Article Text

Abstract
Ischaemic stroke can result in approximately 2 million brain neurones being damaged for each minute that it is left untreated. Various trials and studies such as the National Institute of Neurologic Disorders (NINDS) trial, the European Cooperative Acute Stroke Study (ECASS), ECASS II, and the Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke (ATLANTIS) study have clearly demonstrated the beneficial effects of intravenous tissue plasminogen activator (tPA) for treatment of acute stroke.
Therefore to minimise damage and improve clinical outcome, we need to identify patients who present within 4.5 hours of symptom onset and reduce the time taken to adminster a thrombolytic agent. This time is commonly referred to as the ‘door to needle’ (DTN) time.
Our standard, set by the Clinical Commissioning Group (CCG) is to achieve a median time of scanning and thrombolysis within 55 minutes from the time that the patient enters the hospital. The aim of our QIP was to collect data on what the DTN time was during November 2015, December 2015, and January 2016 and to evaluate how this can be improved after each month.
This Quality Improvement Project in the DTN time in patients for thrombolysis has identified areas in the pathway that leads to delays. One major contributing factor is the time for a doctor to come and assess and administer the thrombolytic agent to the patient. Change was implemented by ensuring that the core medical trainee on call is allocated to respond as a priority to all possible thrombolysis calls. This has resulted in a reduction of mean DTN time, from 74 minutes in November to 43 minutes in January. As well as improving patient outcomes, it is proposed that the implementation of change has benefitted the training experience and development of key skills of the core medical trainees.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Our standard, set by the Clinical Commissioning Group (CCG) is to achieve a median time of scanning and thrombolysis within 55 minutes from the time that the patient enters the hospital. However, we found that as a trust we were not achieving this target and that our time was way below target, being 75 minutes in November. One major issue contributing to this delay was the wait for assessment by a doctor in Accident and Emergency (A&E).
We have therefore as a trust aimed at achieving a mean door to needle (DTN) time of less than 45 minutes. We set this because we felt that a mean time would be a more difficult target to achieve and would therefore provide additional motivation to our stroke team to reach this target.
The aim of our QIP was to reduce our DTN time from 75 minutes in November 2015 to less than 45 minutes by the end of January 2016. We would attempt to achieve this by collecting data on what the DTN time was during November 2015, December 2015, and January 2016 and to evaluate how this can be improved after each month.
Background
Ischaemic stroke can result in approximately 2 million brain neurones being damaged for each minute that it is left untreated.1 Various trials and studies such as the National Institute of Neurologic Disorders (NINDS) trial, the European Cooperative Acute Stroke Study (ECASS), ECASS II, and the Alteplase Thrombolysis for Acute Noninterventional Therapy in Ischemic Stroke (ATLANTIS) study have clearly demonstrated the beneficial effects of intravenous tissue plasminogen activator (tPA) for treatment of acute stroke.2
The landmark National Institute of Neurological Disorders and Stroke rt-PA (NINDS) Trial in 1995 showed that treatment with intravenous t-PA within three hours of the onset of ischemic stroke improved clinical outcome at three months.3
The subsequent 2008 European Cooperative Acute Stroke Study III (ECASS III) further demonstrated a benefit of intravenous alteplase beyond the conventional 3-hour time window established in the NINDS trial, effectively extending the window for alteplase administration to 4.5 hours.4
These studies have been discussed and appraised by the National Institute for Health and Clinical Excellence (NICE) and it has been recommended that treatment with alteplase for acute ischaemic stroke should occur within 4.5 hours of symptom onset.5 Therefore to minimise damage and patient disability post ischaemic stroke and thus improve clinical outcome, we need to identify patients who present within 4.5 hours of symptom onset and reduce the time taken to administer alteplase therapy. This time is commonly referred to as the ‘door to needle’ (DTN) time.
Basildon Hospital is a medium sized district general hospital located in South West Essex. When a patient presents as a stroke they are first seen in the A&E department, where there are one of six stroke specialist nurses on-call, providing thrombolysis assessment and initial rapid brain imaging. During this time they will also contact a doctor in A&E to assess the patient and their suitability for thrombolytic therapy. In 2013, 37% of patients presenting with ischaemic strokes were thrombolysed within three hours with a median time of thrombolysis of 81 minutes. This had improved to 57% of all patients presenting with ischaemic strokes being thrombolysed within three hours in 2014 with a median time of 55 minutes. However, there was a large proportion of patients that were still having delays in being thrombolysed and so reasons for this had to be assessed and changes introduced.
Baseline measurement
We analysed the time that the patient was first alerted to the stroke nurse, the time to Computed Tomography (CT) Head scan, the time of arrival of a doctor to examine the patient and then the time of administration of alteplase. The stroke nurse clinical lead uses all of this information to calculate the overall DTN time and for patients who do not meet our target, we are able to establish causes of delay.
Case notes of all patients thrombolysed during November 2015, 11, were reviewed using the parameters above to assess if they had a DTN time of less than 45 minutes. Of the 11 patients, only 3 (27%) achieved the target time, with the 8 patients beyond this having an average DTN time of 88 minutes (43 minutes beyond our target time).
Design
Our team consisted of the stroke nurse clinical lead, who was able to gain feedback and experience from other stroke nurses on call, a core medical trainee currently on a stroke rotation placement and part of the acute medical take, and a senior stroke consultant. Together we evaluated the reasons for the delay in DTN time by analysing patient notes. Out of the eight patients found to have a DTN time higher than the target, the reason for five were due to a delay in the arrival of a doctor to assess and potentially thrombolyse a patient.
As 62.5% of the delay was due to the delay in the arrival of a doctor to assess the patient, it was discussed amongst the team that the core medical trainee on the medical take should be present at potential thrombolysis calls when fast bleeped by the stroke nurse. This was communicated to the core medical trainees at their weekly teaching session where further discussion was had to establish their views before implementation. Most of the core medical trainees felt this would be a valuable learning experience, although some had concerns about an increased work load on an already busy medical take. It was therefore decided to introduce the core medical trainee immediately to thrombolysis calls.
Strategy
PDSA Cycle 1 (December 2015). From our discussions at the end of November, we had decided to introduce the core medical trainee to respond to thrombolysis calls and to see if this intervention led to an improvement in our DTN time, with an expectation that we would see a reduction. The aim of this cycle was therefore to assess how quickly the core medical trainees were responding to thrombolysis calls and how it affected the DTN time. 15 patients were identified in the December cohort and their notes analysed. The DTN time target of less than 45 minutes was achieved in 46.6% of the patients. This was a 72.5% improvement from November. However, over half the patients analysed in this cohort still had a DTN time that was over 45 minutes. Feedback during a discussion with core medical trainees found that there was confusion about their role and prioritising calls from the stroke nurse. This new role was therefore further clarified through an email by the Royal College of Physicians tutor and all trainees were informed that stroke calls needed to be prioritised.
PDSA Cycle 2 (January 2016). The aim of this cycle was to again assess response to calls by core medical trainees and if the target DTN time was achieved. During this cycle, we expected a further improvement in times after further discussions and messages were sent to core medical trainees about their need to prioritise thrombolysis calls. 6 patients were thrombolysed in January. Although 2 patients still had a DTN time higher than the desired target of 45 minutes, it was not significantly higher as compared with the November and December cohort. The implementation of the core medical trainees to carry the stroke thrombolysis bleep and clarification of their role in attending the bleeps seems to have contributed in achieving an acceptable DTN time of less than 45 minutes. We have also found that by setting this target of a mean DTN time of less than 45 minutes that we also met our CCG target of a median time of less than 55 minutes.
Results
Baseline Door to Needle Time in November 2015 (figure 1).

Chart detailing the DTN times for all patients thrombolysed during the month of November
Out of the 11 patients, only 3 (27%) achieved the target of DTN time less than 45 minutes. We evaluated the reasons for the delay in DTN time by analysing patient notes (figure 2).

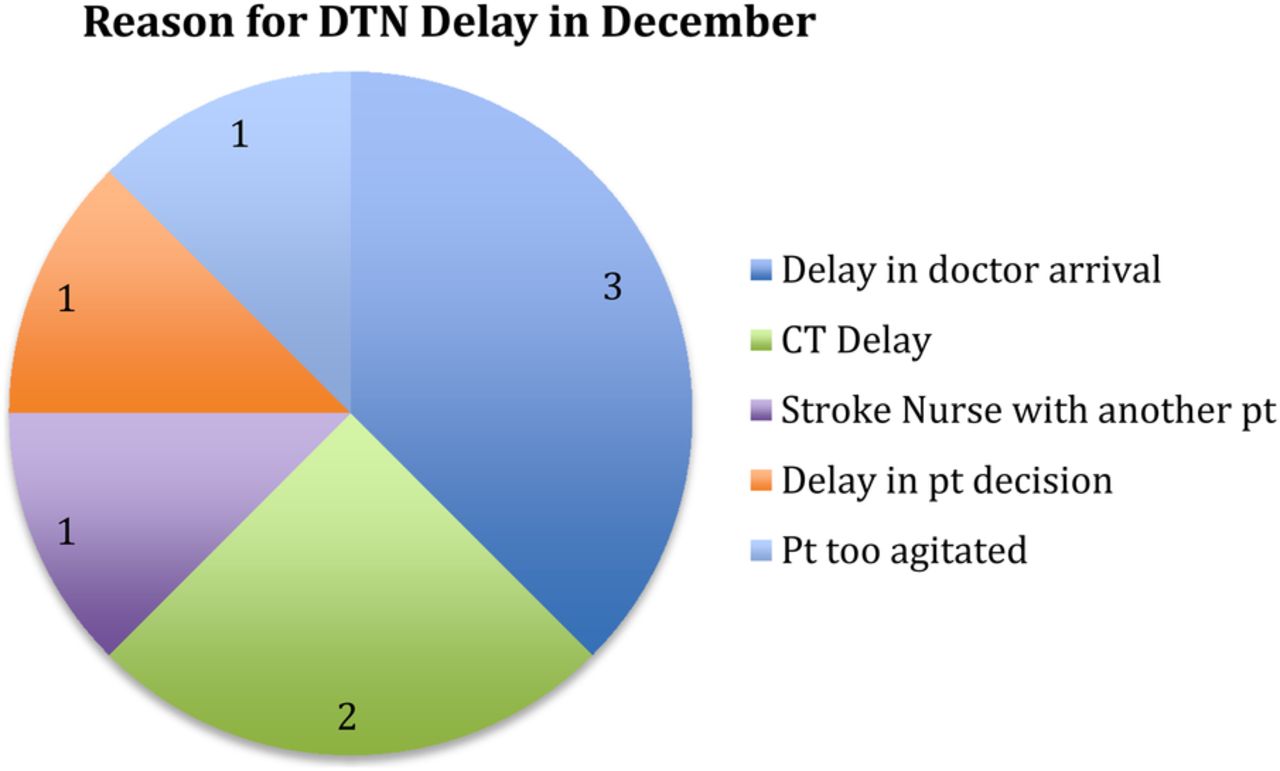
Causes for delay in DTN time in November
Out of the 8 patients found to have a DTN time higher than the target, the reason for 5 (62.5%) were due to a delay in the arrival of a doctor to assess and potentially thrombolyse a patient. It was therefore suggested that the core medical trainee on the medical take should be present at potential thrombolysis calls when fast bleeped by the stroke nurse. Upon this introduction, there was a reduction in the mean DTN time in December 2015. However, the mean time still remained above target of less than 45 minutes (figure 3).

Chart detailing the DTN times for all patients thrombolysed during the month of December after introduction of the core medical trainee
15 patients were identified in the December cohort. The DTN time target of less than 45 minutes was achieved in 46.6% of the patients. This was a 72.5% improvement from November. However, over half the patients analysed in this cohort still had a DTN time that was over 45 minutes. Analysis of the data found that delay in doctor arrival was still a major factor in the delaying of treatment, despite our intervention of making it a priority for core medical trainees to attend stroke thrombolysis calls (figure 4).
Causes for delay in DTN time in December
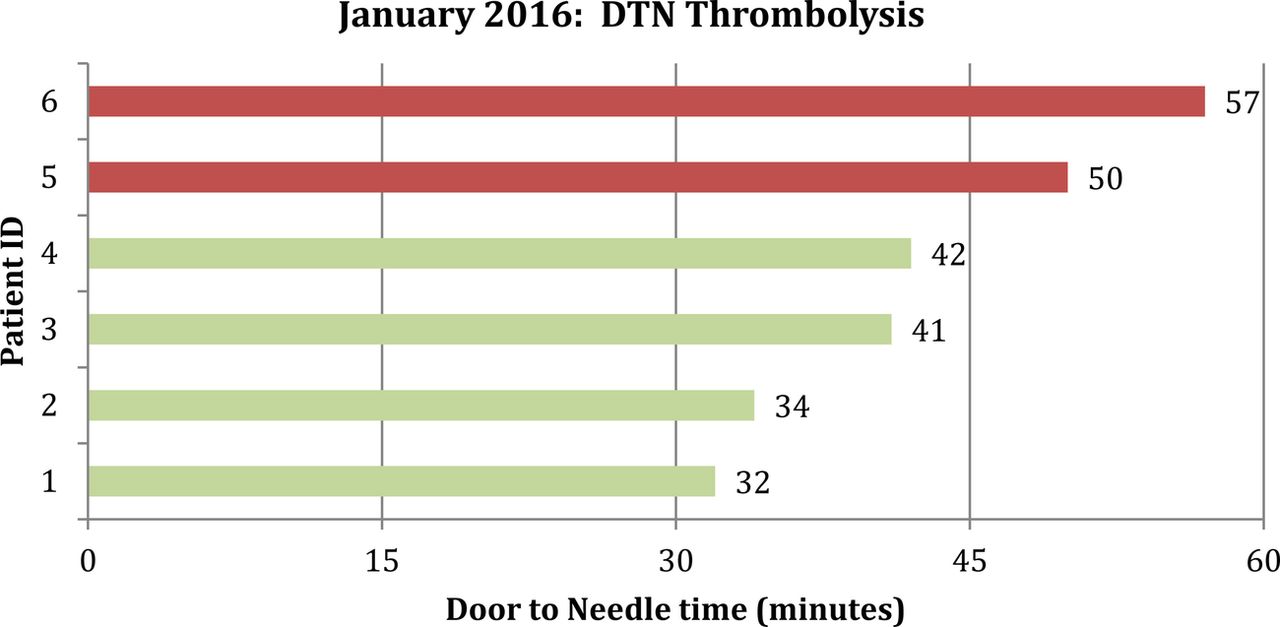
Subsequent feedback during a discussion with core medical trainees found that there was still confusion about their role and the prioritisation of calls from the stroke nurse. This new role was therefore clarified and all trainees were informed that stroke calls needed to be attended as a priority. Data was collected again after this in January 2016 (figure 5).

3. Door to Needle Time in January 2016 After Implementation of Core Medical Trainee to Thrombolysis Calls and clarification of their roles.
There seems to be a vast improvement in DTN time with 66.7% of the patients meeting target. Although 2 patients still had a DTN time higher than the desired target of 45 minutes, it was not significantly higher as compared with the November and December cohort. Analysis of results showed that delay in doctor arrival was not a factor leading to delay during this month (figure 6).

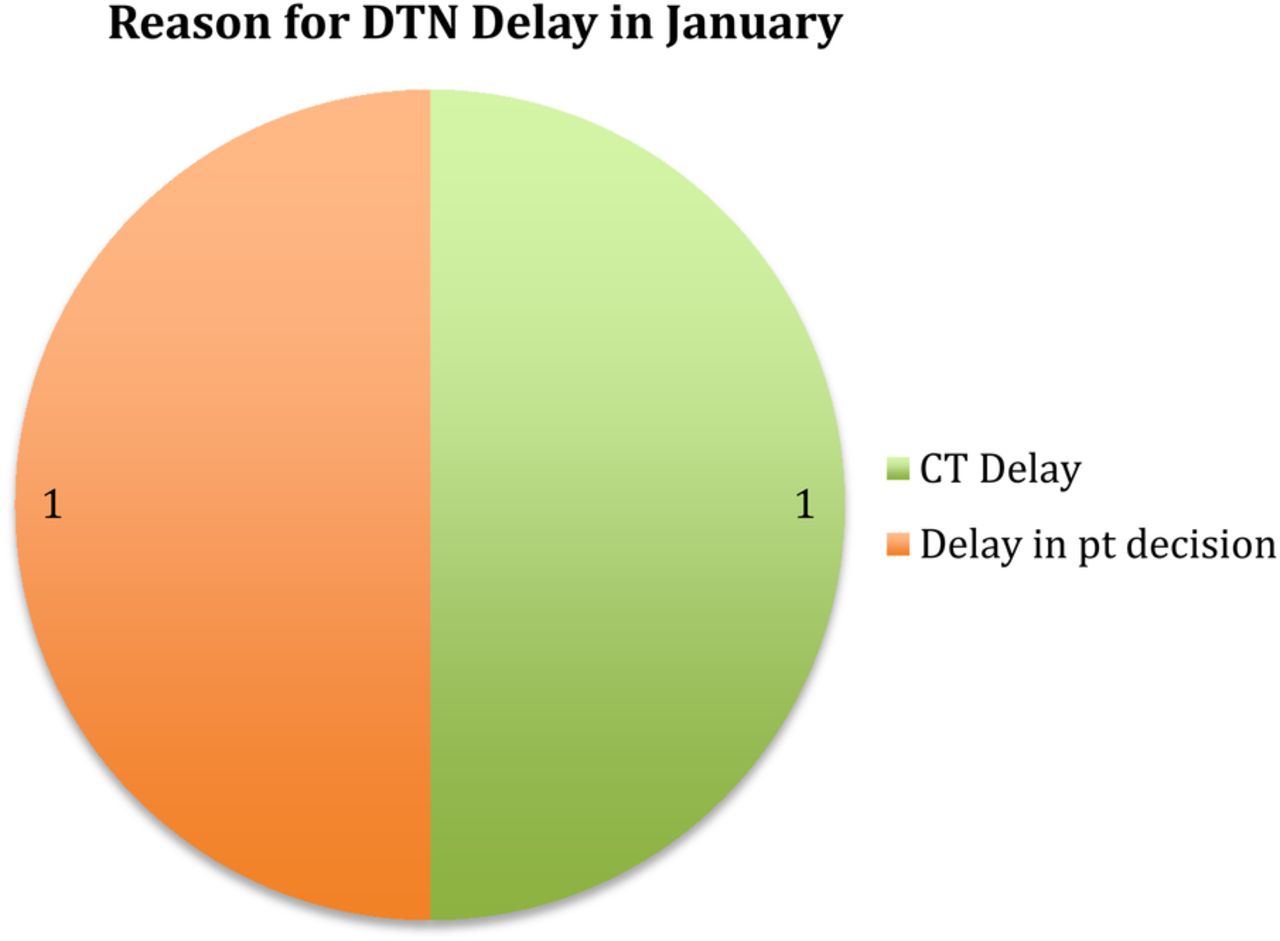
Causes for delay in DTN time in January
The implementation of the core medical trainees to carry the stroke thrombolysis bleep and clarification of their role in attending the bleeps seems to have contributed in achieving an acceptable DTN time of less than 45 minutes by January 2016 (figure 7). We have also found that by setting this target of a mean DTN time of less than 45 minutes that we have also met our CCG target of a median time of less than 55 minutes.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Chart showing mean and median DTN times from November to January after the introduction of core medical trainee
Lessons and limitations
The lessons that we learnt while implementing our project was the need to explain earlier to core medical trainees the reasons why they were needed to attend thrombolysis calls as priority. Initially, there were some that felt that this added to an already heavy workload, however, we were able to demonstrate the benefits of providing stroke cover whilst on call and how it will enhance the training of core medical trainees. If we were to repeat this project, I believe it would have been better to present to the core medical trainees after each cycle our findings for how the DTN time had changed since their introduction. I feel that this would have given further encouragement to them and also increased motivation to achieve even better times.
An important limitation to note is that in December, there was an extreme outlier for DTN time. This patient had a time of 206 minutes, the delay being due to the family needing time to make a decision. Therefore, the mean time would have been significantly affected by this.
Another limitation was that there were only six patients that were thrombolysed in January, giving a much smaller sample size than the previous two months. Although we were able to reduce our DTN time to within our aim of less than 45 minutes, it would be prudent to continue analysing data in future months to come. This would allow us to monitor times further and ensure the sustainability of our project. In the long term, the introduction of the core medical trainee to respond as a priority to stroke thrombolysis calls is likely to lead to improved patient outcomes by reducing the DTN time. We have tried to ensure sustainability of our project by updating all those involved with the stroke thrombolysis pathway of the change we have introduced and how it has improved times. We will continue to monitor the mean and median DTN times as the stroke nurse maintains a record of this and if there are any increases in times, beyond our target of 45 minutes, we will again assess the reasons why, implement change, and inform doctors involved in stroke thrombolysis calls of this.
Conclusion
This Quality Improvement Project in the DTN time in patients for thrombolysis has identified areas in the pathway that leads to delays. One major contributing factor is the time for a doctor to come and assess and administer the thrombolytic agent to the patient.
Change was implemented by ensuring that the core medical trainee on call is allocated to respond as a priority to all possible thrombolysis calls and that they were clear of what was expected of them. This has resulted in a reduction of mean DTN time, from 74 minutes in November to 43 minutes in January. This is in keeping with NICE recommendations of giving alteplase within 4.5 hours and that the earlier it is given, the more patients are likely to benefit from its administration.5
As well as improving patient outcomes, we also propose that the implementation of change will enhance the training experience and development of key skills of the core medical trainees.
Acknowledgments
Beth Smyth
Footnotes
Declaration of interests Nothing to declare.
Ethical approval No ethical approval for this quality improvement project was sought as it was deemed an improvement study and not a study on human subjects.