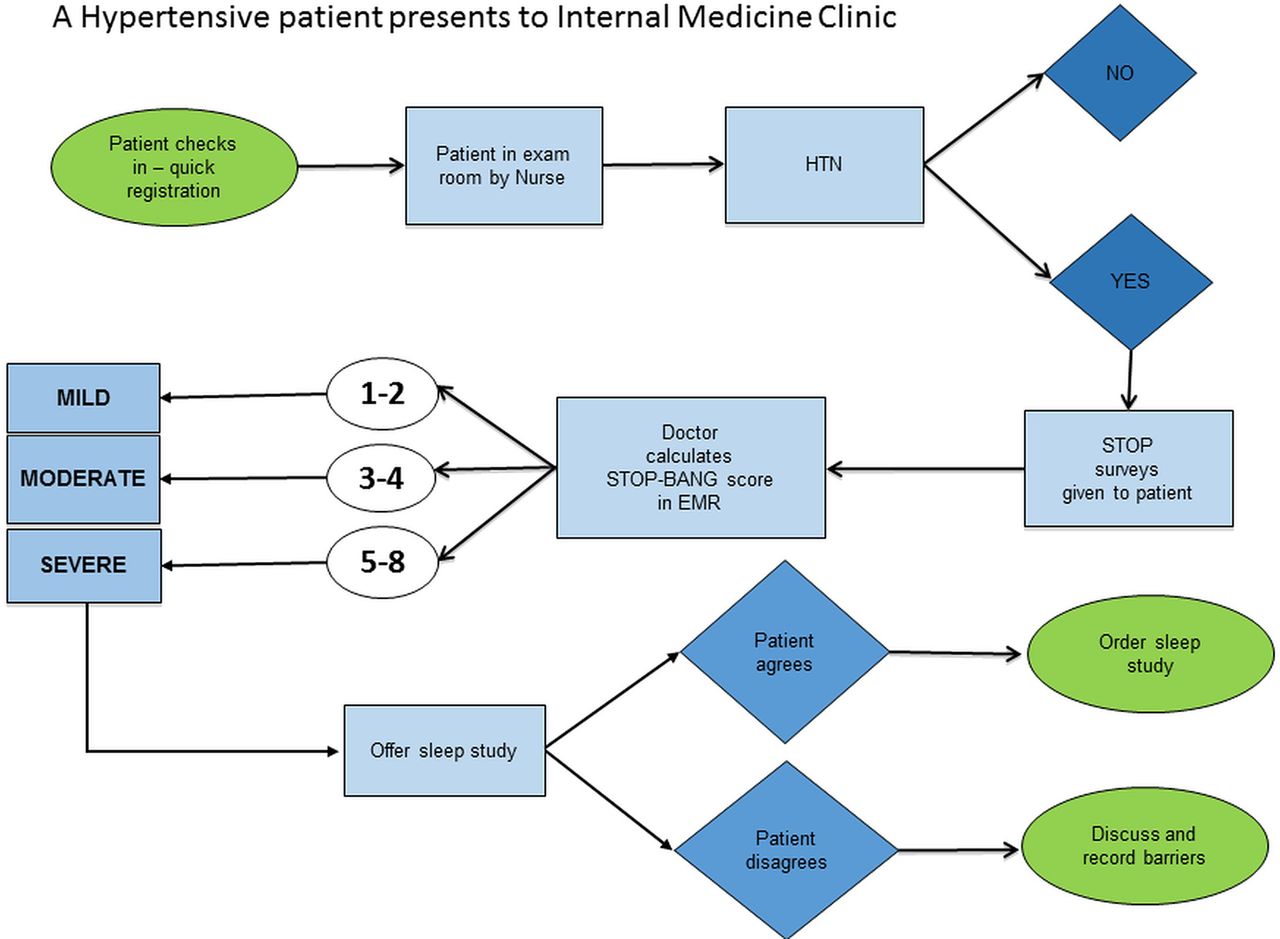
Process workflow chart. HTN, hypertension; STOP-BANG, loud Snoring, Tiredness, Observed apnea, high blood Pressure-Body mass index, Age, Neck circumference, and Gender.
Results
Process measures
Improvement in physician knowledge
After the first PDSA cycle of integration of customised workflow of STOP-BANG screening tool in the EHR, OSA screening rate did not change significantly. This was explained by the lack of physician knowledge about OSA and unawareness of the new EHR tool based on residents’ anecdotal reports. We conducted a pretest to assess gaps in residents’ knowledge, prior to providing the education. Pretest consisted of five questions on OSA; residents answered only 58.3% of questions correctly. However, we did not perform the post-test to assess objective evidence of any improvement in the resident’s knowledge.
Percentage of patients with HTN screened for OSA with the use of the STOP-BANG screening tool
We plotted a weekly SPC chart for the process measure of the percentage of patients with HTN screened for OSA (figure 3). After the first PDSA cycle, the screening rate did not increase significantly (2.86% increase in the week of 5 July 2017) resulting in unsustainable variation in subsequent weeks. After the second PSDA cycle in August 2015, the screening rate did not increase significantly (2.86% increase in the week of 23 August 2015) resulting in an unsustainable variation. After the third PDSA cycle (completion of STOP survey by patients, facilitated by nurses), on 20 September 2015, OSA screening rates increased to 11% at the end of the week. However, this increase was not sustainable. There was significant weekly variation during the subsequent weeks. In the week of 8 November 2015, the rate was increased to 17%, which subsequently decreased and then increased to 14.5% in the week of 29 November 2017. There was also significant weekly variation in the screening rates in December 2015, resulting in an increased rate of 11.83% in the week of 27 December 2015. We achieved an average of only 3.88% increase in OSA screening using STOP-BANG tool during the 6-month period. Significant weekly variation may be explained by residents rotating every 5 weeks, spending 1 week at a time in the clinic. The increase in screening rate may be from active participation of assigned residents in this project. Over 50% of the patients completed the STOP survey; however, physicians were unable to document and discuss all completed STOP paper surveys in the STOP-BANG tool in the EHR. Physician’s barriers to acceptance of screening included: (1) lack of electronic chart alerts; and (2) lack of extra time needed to complete the STOP-BANG tool during the clinic visit while addressing multiple chronic diseases. The clinic population had multiple chronic diseases, and patients were scheduled every 20–30 minutes for physicians for a follow-up clinic visit. We had anticipated the lack of sufficient time to address OSA screening in every patient with HTN in the clinic. The variation seen in relation to the PDSA cycles was not sustainable.

{kind=link}
{kind=link}
{kind=link}
Weekly statistical process control (SPC) chart showing percentage of patients with hypertension screened using STOP-BANG questionnaire. CL, control limit; LCL, lower control limit; PDSA, Plan-Do-Study-Act; STOP-BANG, loud Snoring, Tiredness, Observed apnea, high blood Pressure-Body mass index, Age, Neck circumference, and Gender; UCL, upper control limit.
Outcome measure
From July 2015 to December 2015, 32% of patients scored ≥3 on the STOP-BANG (n=318/1000) survey. Patients with a STOP-BANG score of ≥3, 10.4% (n=33/318) had a confirmed diagnosis of OSA. Sixty-three patients scored ≥5 on the STOP-BANG survey. Seventy per cent (44/63) of patients agreed for a sleep study referral. Thirty-three patients were diagnosed with OSA. Of the 255 patients with STOP-BANG score of 3–5, about 50% agreed for sleep study referral. However, most of the sleep studies were not completed within 6 months due to multiple barriers. We achieved a 3.3% increase from the baseline rate of less than 1% OSA diagnosis in IMC patients with HTN. We were unable to achieve any significant increase in OSA diagnosis rate within 6 months in the IMC patient population due to multiple reasons: (1) the majority of the patients had the sleep studies scheduled at later dates due to long wait time for sleep study appointment; (2) we identified various barriers for acceptance of sleep study including fear of sleep study procedure, fear of diagnosis and treatment using CPAP and cost and lack of transportation for sleep studies. Out of 33 patients with a confirmed OSA diagnosis, 22 patients had sleep study report in the EHR and 11 patients did not have sleep study report. However, there was a medical documentation in the EHR indicating patient’s history of confirmation of OSA diagnosis from the sleep study and were under care of the sleep/pulmonary specialist for the treatment. Sleep studies were not performed in ECMC; we did not receive reports of all completed sleep studies and pulmonary/sleep medicine physicians’ reports IMC physicians had requested the medical records for the sleep studies. We did not achieve our goal of 10% increase in OSA screening (process measure); therefore, we were unable to significantly impact increases in OSA diagnosis (outcome measure).
Balancing measures
Patient backlog
The extra time used on the screening tool did not result in any patient backlog in the clinic. This was determined by anecdotal reports of lack of patient complaints for a long wait time and lack of overtime for clinic staff during this project. The baseline time for the cycle time of a follow clinic visit was an average of 1 hour from start of the registration to patient discharge. We did not measure actual cycle time during the project.
Cost of the sleep studies
There was a definite concern regarding sleep study cost in our patient population due to a higher copay or lack of insurance coverage. This was documented by physicians in EHR under barriers for acceptance of sleep study; however, we were unable to retrieve accurate percentage of patients who refused sleep study due to cost reasons. During follow-up clinic visits, patients reported to the physicians that cost of sleep study was the reason for not completing the sleep study.
Discussion
Summary
OSA is more prevalent in patients with HTN and obesity than in the general population.2 6 18 However, many patients with HTN have undiagnosed OSA. In the IMC population, over 70% of the patients have a diagnosis of HTN with a mean high BMI of 32 (obesity=BMI of 30 or greater8). Our baseline data showed that less than 1% of patients with HTN were screened and diagnosed with OSA. These data indicated that OSA screening and diagnosis in patients with HTN and obesity was underutilised in our IMC. The aim of this QI project was to increase OSA diagnosis from the baseline rate of less than 1%–5% in patients with HTN between the ages of 18–75 years over a 6-month time period using the STOP-BANG sleep apnoea screening tool in IMC.
The average increase in OSA screening rate using the STOP-BANG tool was 3.88%. The significant variation seen in relation to PDSA cycles was not sustainable. Thirty-two per cent of patients scored ≥3 on the STOP-BANG tool and 10.4% had a confirmed diagnosis of OSA. OSA diagnosis was increased to 3.3% in IMC patient population within the 6-month period.
This QI project has several strengths. We were able to identify various barriers to OSA screening and diagnosis in IMC patient population with continuous feedback from the patients and the team members. We achieved an unsustainable increase in OSA screening rate during few weeks with engagement of the assigned residents. OSA diagnosis was increased to 3.3% in IMC patient population within the 6-month period with multiple barriers for OSA screening and diagnosis. Low OSA screening rate and various patient-related barriers to acceptance of the sleep study resulted into insignificant increase in percentage of OSA diagnosis. This QI did not result in any increase in opportunity costs.
We learnt important lessons from this project. Engagement of a multidisciplinary team in performing the root cause analysis was crucial to the design of this project. The team outlined various barriers and designed strategies to overcome the barriers. In collaboration with the IT department, we created an innovative workflow to calculate and document a STOP-BANG score within the EHR. We created chart alerts to remind physicians to screen for OSA. However, manual calculation and documentation of the STOP-BANG screening tool in the new workflow added extra steps, resulting in an increase in physician time during the patient visit. Lack of automated and integrated EHR algorithm support to calculate and document STOP-BANG screening tool and clinical decision support to prompt physicians to order sleep study referral for high STOP-BANG score was found to be the greatest system barrier. The ECMC IT department evaluated the possibility of purchasing an automated EHR screening tool and the cost was identified as a major barrier to the implementation.
Physicians felt that there was insufficient time to address and document OSA screening in every patient with HTN. This was based on physicians’ anecdotal reports of lack of sufficient time to address multiple problems in our clinic population during clinic visit. The physicians identified patient-related barriers for acceptance of sleep study referral, which included lack of patient knowledge about complications of undiagnosed and untreated OSA, fear of overnight stay in the sleep laboratory for sleep study and concern about cost of sleep study and insurance coverage.
Limitations
This QI project has several limitations. (1) There was a lack of sustainable intervention for OSA screening in patients with HTN in the clinic due to identified EHR, physician and patient-related barriers. (2) This QI project was conducted for a short period of 6 months and we were unable to follow-up on the results of sleep study due to long wait time for the sleep study appointments. (3) We did not conduct post-test to evaluate objective improvement in physician knowledge after the completion of the physician education. (4) There was a lack of internal validity; we were unable to demonstrable meaningful impact or change resulting from different PDSA cycles during QI project. (5) We were unable to design weekly SPC chart for the outcome measure of OSA diagnosis due to various reasons. (6) This QI was performed in a safety net primary care clinic in patients with multiple comorbidities, so the results cannot be generalisable to other settings.
Conclusions
The aim of this QI project was to improve OSA diagnosis in hypertensive clinic population with the use of the STOP-BANG screening tool. Integration of the screening tool in the EHR, physician and nursing education and a team-based approach did not lead to a sustainable increase in OSA screening. Lack of EHR automation and lack of sufficient physician time were identified as major barriers for acceptance of OSA screening in IMC. Thirty-two per cent of patients scored ≥3 on the STOP-BANG (n=318/1000) tool and 10.4% (n=33/318) had a confirmed diagnosis of OSA. We achieved a 3.3% increase from the baseline rate of less than 1% OSA diagnosis in IMC patients with HTN. There was no significant increase in OSA diagnosis during 6 months of the QI project. Overcoming barriers to acceptance of sleep studies and improving the referral process for sleep studies may result into timely diagnosis of OSA and treatment. Long waiting time for the sleep study appointment, cost of sleep studies, lack of insurance coverage and patient knowledge regarding OSA were identified as major barriers resulting in the delay of diagnosis of OSA in the IMC.
The future project will focus on a longer time period of at least 18 months in duration. PDSA cycles will focus on shifting the responsibility of calculating and manually entering OSA screen in EHR from the physician to the nursing staff. This shift may allow for more time for the physician to spend educating and discussing barriers to acceptance of OSA screening with the patients. The future PDSA cycles will also include patient education by providing brochures about OSA. There was a minimum cost involved in conducting this QI project. The team planned to make interventions sustainable by using frequent EHR reminders for physicians and engaging nursing staff to calculate and enter STOP-BANG score in EHR as a part of routine care in patients with HTN in the clinic.
Acknowledgments
We would like to thank the administrative staff, IT department and clinic nursing staff of ECMC.
References
Footnotes
Contributors SYB: performed research and writing. MN and MS: performed research. AK: performed research. JLR: writing
Competing interests None declared.
Ethics approval Based on local policy, this work was deemed as an improvement study and not a research study on human subjects as patients were not affected directly, and their treatment was not altered nor were they given an experimental or novel therapy. The local research policy was met, and ethical approval was not required.
Provenance and peer review Not commissioned; externally peer reviewed.