Article Text

Abstract
Prolonged waiting times and length of stay in Pediatric Emergency Department, are the two of the most challenging patient and clinical outcomes of healthcare institution. These emerged due to various reasons, namely: the use of triaging process and patient flow criteria that eventually lead to bottlenecks and overcrowding in the ED. After realizing the root causes of the prolonged waiting times and length of stay, the KASCH ED instigated a team to study the factors and thereby arrive at a considerable conclusion that will result in an improvement.
The quality improvement project was initiated and steps were undertaken to improve the flow, reduce the waiting times, and reduce the overcrowding in Pediatric Emergency Acute Care Unit. The primary cause identified was inadequate team awareness and lack of the ED process flow, thus creating confusion as to where the type of patients based on the triage level will be assessed, managed and treated. Using the Canadian Triage and Acuity Scale (CTAS) as guide in triaging patients, a theory called Pediatric Rapid Assessment and Management (PRAM) was introduced in the Acute Care Unit. This certain model is basically aimed to rapidly assess and managed the patients who were triaged as Level III and Level IV within a period of 30 minutes.
Several PDSA cycles were tested and implemented in order to assure that the process fit the criteria and the process flow will be improved. Following the completion of each cycle, significant improvements were noted, such as patients being assessed in Initial Assessment Room on average time less than the target of 15 minutes. In like manner, patients' length of stay on average less than 15 minutes in PRAM bed. The total time for assessment and plan of management is with a target time of less than 30 minutes. The team continuously drive th process and monitored the key performance indicators of the PRAM during the study period and subsequent improvement strategies were likewise implemented.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
King Abdullah Specialized Children's Hospital (KASCH) was opened in April 2015 as a tertiary academic medical center in Riyadh. KASCH has an Emergency Department (KASCH-ED) which consists of 4 Units: Triage, Urgi-care Center (UCC), Pediatric Acute Care (PAC) and Resuscitation Unit (RU). In Triage, the capacity is 9 rooms; 5 of these 9 rooms are utilized for initial assessment. The patients are usually assessed by a nurse to identify the level of acuity based on Canadian Triage and Acuity Scale (CTAS) triage scale. The CTAS levels ranges from level I representing the highest priority patients to level V representing the lowest priority patients.
Whenever a patient passes through triage and their CTAS level is III or IV with specific criteria, the patient will be brought from Triage to the Pediatric Acute Care Unit (PAC). The patient will be evaluated by a nurse and vital signs will be taken. The patient will be waiting in PAC for a bed for a maximum of 15 mins. If a bed is available, the patient will be moved to be assessed by a physician and a nurse to establish the initial plan and management within a 15 min target time. This corresponds to a total length of stay in PAC of 30 min for plan of management. These target times represent the institutional target determined for KASCH-ED. After a plan is completed, the patient will be moved to a definitive area of care within a maximum of 15 min time limit.
The ED goal is to achieve a maximum length of stay of 4 hours or 6 hours if any consultation is made. Our standard criterion has been adapted from Toronto Western Hospital, where they also have defined the target time of 4 hours for patients to be assessed, treated and discharged (3). These new timings were outlined to reduce the length of stay of patients in the Pediatric Emergency Department and reduce the overcrowding, aiming to identify and eliminate variations in clinical processes. The data collected can reflect that ED crowding is not just ED problem, but a wide hospital issue that needs to be addressed as one.
In December 2015, the KASCH-ED had a total of 68,233 patients, of which 19,788 (29%) were seen in the Pediatric Acute Care Unit. These numbers show that KASCH-ED faces crowding and patient flow issues that could lead to delays in timely patient management and decision. These problems were identified based on our analysis of our daily KPI's, where we monitor 24 hours of performance and timings, including the delays in patients' disposition – ie the plan for continuing health care of a patient following discharge from each ED area. More specifically, there were noticeable delays of patient flow in the Acute Care area with no proper functioning flow process in place, leading to crowding and a bottle neck of patient flow in or out of the ED.
The development aims of this QI Project were to reduce the overcrowding of patients in the PAC section of the ED by 50% by August 2016 with the purpose of delivering the best care for our patients through:
Have in place a flow chart outlining a systematic Rapid approach process for assessing pediatric patients
This process be 100% implemented between the nurses and the physicians as evidenced by appropriate documentation
Balancing measure: without compromising the quality of patients' care
Process measure: establishing time frames (15 min in each area)
Background
KASCH Emergency Department uses the Canadian Triage and Acuity Scale (CTAS) to triage patients based on their presenting complaints, vital signs and selected modifying factors. The role of triage in a hospital emergency department is to assign priority to patients who seek urgent care while identifying patients for whom examination by a physician can be deferred.1–3 Several studies demonstrated that there is an ongoing increase in waiting time and crowding in emergency departments (EDs) worldwide.4 Thus, Triage plays an important role in such situations to avoid a long waiting time to be treated by a physician and to appropriately prioritize patient flow in the Emergency Department. In children's hospitals in numerous countries from Asia, the European Union, and North America patients are triaged on arrival to the ED with a standardized triage tool called the Canadian Triage and Acuity Scale (CTAS) developed by Gravel et al.2 The CTAS levels are designed such that level I represents the highest priority patients and level 5 represents the lowest priority patients. Level I resuscitation, level II emergent, level III urgent, level IV less urgent, level V non-urgent.
The team explored the factors leading to increased length of stay in PAC, creating a Fishbone Diagram. Prioritization of the causes of increased length of stay in PAC was done utilizing the Pareto (80/20 principle), see supplementary material.
supplementary data

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Baseline measurement
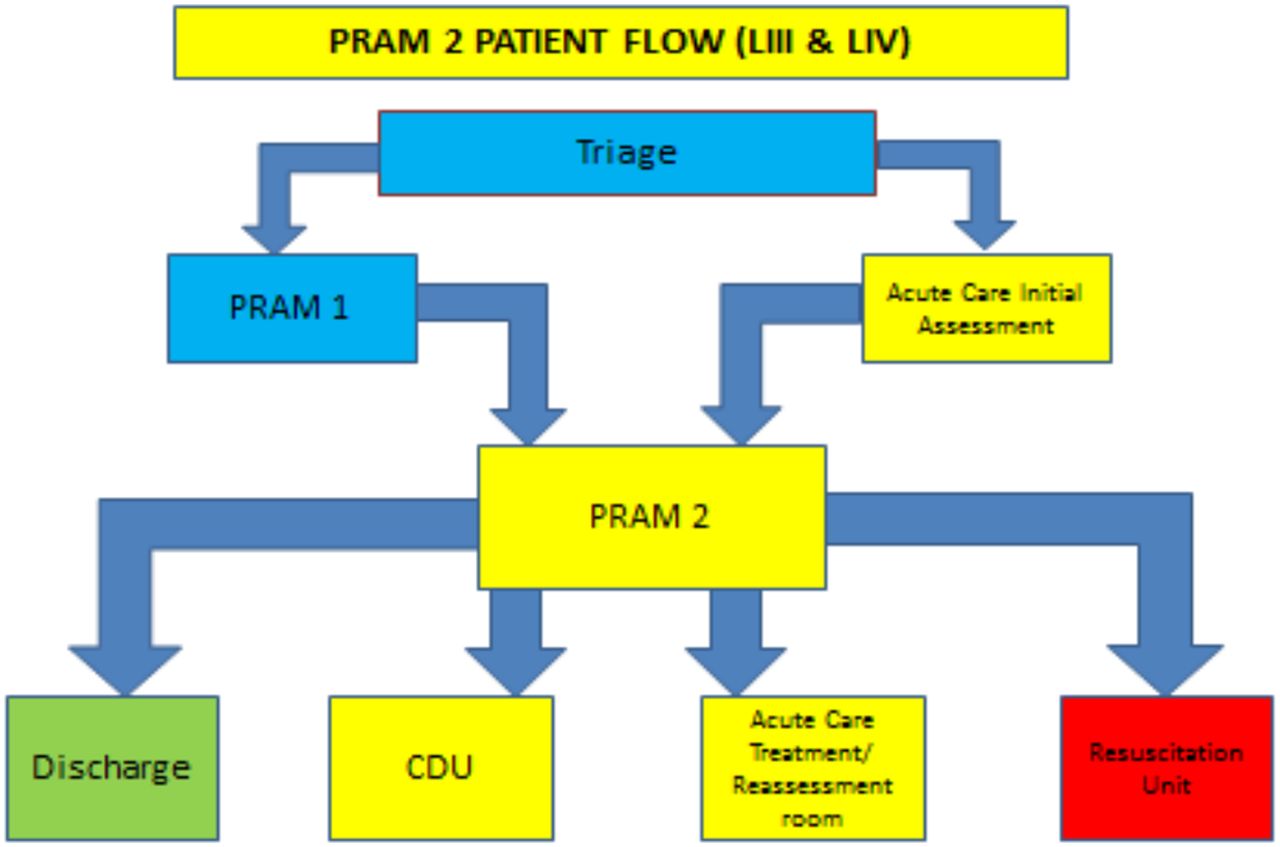
The quality improvement project was initiated and steps were undertaken to improve the flow, reduce the waiting times, and reduce the overcrowding in the Pediatric Acute Care Unit (PAC). The primary cause identified via the Pareto chart was inadequate team awareness and lack of ED process flow, thus creating confusion as to where the type of patients based on the CTAS triage level will be assessed, managed and treated (Figure 2).
It was decided to introduce a theory called Pediatric Rapid Assessment and Management (PRAM) to the Acute Care Unit. This model aimed to rapidly assess and managed the patients who were triaged as Level III and Level IV within a period of 30 minutes.
PRAM was introduced in March 2016 with the intent of shortening length of stay and facilitating the rapid turnover of patients in the PAC section of the Emergency Department. The baseline data were collected from the initiation of the project in March 2016 by utilizing an audit tool to track the patients being received in PAC. The main measures were:
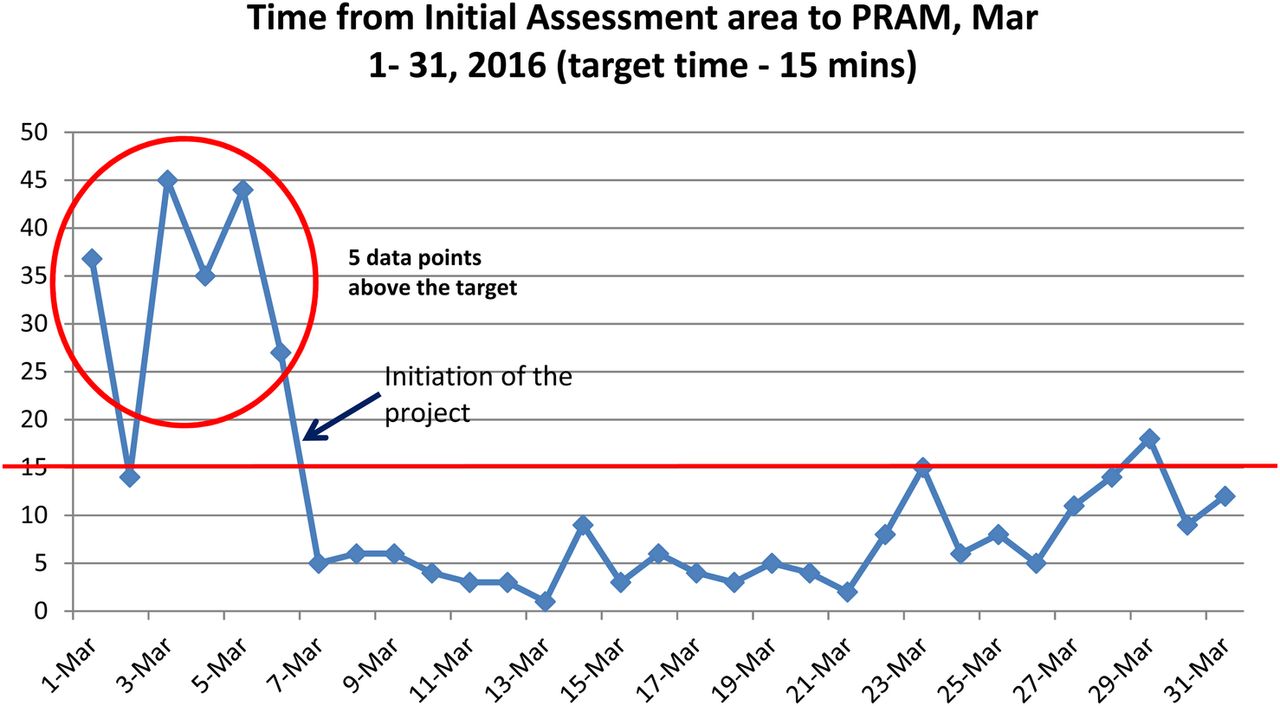
Average time from initial assessment area to PRAM (target: 15 minutes), (Figure 1).
Average time in PRAM bed (target: 15 minutes), (see supplementary material).
In aggregate, these represent:
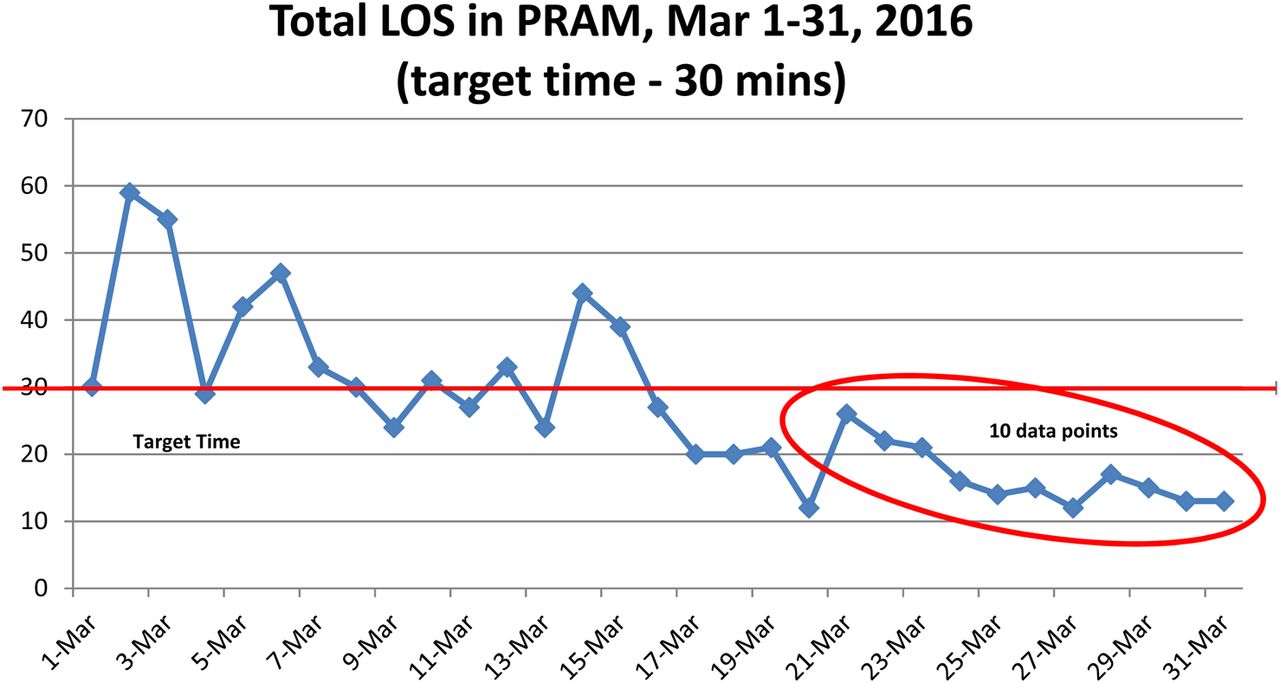
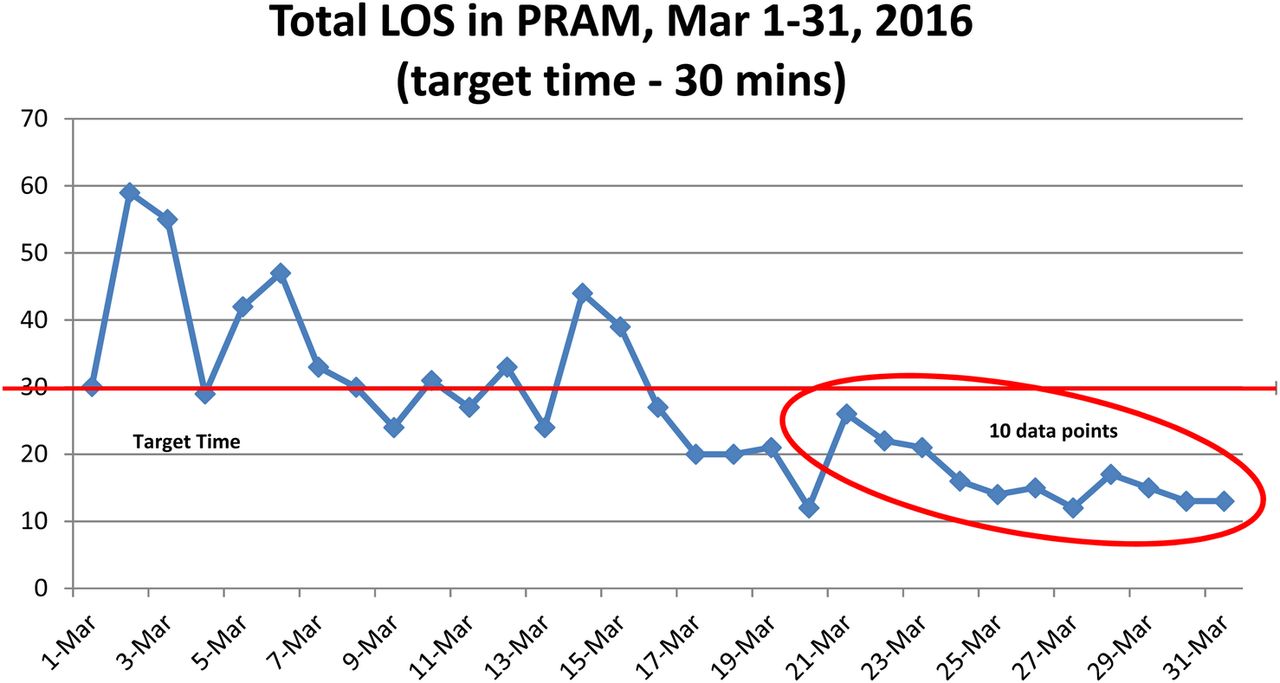
Total length of stay in PAC (target: 30 minutes), (Figure 3)
supplementary data
These KPIs were monitored during the initial phase of the project, see Figures (1 & 3). The data was collected on a daily basis, through the use of an audit tool which designed by the QI Project Team; the graphs with a monthly average, see supplementary material.
supplementary data
At the outset, PRAM had no specific process flow or designated area, thus the data were collected at the time based on the number of patients that would come to PAC assessed as CTAS triage level III. Several interventions took place in order to establish accurate data collection and thereby arriving at absolute figures or data.
Design
In March 2016 the Pediatric Rapid Assessment and Management (PRAM) model was introduced to the Emergency Department. It was introduced both in the Triage section with 4 out of 9 triage beds designated as PRAM 1 and into the Pediatric Acute Care Unit specifically, where it was designated as PRAM 2. This project focuses specifically on the introduction of PRAM into the Pediatric Acute Care Unit.
Guidelines for PRAM were created and implemented so that patients who were triaged as level III and level IV could be assessed against the Inclusion Criteria created in the PRAM guidelines, be seen in the Pediatric Acute Care Unit and assessed, managed and treated accordingly. The PRAM model was utilized to assess all patients CTAS level III and level IV within set inclusion criteria categorized in the PRAM guidelines.
The criteria included all patients with Triage level III except respiratory conditions mainly Asthma, Bronchiolitis, and Croup. CTAS level IV patients include patients with cardiac disorders, Organ transplant patients, Stem cell transplant patients, Bone marrow transplant patients, Renal failure patients, Hepatic failure patients, Oncology patients (not febrile neutropenia), patients with Metabolic disorders and patients with Diabetes Mellitus. Many other Triage level V patients were also included.
At the outset, challenges were encountered in enhancing the PRAM as a structure, however, through continued dedication of the team, by continuous 24 hours monitoring by drive nurses, accurate data collection and appropriate data management and treatment, PRAM is set to achieve the desired outcomes.
Strategy
Several PDSA cycles have been run to test the change ideas described as follows:
PDSA Cycle 1: Introduction of the Pediatric Rapid Assessment and Management (PRAM) model
Aim: To introduce the concept of the Pediatric Rapid Assessment and Management (PRAM) model in the Pediatric Emergency Department. The specific objectives of this cycle were:
Designating the specific rooms for PRAM and assignment of dedicated staff to man the area.
Educating the Pediatric Emergency staff regarding PRAM process.
Creating a process flow chart.
Plan:
Physically identify the rooms designated to be used for Pediatric Rapid Assessment and Management in the PAC Unit. There are four rooms assigned – 1 bed for initial assessment room, 3 beds are allocated for PRAM (known as PRAM 2).
The PRAM process flow was initiated and disseminated to all Pediatric Emergency Department staff (Figure 2)
In service/educational sessions were conducted to all Pediatric Emergency Department staff focusing on the importance of familiarizing themselves with the function of the Pediatric Rapid Assessment and Management in the Pediatric Acute Care Unit.
Prediction: The QI Project Team anticipated that the with the above-mentioned strategies, the Pediatric Emergency Department staff will be able to perform their duties well and that patients are seen in a timely manner.
Do: The cycle number 1 was initiated in March 2016. A QI Project Team comprising of the Nurse Manager, Clinical Resource Nurse, and several expert staff nurse in the area collaborated to commence this improvement initiative.
Study: In this phase, the success rate gained from educating the Pediatric Emergency staff was elevated to 90% in May 2016 compared with the Initial rate of 70% during the kick off phase in March 2016. The designated rooms were utilized by the staff up to 70% in May 2016 compared to 50% in March 2016 with appropriate implementation of the process flow chart.
Act: There were consistent reminders from the PRAM 2 Team Nurse Team Leader as to the adherence to the PRAM 2 process as mentioned in the 3 Aims of the PDSA cycle 1. The result of the Cycle 1 led to test the idea of the PDSA cycle 2 of structure and process of the Pediatric Rapid Assessment and Management (PRAM).
PDSA Cycle 2: Creating the structure of the Pediatric Rapid Assessment and
Management (PRAM)
Aim: To create the structure and process of Pediatric Rapid Assessment and Management in the Acute Care Unit by establishing guidelines to assess, manage and treat the patients referred to the PRAM.
Plan:
Create comprehensive PRAM Guidelines that will assist the entire Pediatric Emergency Department team to appropriately assess, manage and treat the patients referred to PRAM.
Develop an audit tool to track and monitor the patients' length of stay in the Pediatric Rapid Assessment and Management Area.
Prediction: We projected that the PRAM guidelines will facilitate the timeliness and efficiency of the healthcare service delivery to the pediatric patients. In the same way, we anticipate that the data gathered utilizing the audit tool will assist the team in analyzing the causes of prolonged length of stay of pediatric patients in the PRAM area.
Do: Auditing and monitoring of the patient's length of stay in the PRAM were conducted by the members of this QI project.
Study: During this cycle, data from all patients who exceeded the expected time frame (more than 20 minutes) in PRAM were studied for 1 week. Data analysis was done on all the patients who had a length of stay (LOS) above 20 minutes to identify the causes; see the fishbone diagram. The main cause of delays identified were the lack of a team leader in PRAM to drive patient flow and lack of awareness of physicians and nurses about the time that patients should stay in each area, i.e. 15 minutes in the Initial Assessment Room and 15 minutes in a PRAM bed with a total LOS of 30 minutes.
Act: The causes of the delays in the PRAM were carefully dissected, analyzed and reported to the Chairman of the Pediatric Emergency Medicine Department during the daily Clinical Operations meeting.
PDSA Cycle 3: Resolving the Root Causes of the Delays in PRAM
Aim: To recognize and resolve the identified root causes of the delays in Pediatric Rapid Assessment and Management in the Acute Care Unit by scrutinizing the specific reasons.
Plan:
To carefully study the reasons for the delays that were due to several factors (wait for Consultant decision, Physician assessment at the bedside, availability of Physician and during handover) and formulate an action plan to resolve the issue. The action plan will be presented to the Chairman of the Pediatric Emergency Medicine Department after approval from the team. The Chairman then will notify the division heads to inform the Physicians regarding the factors of the delays mentioned above.
Prediction: We expect to notice an improvement in the delays, after disseminating the information to the Physicians and with the nurses driving the flow. There will be a cohesive approach in the whole Pediatric Emergency department to the treatment and management of pediatric patients.
Do: The division heads and designees conducted a daily debriefing as to the PRAM guidelines and the reasons for delays. The Physicians who were assigned in the PRAM area were instructed to strictly adhere to the time frames specified in the guidelines.
Study: In May 2016 the team reviewed a total of 277 patient delays in PRAM (see supplementary material). 31.76% was due to waiting for Consultant's decision, 28.1% was because of Physician's assessment at bedside, followed by 26.35% which was due to unavailability of Physicians. Only 9% was due to handover and 4.6% was due to other reasons including Physician's not being able to see patients because they are busy elsewhere.
supplementary data
In June 2016, the team reviewed a total of 82 patient delays in PRAM (see supplementary material). 26.8% was due to waiting for Consultant's decision, 34.1% was because of Physician's assessment at bedside, followed by 21.9% which was due to unavailability of Physicians,10.9% was due to handover and 0.06% is due to other reasons including Physician's not being able to see patients because they are busy elsewhere.
In July 2016 the team reviewed a total of 118 patient delays in PRAM (see supplementary material). 8.4% was due to waiting for Consultant's decision, 28.8% was because of Physician's assessment at bedside, followed by 38.1% which was due to unavailability of Physicians, 21.1% was due to handover and 3.3% is due to other reasons including Physician's not being able to see patients because they are busy elsewhere.
PDSA Cycle 4: Controlling and Sustaining the Improvement Strategy in PRAM
Aim: To continuously monitor, review and evaluate the progress of the Pediatric Rapid Assessment and Management in the Acute Care Unit by tracking patient delays of more than 20 minutes.
Plan:
The QI project team to consistently monitor the patient delays in PRAM using the audit tool and identify the specific cause of the delay. Once identified, the team will notify the division heads and the Chairman to act on these causes, discussing a particular course of action with individual physicians if appropriate.
Prediction: We strongly believe that the Physicians with the collaboration of the nurses, will result in a well-organized and systematic Pediatric Rapid Assessment and Management that will eventually reduce patient delays and increase positive patient outcomes.
Do: The QI Project Team carried out regular meetings to tackle the observations and audit results. Also, the team leader updates the Chairman during the Clinical Operations meeting in respect to the flaws of the PRAM process flow. In order to rectify the defects of the PRAM process flow, the team formulated an Escalation process to address the issues of delays and overcrowding.
Study: In July 2016, the PRAM key performance indicators yielded as follows: The average time from initial assessment area to PRAM with a timeframe of 15 mins is 7 minutes, average time in PRAM Bed with a total timeframe of 15 mins is 12.5 minutes, while the average Length of Stay in PRAM with a timeframe of 30 mins is 19.6 minutes. We are still facing some challenges recently as evidenced by the prolonged stay of patients in the PRAM beds in some days. These are attributed to influx of patients and the unavailability of enough physicians to assess the patients.
Act: These KPIs were monitored on a daily basis and reported to the Chairman of the department. The division heads are constantly notified to impose the PRAM guidelines and strictly adhere to the protocol.
Results
After one week of the initial intervention on March 2016, there was a dramatic drop in the total length of stay in PRAM area from 60 minutes to less than 30 minutes, see figures (1, 3) and supplementary material.
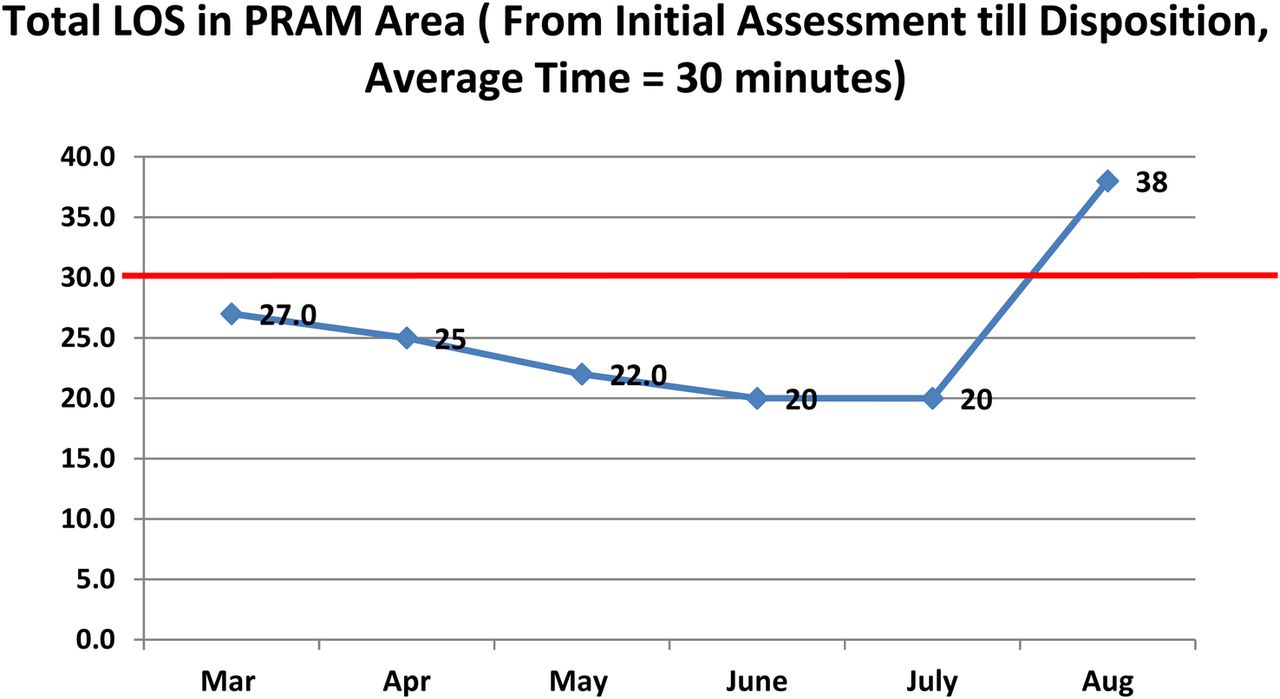
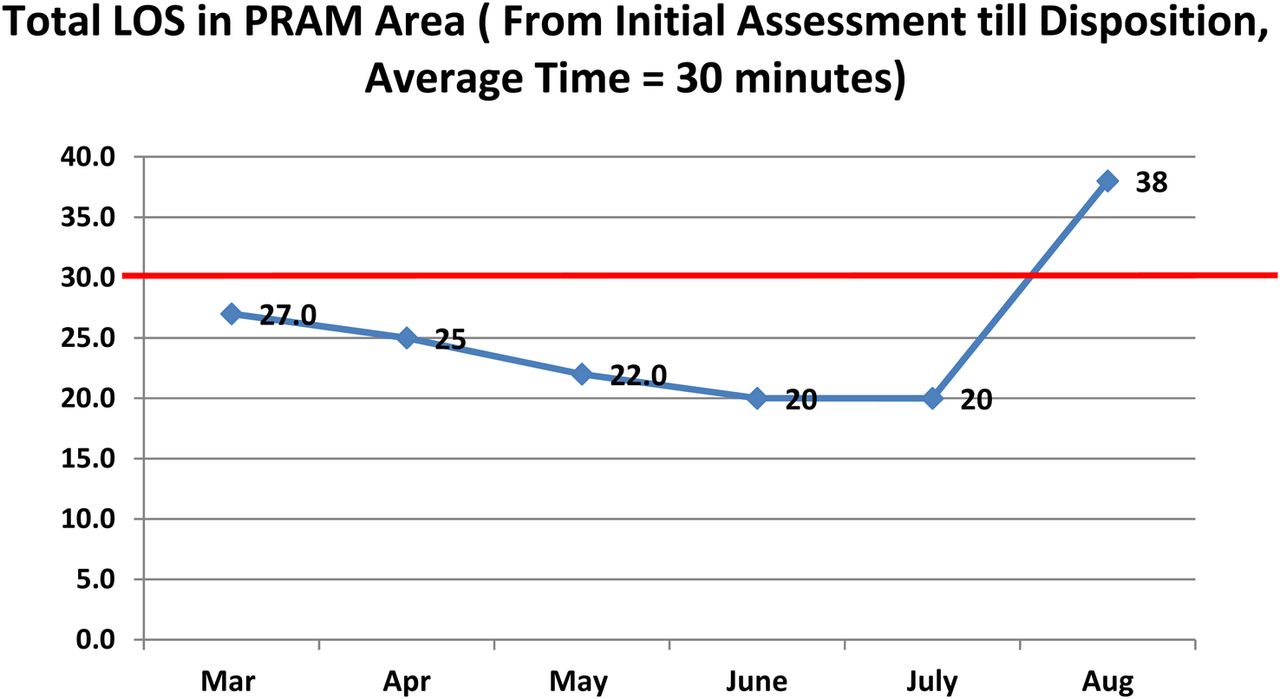
The length of stay continued to be less than 30 minutes between (total targets) in both initial assessment time and PRAM Room time until August 2016, see Figure 4.
On August 2016, the PRAM key performance indicators yield evidence of delay with initial assessment time of 15 minutes and the PRAM Room time of 23 minutes with a total average length of stay of 38 minutes. This challenge was attributed to shortage of rotating junior physicians and shortage of senior ED physicians due to leaves and summer vacation.
Lessons and limitations
The PRAM project is a milestone quality improvement introduced in KASCH Pediatric Emergency Department. Our target population is now acknowledged as patients assessed as Level 3 and Level 4 based on CTAS Triage with set inclusion criteria. The lower number of patients during the summer season in the Acute Care provided us a good opportunity to study the defects of the delays in the PRAM. However, this quality improvement project is still anticipated to look at the through puts in the winter season where the highest volume of patients will surge in the Pediatric Acute Care Emergency Department. We then would like to evaluate and draw a conclusion so that contingency measures could then be established which will be implemented all throughout the year. Our analysis of delays will continue based on the daily KPI's performed in the Unit. With this, we aim to maintain and sustain the results and in case of setbacks in the timings we will be able to tackle and correct it in a timely manner that will not affect our performance.
During the PDSA cycles, we encountered issues in that some nurses and physicians took more time to accept the changes being implemented. For the nurses, we find it easier to rectify as it only required in-service education and one-to-one coaching, but for the physicians, this concern became more challenging due to the Physician's monthly rotation and inadequate orientation prior to their assignments in the Acute Care Department that leads to some delays in the PRAM assessment. This was discussed with the Chairman of the department of Emergency Pediatrics, and the Program Director of Residents and they are willing to introduce the Guidelines of PRAM as part of the orientation for the residents in rotation within the unit.
Communication was one barrier, due to the diverse nationality that prevails in our Pediatric Emergency Department settings, and the cultural sensitivity of the population in understanding that the priority is according to the Triage acuity level.
Conclusion
Designating the PRAM area was initially a strategy that was designed to face the issues encountered regarding the length of stay for Pediatric Emergency Department patients and decision for plan and management for Level 3 and Level 4 patients with inclusion criteria based on CTAS Triage. Surveys on overcrowding in ED departments indicate that large variation in data is related to operational processes, specifically patient volumes and flow through the ED, and conclude that patient volume may be more relevant to overcrowding.4 By redefining the ED structure, the process flow, training the frontline staff and educating them to comply with the PRAM guidelines, we were able to tackle the main issues that led to the resolution of the problems. In addition, the patients with their families verbalized a marked improvement on the patient flow in the PRAM. In the KPIs analysis, we are able to see the enormous improvement that is reflected in our daily KPIs review. This quality management initiative is a work in progress and is expected to encounter more interesting challenges.
Our results were achieved based on the improvements that were generated through several PDSA cycles. Our future goal is to include all patients and families in the PRAM process, by providing them information about our area and our process flow as well as our time frames.
We are positive that this quality improvement project will be able to sustain the process of rapid assessment and management of emergency patients leading to improvement of the flow, length of patient's stay and improve family satisfaction.
Acknowledgments
We would like to acknowledge the PRAM of acute care unit nursing team for their commitment and active participation for the realization of the quality improvement projects' goals and objectives; Rua Sultan, Jecel Tulalian , Roxanne Mangilit, Rea Myla Aguila, Apple Ruth Mallari, Sharon Nedroda.
We would also like to extend our sincerest gratitude and appreciation to the physicians and nursing staff of the Pediatric Emergency Department Acute Care Unit in King Abdullah Specialized Children's Hospital, King Abdulaziz Medical City, Riyadh for their dedication and support.
Footnotes
Declaration of interests Nothing to declare.
Ethical approval Based on guidelines set forth by the Quality Management Committee Charter, this Quality Improvement Project was submitted for review prior to its initiation and successfully passed the criteria. This QI project was instigated with the full support of the Pediatric Emergency Medicine Department of the King Abdullah Specialized Children's Hospital.