Article Text

Abstract
Background Paediatric surgery is a stressful experience for patients and caregivers. While standardised protocols are the norm, patient-centred approaches are needed to empower patients/caregivers for an optimal perioperative pain experience. To address this gap, we employed a patient-centred approach using design thinking (DT) methodology to develop insights, map processes, identify opportunities and design solutions for individualised empowerment tools.
Methods In consultation with DT experts, a multidisciplinary team of stakeholders (healthcare providers, patients who underwent pectus excavatum/scoliosis surgery and their caregivers), were invited to participate in surveys, interviews and focus groups. The project was conducted in two sequential stages each over 24 weeks—involving 7 families in stage 1 and 16 patients/17 caregivers in stage 2. Each stage consisted of three phases: design research (focus groups with key stakeholders to review and apply collective learnings, map processes, stressors, identify influencing factors and opportunities), concept ideation (benchmarking and co-creation of new solutions) and concept refinement.
Results In stage 1, mapping of stress/anxiety peaks identified target intervention times. We identified positive and negative influencers as well as the need for consistent messaging from the healthcare team in our design research. Current educational tools were benchmarked, parent-child engagement dyads determined and healthcare-based technology-based solutions conceived. The ‘hero’s journey’ concept which has been applied to other illness paradigms for motivation successfully the was adapted to describe surgery as a transformative experience. In stage 2, patient and caregiver expectations, distinct personas and responses to perioperative experience were categorised. Educational tools and an empowerment tool kit based on sensorial, thinking, relaxation and activity themes, tailored to parent/child categories were conceptualised.
Conclusion DT methodology provided novel family centred insights, enabling design of tailored empowerment toolkits to optimise perioperative experience. Adapting the hero’s journey call to adventure may motivate and build resilience among children undergoing surgery.
- paediatrics
- pain
- patient-centred care
- focus groups
- surgery
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic
Perioperative pain management is usually based on standardisation and does not include patient-centred values for an optimised pain experience.
What this study adds
Novel family centred insights into positive and negative pain influencers, opportunities, patient-caregiver categories for individualisation of empowerment practices for children.
How this study might affect research, practice or policy
Study results will enable design of tailored empowerment toolkits for preoperative education/expectation setting and optimised perioperative experience for children/caregivers.
Introduction
The Institute of Medicine’s landmark paper ‘Crossing the Quality Chasm’, maintains that the overarching goal of healthcare is to consistently provide value-based patient care.1 To achieve this goal, innovations should identify and prioritise the viewpoint of the patient as the end-user rather than solely relying on traditional outcome-based improvement methodologies.2 In paediatric medicine, the end-user construct includes the patient and caregiver. To enhance value-based paediatric care, soliciting the experience of child and caregiver for the design of healthcare interventions is essential.1 3 Design thinking (DT) is an innovative, human-centred, creative problem-solving approach aimed at understanding people, rather than processes.4 DT can promote a more empathic understanding of the child-caregiver construct through direct interaction which allows for the framing of meaningful problems and the development of solutions5 for healthcare problems.
One such challenge is providing a satisfactory pain experience after major surgery, which is a daunting experience for both children and their caregivers.6 Suboptimal pain management and anxiety may compromise recovery, with potential long-term consequences.7–9 We focused on surgical correction of pectus excavatum and scoliosis as they are some of the most painful and stress provoking surgical procedures adolescents undergo.9–11 While perioperative protocols are often used in these surgical populations,10 12 satisfaction with pain management remains suboptimal. In our centre, we use standardised pain protocols and preoperative education, but lack of a patient-centred approach prevents empowerment of patients/caregivers.13 In this project, through consultation and collaboration with a specialty group with design expertise (more information described in the ‘Methods’ section), we applied DT methodology to develop insights and co-create concepts for individualised empowerment tools to improve the patient/caregiver perioperative pain experience. One specific DT modality we used is the integrated new product development process (iNPD). iNPD is generally used in manufacturing, and is universally applicable to problem-solving in a wide variety of situations including healthcare and was implemented successfully to tackle healthcare problems at our institution by cardiology,14 bone marrow transplant15 and behavioural medicine16 teams. This inspired us to use iNPD in the perioperative environment to improve the pain experience. The iNPD process17 uses horizontal and interdisciplinary research-focused modelling (identifying the problem from each stakeholders view, researching the problems, identifying opportunities), ideation (generating a wide variety of ideas) and refinement of process or product (conceptualising solutions in an iterative process) to develop technologically feasible and cost-effective solutions that address stakeholder needs.18
Methods
Setting and participants
This DT project was facilitated by the Live Well Collaborative (LWC), a non-profit organisation run by a multidisciplinary team of faculty and students with design expertise from the University of Cincinnati, mirroring previous collaborations with other groups at our tertiary paediatric institution.19,20 LWC team leads engaged healthcare providers (nurses/nurse practitioners/physicians from anaesthesia, pain, pectus/spine surgical teams and behavioural medicine, physical therapy, integrative care and hospital medicine), and partnered with them to identify and invite adolescents and their caregivers who underwent Nuss procedure or spinal fusion (for idiopathic scoliosis) between June 2016 and June 2018, and their caregivers, to participate in this project.
Intervention
The project was conducted in two stages: stage 1 (June–December 2017) followed by stage 2 (August 2018–January 2019), with different goals for each stage. While stage 1 was used to understand and benchmark the perioperative experiences and gain insights, stage 2 was focused on developing concepts for tailored interventions and built on learnings from stage 1. Each stage was divided into three phases, per the LWC process with the following goals: (A) design research—to generate insights from previous learnings for application to the current problem and use stakeholder expertise to map experiences and identify opportunities, (B) concept ideation—benchmarking of current tools, identify individual differences and co-create tailored strategies and (C) concept refinement—co-creation of the final solution system. We will denote stage followed by phase for easy readability (eg, stage 1A is stage 1, phase A).
Stage 1
Stage 1A
Generate insights from previous learnings
LWC reviewed processes and innovations stemming from three past collaborations between
LWC and the cardiology team,14 bone marrow transplant team15 and behavioural medicine.16
Generate insights into perioperative experiences
LWC used an ‘empathy map’21 to organise insights of stakeholders. Healthcare providers members detailed perioperative processes, while patients/caregivers were interviewed regarding experiences of anxiety/pain, use of technology and helpful/unhelpful factors. Sample questions included “What were the major stress points during your stay in the hospital?”, “Looking back, what do you feel helped/prepared you the most through this process?”
Stage 1B
Assess differences in engagement
Interviews were conducted to assess level of engagement of patients/caregivers and differences in educational needs.
Benchmarking of educational tools
Educational tools were benchmarked by the team through focus groups. A non-weighting matrix was used to rate each tool (working the best (1), working ok (0), needing improvement (−1)) on the following criteria: manageable/sustainable, feedback or output, customisable, educational, engagement, non-obtrusive/integrated, connections, parental role, right information at right time and using resources.
Stage 1C
Deliverables were refined and final products elucidated.
Stage 2
Stage 2A
Build on stage 1 learnings
Learnings from stage 1 were reviewed and thematic ways to present the surgical journey to patients/caregivers discussed.
Generate insights into preoperative expectations
Surveys were used to gain insights into patient/caregiver preoperative expectations/goals.
Stage 2B
Parent-patient persona differences
Caregiver personas were developed based on their comfort with helping patients cope with the surgical journey and their own ability to deal with stress. To develop patient personas, patients were asked how much information they wanted about their pending surgery and their motivations.
Empowerment toolkit development
Alternative pain management tools were benchmarked and classified, and ideal times to deploy them during the perioperative process and suitability for different personas was determined.
Stage 2C
Deliverables were refined and final products elucidated.
Study of the intervention
Data from interviews and focus groups were recorded by real-time notetaking by LWC team during each interview session. The LWC team created a process map of the patient’s/caregiver’s journey from the focus group information.22 Additionally, the team created thematic descriptions using empathy maps, to capture the breadth of behaviours/emotions experienced by a user to identify problems and potential gains from improvements to the current system. ‘User journey’ diagrams were created to provide simple visual representation of the process steps from the experiencers’ viewpoint and ideas explored before converging to shared solutions.4
Measures
Gathering data by a neutral third party (LWC team) decreased observer bias and facilitated systematic qualitative analyses. Focus group deliverables were stage and phase specific. The deliverables included identification of patterns, pain factors and key interventions, followed by definition of dyads, personas and toolkit preferences. The co-creation of deliverables by stakeholders was the end point of each stage. These included healthcare technology-based educational tools, personalised pain coping toolkits and motivational presentation of the surgical journey, allowing optimisation of the patient/caregiver experience through empowerment.
Results
Stage 1
Stage 1A
The LWC team conducted two focus groups with 7 families (patient and caregiver dyads) and 11 clinicians.
Insights from previous learnings
Review of LWC previous projects revealed the importance of having a road map for process flow and expectations,14 providing information at the right time and right place,15 and sharing information with patients/families, for optimal engagement.16
Mapping experiences of stress/anxiety
Stress ‘hotspots’ for caregivers/patients were mapped (online supplemental figure 1). For patients, anxiety peaked during presurgery testing, preoperative check-up, admission, epidural removal (pectus) and transition to oral opioids, discharge and several moments during homecare with physical therapy and dressing removal. Caregiver anxiety peaked between first consultation and insurance application, intraoperative period and during postoperative transition to home care at discharge. Main inducers of anxiety were their child’s overall health, uncertainty about perioperative plans and feelings of inadequacy while helping their child cope with pain.
Supplemental material
Factors influencing pain experience
Thematic analyses provided the following key insights: patient experience was heavily influenced by the patient-parent dynamic, and anxiety in parents was mirrored in their children; as parent buy-in to the process increased, so did patient buy-in; families who had prior experience with a family member in severe pain better communicated pain expectations to their child; parents often focus on the surgery itself and are somewhat surprised by the demands of postoperative care; patients and families feel conflicted between going home and staying longer in the hospital following surgery, as returning home feels ‘safe’ but also a loss of means no longer having the constant in-person medical team support. Positive influencers of pain experience included patient preparedness (involvement in preoperative education), articulation (ability to verbalise/qualify pain), motivation (engagement in the process/adherence to requirements) and confidence in clinical staff/caregivers. Negative influencers included lack of engagement, poor adherence to clinical recommendations and negative emotions (depressive or anxious perspective). Caregivers unanimously agreed that the use of electronic apps would improve messaging, guiding patient care at home.
Stage 1B
The LWC conducted two focus group sessions with 15 clinicians and 4 families.
Patient-family engagement dyads
LWC recognised four combinatorial dyads based on patient/caregiver level of engagement and knowledge seeking: both patient and caregiver engaged; both non-engaged, and either patient or caregiver engaged. This indicated need for customised educational tools targeted to level of engagement within the dyads.
Benchmarking of educational tools
Booklets/Folders, website, preoperative class, poster and clinical staff communication were identified as existing educational resources. A matrix summarising strengths (1=very strong, .5=moderate strength) and weaknesses (−1) with equivocal evaluation of each tools showed that preoperative class and website were considered most useful. Recommendations for improvements were categorised into essential changes, things that should and could be modified/incorporated.
Thematic analyses revealed the following essential elements of solutions: resource to target anxiety peaks, provide emotional support and assistance; ability to engage the patient/caregiver as the better engaged a patient is, the more empowered they feel; create defined roles for the caregiver (as comforter, coach and caregiver) at each stage of the process—this increases confidence in them to aid in the recovery; provide relevant information at the appropriate time, from a trusted source and in a digestible manner; establish connectedness between healthcare providers and families with further strengthening throughout every stage of the process was deemed essential. Education about non-pharmacological alternatives (holistic modalities) and mind-body connection in the perception of pain were identified as essential but missing items in the educational toolkit. Stakeholders selected medication apps, commercially available technology assisted progress trackers, online ‘chats’ with former patients/caregivers, checklists and journal articles as preoperative educational tools with high potential.
Stage 1C
The following frameworks for dissemination of information and for patient/caregiver motivation were co-designed by stakeholders with LWC.
Ambition, information and motivation system framework
The ambition, information and motivation (AIM) system was envisioned as electronic devices (website, mobile app and wearable) communicating with each other and pocket guide relaying information consistent with other tools, to allow consistent real-time messaging in a user-friendly fashion.
The hero’s/heroine’s journey
Realising that illness and surgery pose an important challenge, the hero’s journey seemed the most appropriate structure to transform that experience into a meaningful experience. The hero myth is a template for human growth and development to describe how people deal with illness and life crises.23 It has been applied successfully to other models of healthcare crisis, such as haemodialysis recipients with end-stage renal disease.23–25 ‘The hero’s journey’ promoted by Joseph Campbell26 was selected as the template to highlight the perioperative journey as a transformative process (figure 1A) and the concept had instant appeal with patients/caregivers. The 12 stages of this journey described by Vogler were adapted to embody this transformation for pectus and spine surgical patients using customised storyboarding adapted for age and narrated from patient perspectives. This vision had instant appeal with children and caregivers. Storyboarding of the hero’s journey begins with life before surgery, with individuals living in ordinary world (figure 1A). The ‘call to adventure’ takes place during their consultation with surgical team for possible intervention. The patient and their family may doubt their decision, particularly as they wait for insurance approval—the hero’s ‘refusal of the call to adventure’. However, through interaction with the AIM system, the ‘mentor’ for their journey, our patients can successfully face the obstacles of pain, physical therapy, motivation, time resources and medications. In the end, they find their ‘treasure’—a successful recovery from surgery. They return to the ordinary world stronger and with increased self-confidence.

The hero’s journey illustrates the different stages in the surgical journey as a transformative experience leading to improved resilience and confidence—giving the families tools to face tough situations (A). We storyboarded the journeys of patients who underwent pectus excavatum (B) and scoliosis surgery (C) from a Generation Z-based perspective. AIM, ambition, information and motivation; PT, Physical therapy; PE, Pectus excavatum.
Stage 2
Stage 2A
The LWC team conducted a survey with 17 caregivers and 16 patients.
Thematic choice for hero’s journey illustration
Building on concepts developed during stage 1, illustration styles for the hero’s journey were presented by LWC to patients/caregivers who rated the jungle theme the highest (18/33) followed by space (11/33) and mountain (4/33) themes.
Insights into preoperative expectations
Caregivers’ surgical expectations were for their children to lead a ‘healthier life’ (12/17), ‘recover’ (4/17) and ‘have no complications’ (1/17). Patients expressed surgical goals to be ‘improved physical ability’ (7/16), ‘breathe better’ (6/16) and ‘better looks’ (3/16).
Stage 2B
Caregiver and patient personas
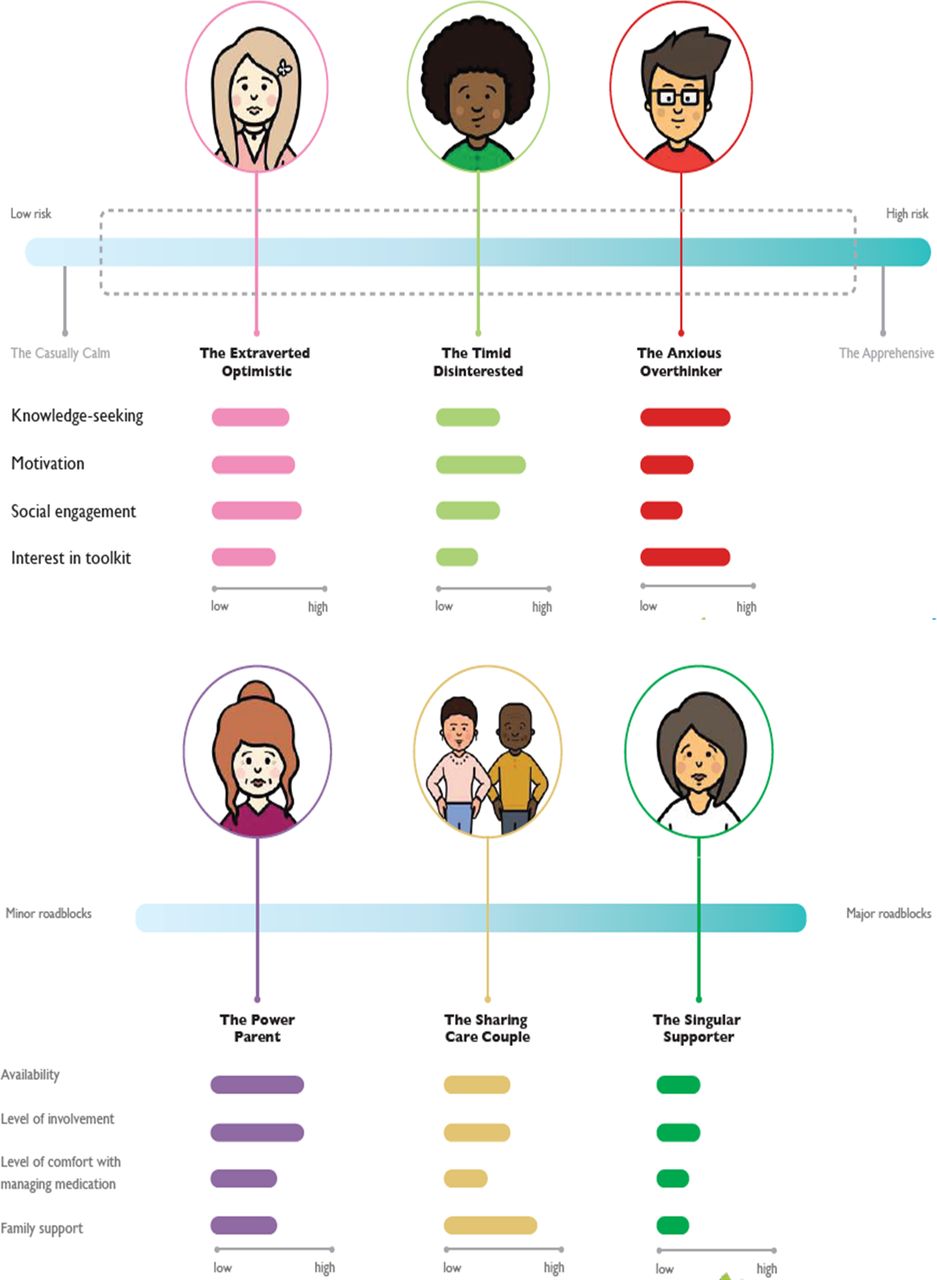
Caregivers (10 mothers/7 fathers) and patients (13 males, 3 females) attended interviews with the LWC team. LWC identified parent personas based on level of availability, involvement and comfort with managing medication (figure 2): (a) the Power Parent is available, able to easily manage complex medication schedules and motivated by their child’s progress; (b) the Sharing Couple: this couple splits caregiving tasks equally due to competing career priorities, but maintaining strict medication schedules is challenging and (c) the Singular Supporter: as the sole supporter, juggling caregiving and working, maintaining a strict medication schedule and managing the complexity of surgery recovery is challenging and stressful.
{kind=link}
{kind=link}
Patient-caregiver personas. Patient personas are presented in the top panel and those for caregivers in the lower panel. The shaded blue line indicates increasing risk for anxiety among the patients (top panel) and increasing level of roadblocks or difficulties in managing their child’s pain (lower panel, for caregivers). The themes used for determining the personas are represented on the left side with each theme scored as low to high by the coloured bars. The terminology does not intend to be judgemental about patients or caregivers but are used as descriptors based on experience shared.
Patient personas defined based on knowledge-seeking, motivation and social engagement behaviours (figure 2) were (a) the Timid Disinterested is non-chalant, calm and generally interested in detailed information. Although they might get anxious, they rarely communicate this distress; (b) the Expressive Optimist is expressive and positive; however, can become increasingly anxious as the surgery date approaches. They enjoy connecting with former patients and asking the doctors questions and (c) the Anxious Overthinker often does extensive research on the topic and often ask ‘what if…’ questions focused on anticipated risks and problems.
Pain empowerment toolkit
Pain management tools were classified as (a) thinking: goal setting, problem solving, setting expectations; (b) relaxation: muscle relaxation, breathing, guided imagery, meditation, music; (c) sensorial: craniosensorial therapy, aromatherapy, massage, healing touch/reiki and (d) activity: exercise, distraction, pacing, scheduling. Thinking and relaxation tools were determined to be most useful during the preoperative stage; thinking, relaxation and sensorial tools during the inpatient surgical stay, while all four tools were considered useful for postdischarge home care.
Stage 2C
Video illustration of hero’s journey
An animated video illustrating the hero’s journey narrative was co-created by LWC team with input from patients (figure 1B and C).
Tailored empowerment toolkit
The tailored toolkit in the form of empowerment cards were developed to be introduced early in the preoperative process, then demonstrated during presurgical class so that patients/caregivers can select and customise the kit to their individual needs.
Discussion
Novel application of DT methodology to understand stakeholders’ views, identify opportunities for improvement and create meaningful individualised solutions for optimizing the perioperative experience of pediatric patients undergoing major surgery. The global aim was to empower patients and families and to improve their perioperative experiences. Using informative data visualisation, stress ‘hotspots’ and factors influencing perioperative stress were identified. Patient/Caregiver dyads and key patient and caregiver personas based on engagement and several other characteristics were defined. These pieces led to frameworks for individualised education and information dissemination using a technology-based AIM system. Empowerment tool kits based on thinking, relaxation, sensorial and activity categories were co-created by stakeholders and the LWC team. Campbell’s ‘hero’s journey’ was adapted using the popular ‘jungle’ theme, to present the perioperative journey as a motivational experience with the aim of building resilience in patients and families.
Our study described ‘hotspots’ or temporal peaks of anxiety for both caregivers and patients. While studies show preoperative anxiety in children27 and higher caregiver trait anxiety predict negatively biased memories for pain-related fear in children undergoing surgery,28 our study also described postoperative stress points and delineates key intervention times to focus on mitigation efforts.
While family centred qualitative research provides an in-depth perspective of patient/caregiver experience, it is rare in paediatric surgical settings. One study in surgical children conducted semi-focused interviews with parents/children and reported that parents stressed the importance of clear communication and preoperative education from the clinical team.29 In our study, we also recognised four distinctly different caregiver-child dynamics that influence educational needs. Although dyadic analyses have been used to elucidate interpersonal influences on pain communication between caregivers and children, they have not been described in a paediatric surgical setting.30 Furthermore, to our knowledge, there are no studies describing patient and caregiver persona. Identification of different caregiver-patient personas emphasises that a one-size-fits-all approach will not be effective and individualised solutions are needed both for education and pain management.
Recent evidence shows that patient-centred approaches positively impact clinical outcomes and more efficient healthcare system utilisation.31 Our findings emphasise onpersonalised medicine concepts and patient-centred care.14–16 With the desire to improve patient/caregiver comfort with medication management, our team implemented an app to provide caregivers with medication schedules in 2019 to provide automated reminders to administer medications postdischarge. We also introduced a preoperative psychological screen in 2019 within surgical workflow which triggers referral for behavioural counselling to improve pain coping.
Finally, adapting the visionary hero’s journey to the paediatric surgical context is a novel concept which can motivate paediatric perioperative patients to rise to their surgical journey challenge. This could transform the stressful surgical experience into a learning experience with lifelong benefits through resilience development. Empowering the patient/caregiver to use learnings from their surgical experience to overcome future adversities could have a long-term positive impact.32
Limitations
Due to the small sample size of focus groups, all patient-parent engagement spectra and personas were not captured. There is a risk for memory bias as patients/caregivers shared previous experiences. This cohort included children undergoing pectus/scoliosis surgery; although this could limit the generalisation of the findings to other surgical groups, we believe the learnings will be universally applicable. Furthermore, data were collected in written format during active interviews (information may have been missed or misconstrued), qualitative data analyses were not supported by objective quantitative measures; hence, generational insinuations and biases may have influenced data interpretation.
Conclusions
DT methodology and patient-centred facilitated individualised educational and pain management empowerment tools intended to improve the perioperative experience for patients/caregivers. The findings provide a basis for future prospective interventional studies for individualised empowerment of patients/caregivers undergoing surgery to improve resilience and the perioperative pain/anxiety experience.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by our institutional review board as a quality improvement project with waiver of consent from participating subjects.
Acknowledgments
The authors sincerely thank Camille Woods for her managerial assistance in facilitating interactions, meetings and presentations by the LWC team and the institutional research team. The authors also thank A Rednour, A de Icaza, K Spang who were graduate students at College of Design, Architecture, Art and Planning, and participated in the research under the guidance of Craig Vogel, Blake Lane and Linda Dunsheath. Additionally, the authors thank Maria Ashton MS, RPH, MBA for providing writing assistance, editing and proofreading. None of the authors have any conflicts of interest to disclose.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @vidyachidambar1
Contributors VC: QI study participation, planning, manuscript preparation, figure editing, interpretation of results. BS: manuscript review, interpretation of results. LB: manuscript review, interpretation of results. RH: manuscript preparation, review. MM: QI study participation, manuscript review. BL: study design, data collection, data interpretation, manuscript review. SW: QI study participation, manuscript review. EMcK, CB, AK: QI study participation, manuscript review. PS, RB: QI study participation, manuscript review. LD: study design, data collection, data interpretation, manuscript review. CV: study design, data collection, data interpretation, manuscript review. VG: study design/planning, interpretation of results, manuscript editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.