Article Text

Abstract
Increasing numbers of children are either overweight or obese, which has a significant negative impact on their current quality of life and their future health. The results of England's National Child Measurement Programme 2012-13 revealed that approximately one fifth of 4- to 5-year-olds and one third of children aged 10 to 11 years were overweight or obese. Emergency departments (EDs) see large numbers of children every year and therefore represent a potential opportunity to address the obesity issue.
A pathway was devised to guide referral of overweight or obese children attending the ED to an existing local healthy living programme. Training sessions on the referral process were provided to ED staff. Audits of ED attendance records were undertaken before and after the implementation of the pathway, and the local programme uptake rate for the first 25 referrals was assessed.
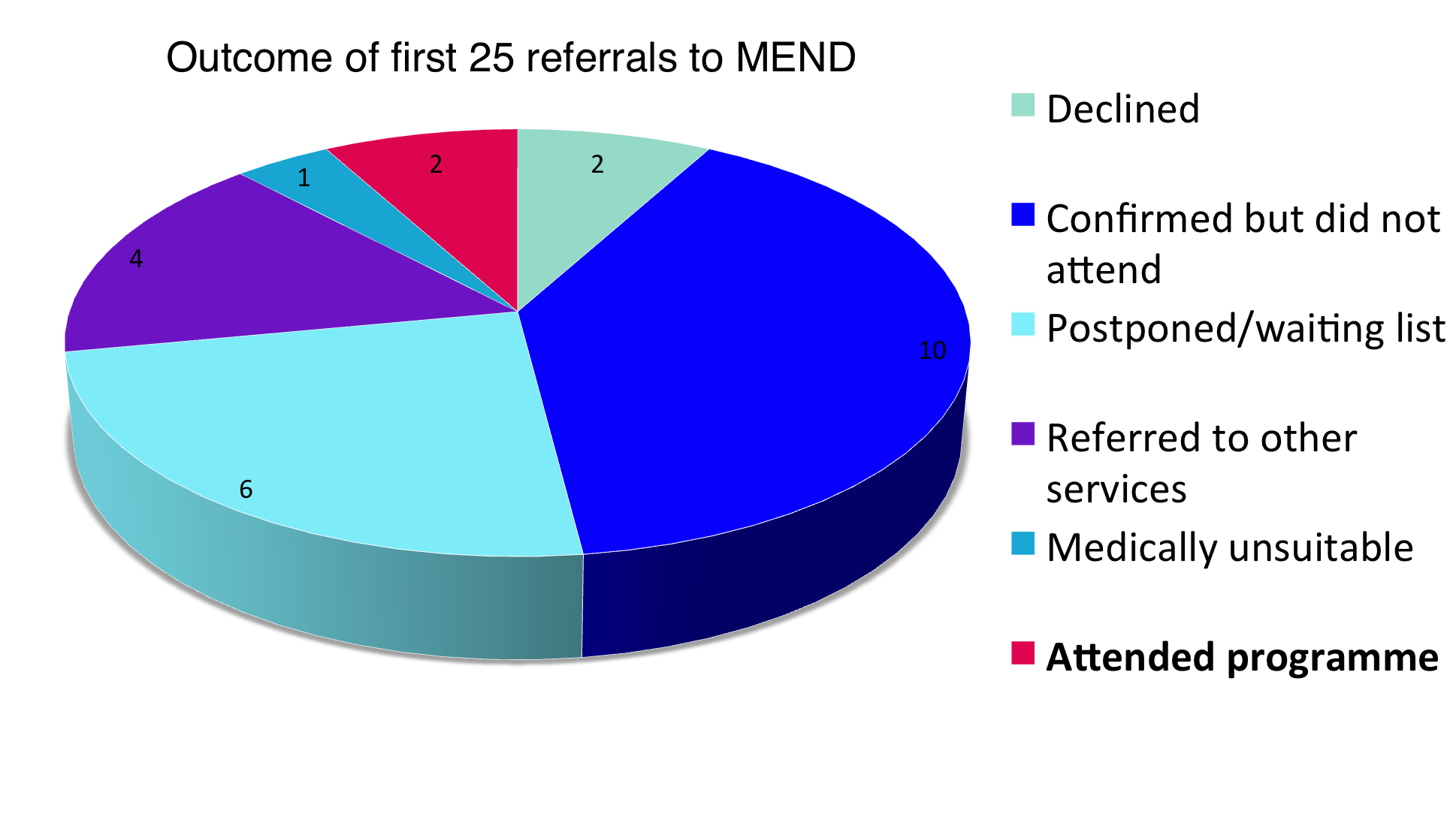
Of the first 25 children referred, two (8%) had participated in a programme, six (24%) were on a waiting list, and four (16%) were referred on to services in their local area, giving an overall engagement rate of 48%.
Further work needs to be undertaken to increase referrals; however, addressing childhood obesity by accessing existing local services from the ED remains a valuable endeavour.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Childhood obesity has been identified by the World Health Organization as one of the most important global health problems (1). Obese children are more likely to become obese adults (2), and have increased risk of cardiovascular disease, diabetes, and cancer (3). In England, one third of 10- to 11-year-old children are overweight or obese, and the rate is significantly higher in certain parts of the country, including London (4). It was noted by emergency department (ED) staff working in a central London teaching hospital that a high proportion of children attending the department appeared overweight or obese. Identifying and managing these children has so far been left primarily to parents, school nurses, and general practitioners (GPs); there are no studies assessing the impact of identification and referral of overweight or obese children from the ED, despite the large numbers of children seen in this setting each year.
Background
Rates of overweight and obese children are assessed annually in the National Child Measurement Programme, which records the weight and height of all children in Reception and Year 6 in England and provides robust data on obesity trends. Although there were fewer overweight and obese 4- to 5-year-old children in 2012-13 than in 2006-7, the rate had increased in 10- to 11-year-olds; of these, 33.3% were overweight or obese (4). Despite the publication of policy documents such as "Healthy Lives, Healthy People; a Call to Action on Obesity in England" released in 2011 (5), the "programme to tackle obesity has been largely piecemeal and disappointingly ineffective" according to a recent report by the Academy of Medical Royal Colleges (6).
Notwithstanding the overall difficulty in addressing excess weight in children, certain interventions have shown to be effective in randomised controlled trials. One such programme, which is available in several boroughs in central London, is run by MEND (Mind, Exercise, Nutrition, Do it), a social enterprise providing community healthy living programmmes for adults and children. Over 90% of children attending a programme show a reduction in their body mass index (BMI), with improvements in their cardiovascular fitness and self-esteem (7). Referrals can be made online and are accepted from any source, which makes this an appealing prospect for ED referrals.
Several studies have shown that overweight or obese children and their parents are receptive to obesity guidance during an ED visit (8, 9); however, there appear to be no studies assessing direct interventions or referrals from the ED targeted at overweight children. Our aim was to identify whether the implementation of a referral pathway in the ED of a central London teaching hospital would improve identification and referral rates of obese and overweight children, and whether these children would subsequently engage with a community programme.
Baseline Measurement
National statistics on overweight and obese children are produced by NHS England. The results for our surrounding boroughs show that the percentage of overweight and obese children ranges from 23-44%, depending on the age and borough in question (4). Children attending the ED can be expected at least to represent the local demographic; some studies, in fact, have suggested an increased ED attendance rate associated with overweight or obesity in children (10).
A 48 h case note review was undertaken with 147 consecutive ED attendance records being analysed before the implementation of the pathway. They were reviewed to assess whether any documentation of the child's weight status was made and whether any intervention was planned, such as referring to the health visitor or informing the GP that the child may be overweight or obese. Additionally, the child's weight was plotted on an age and gender specific weight centile chart to identify those children whose weight was above the 98th and 99.6th centiles. This allowed a very crude estimation of obesity, given that height is not routinely recorded in our ED and therefore BMI could not be calculated.
Thirty-four children (23%) weighed more than the 98th centile for their age and gender, and of those 10 (7%) were above the 99.6th centile. In none of the records was any comment made on the child's weight, nor any referral made to the GP or health visitor.
Design
Local GPs were contacted to establish which services were available in their areas for overweight and obese children, and what the referral process entailed. There were various services available in different clinical commissioning groups (CCGs) with no central referral system, which provided a significant barrier to referrals from the ED. After a review of the locally available services, the MEND programme was selected since it ran in the CCGs covering the majority of our catchment area, and the effectiveness of the programme was supported by randomised controlled trials (RCTs) . Additionally, MEND had already established an online tool which made the referral process straightforward. Referral to MEND was mutually beneficial since its funding depended on filling its programmes; consequently MEND representatives were very supportive of the initiative.
A pathway was developed to help facilitate the referral of overweight or obese children between the ages of 2 and 15 years; the age restrictions reflected those imposed by MEND locally. Children presenting to the ED who appeared overweight or obese would have their height measured, in addition to the routine measurement of weight, and their BMI calculated. If they were overweight or obese according to BMI centile charts, the issue of the child's weight would be addressed sensitively with both the child and caregiver, and permission sought for referral to MEND.
It was anticipated that not all staff would engage in the referral process freely, given that the provision of primary care in the ED is contentious. In addition, time constraints in a busy department would prohibit appropriate referrals if the treating doctor felt it would detract from the urgent care of other patients. Teaching sessions were designed to address these issues, and implementation was at the discretion of the treating doctor.
Strategy
After performing the case note review which identified an absence of documentation of children's weight status and no evidence of referral to GPs or health visitors, the pathway was implemented. Teaching sessions were provided on obesity as a general health problem as well as the specifics of implementing the pathway. Despite this, several doctors voiced concerns regarding the additional time this would take in a busy ED. Further time was spent with those individuals on a one-on-one basis to highlight the importance of the intervention to the individual child's health and to guide the clinician through the referral process. The aim was to reduce the time it would take for them to make future referrals and increase the likelihood of their engagement in the programme.
Three months after the pathway was implemented a further 48 h case note review was undertaken which revealed a disappointingly low documentation and referral rate. Of the 103 consecutive ED attendance records reviewed, only two children were identified in the notes as being overweight or obese. Both of these children were referred to MEND. This was only a small percentage of the 15 children presenting with weights above the 98th centile and significantly fewer than the 33 cases predicted using local demographics.
Owing to the rapid turnover of junior doctors in the children's ED, regular training needs to be established and any referral barriers addressed. Further attendance record reviews and referrer surveys should be performed to help improve the success of the pathway.
One strategy to increase referral rates would be to involve nursing staff in the referral process. Due to the time constraints at nursing triage, only the child's weight was measured routinely. If measurement of the child's height could be entered into the triage process, the BMI could form part of the triage assessment and appropriate referrals made to MEND directly from the nursing team. This should increase referral rates and reduce the reliance on doctors for appropriate referrals.
Results
The referral rate of overweight and obese children was low; however, due to the large numbers of children seen in the ED and the high prevalence of obesity in the local population, there were still sufficient absolute numbers to ascertain the validity of the pathway. The first 25 patients referred during the 3 month period were followed up to assess MEND programme uptake rates. Of these, two had participated in a programme, six were on a waiting list, and four were referred on to services in their local area (figure 1). This suggests an engagement rate of 48%, which clearly leaves scope for improvement.
By comparison, in one study only 61% of overweight or obese adults referred to community health living courses by their GP attended the programme (11), highlighting the difficulty in engaging patients across all age groups.
Despite a desire to achieve 100% uptake rates, a pragmatic approach would be to increase the rate of referral rather than attempt to address the underlying complex issues surrounding programme uptake. Changing colleagues' behaviour may well be easier to achieve than changing that of patients or their caregivers.
See supplementary file: ds2473.png - “Outcome of the first 25 patients referred from the ED to the MEND programme.”
Lessons and Limitations
While implementing the project we learnt that there is a high prevalence of obesity within our population, but that we are very poor at recognising and acting upon this. Even after a promising response to the teaching session the ED doctors still referred few children to MEND. It is very likely that this is due to time constraints within a busy department, which is not something we are able to amend. Concerns were also expressed by members of staff that childhood obesity is a public health problem, not something relevant to the ED. Unfortunately, this opinion may prevent the healthcare provider addressing the patient’s biggest long term health issue, instead focusing on the often trivial reason for ED attendance.
We were surprised at the relatively low uptake of what is clearly a very effective service provided free to the child and their family. This is an area that is outside of our control, and further research will be needed to help improve the step from referral to actual enrolment in a programme.
Regular training will be needed at least every 6 months as we have a frequent turnover of ED doctors who need educating on the referral pathway. We would also benefit from timely feedback from MEND about our referral success rate in order to encourage further referrals to be made. Unfortunately, no further feedback on the referrals was available from MEND. To ensure this remains a sustainable intervention for future doctors to implement we will need to include information about MEND and the referral pathway in the ED doctor induction for our department.
Our results are limited by the fact that we only reviewed the notes over a 2-day period both before and after the intervention. This produced sample sizes of 147 patients before the intervention and 103 after, which may not be representative of the performance of the ED as a whole. Some doctors appeared to be more motivated to refer than others, therefore the sample period may have reflected the working practices of only a small number of doctors and not of the majority.
Similarly only the first 25 patients referred were followed-up. It would be preferable to continue to review this process to establish subsequent uptake rates, and identify components of the referral process that resulted in greater attendance on a programme.
The sustainability of the project will be determined in part by its own success. MEND is commissioned to provide services to the local population and needs to ensure all the places on their programmes are filled. More referrals means higher attendance rates which in turn increases the likelihood of MEND being recommissioned.
Conclusion
Childhood obesity is a growing problem both nationally and internationally. Current interventions are limited in their application and success, in part by the ever increasing obesogenic environment. Specific interventions are greatly needed and every opportunity to improve the health of the population should be fostered.
Our pathway was instituted with mixed success. Fewer than anticipated patients were referred to MEND, and of those who were referred just under half were engaged in a programme. Despite this, the potential benefits to individual children and the population as a whole should not be dismissed. Further work needs to be undertaken to increase referrals, as addressing childhood obesity by accessing existing local services from the ED remains a valuable endeavour.
References
World Health Organization. Global status report on noncommunicable diseases 2010. Geneva: WHO, 2011. http://www.who.int/nmh/publications/ncd_report2010/en/ (accessed January 2014).
Serdula MK, Ivery D, Coates RJ, et al. Do obese children become obese adults? A review of the literature. Prev Med 1993;22:167-77.
World Cancer Research Fund/American Institute for Cancer Research. Food, nutrition, physical activity, and the prevention of cancer: a global perspective. Washington, DC: AICR, 2007.
National Child Measurement Programme: England, 2012/13 school year. http://www.hscic.gov.uk/catalogue/PUB13115/nati-chil-meas-prog-eng-2012-2013-rep.pdf (accessed January 2014).
Department of Health. Healthy Lives, Healthy People: a Call to Action on Obesity in England. https://www.gov.uk/government/publications/healthy-lives-healthy-people-a-call-to-action-on-obesity-in-england (accessed January 2014).
Academy of Medical Royal Colleges. Measuring Up. The Medical Profession’s Prescription for the Nation’s Obesity Crisis. http://www.aomrc.org.uk/projects/obesity-steering-group.html (accessed January 2014).
Sacher PM, Kolotourou M, Chadwick PM, et al. Randomized controlled trial of the MEND program: a family-based community intervention for childhood obesity. Obesity 2010;18(suppl 1):S62-8.
Warkentin J, Chan M, Igric A, et al. A needs assessment for obesity-related anticipatory guidance in the paediatric emergency department. Paediatr Child Health 2008;13:769-71.
Vaughn LM, Nabors L, Pelley TJ, et al. Obesity screening in the paediatric emergency department. Pediatr Emerg Care 2012;28:548-52.
Hering E, Pritsker I, Gonchar L, et al. Obesity in children is associated with increased health care use. Clin Pediatr (Phila) 2009;48:812-8.
Jebb SA, Ahern AL, Olson AD, et al. Primary care referral to a commercial provider for weight loss treatment versus standard care: a randomised controlled trial. Lancet 2011;378:1485-92.
Declaration of interests
None of the authors have any interests to declare.
Acknowledgements
John Criddle, Alex Armitage, Erum Jamall.
Supplementary materials
Supplementary Material for Obesity management in a Paediatric Emergency Department
Extra information supplied by the author
Files in this Data Supplement:
{kind=link}