Article Text

Abstract
Introduction The Cystic Fibrosis Foundation chronic care guidelines recommend monitoring clinical status of a patient with cystic fibrosis (CF) through quarterly interdisciplinary visits. At the beginning of the COVID-19 pandemic, the Cystic Fibrosis Learning Network (CFLN) designed and initiated a telehealth (TH) innovation lab (TH ILab) to support transition from the classic CF care model of quarterly in-person office visits to a care model that included TH.
Aim The specific aims of the TH ILab were to increase the percentage of virtual visits with interdisciplinary care (IDC) from 60% to 85% and increase the percentage of virtual visits in which patients and families participated in shared agenda setting (AS) from 52% to 85% by 31 December 2020.
Methods The model for improvement methodology was used to determine the ILab aims, theory, interventions and measures. In the testing phase of the ILab, data related to process and outcome measures as well as learnings from plan–do–study–act cycles were collected, analysed and shared weekly with the TH ILab teams. Participating centres created processes for IDC and AS for TH visits and developed and shared quality improvement tools specific to their local context with other centres during the ILab weekly meetings and via a secure CFLN-maintained platform.
Results Both specific aims were achieved ahead of the expected target date. By August 2020, 85% of the TH ILab visits provided IDC and 92% of patients were seen for CF care by teams from the TH ILab that participated in AS.
Conclusion Shared learning through a collaborative, data-driven process in the CFLN TH ILab rapidly led to standardised TH IDC and AS, which achieved reliable and sustainable processes which could be reproduced by other networks.
- COVID-19
- Quality improvement
- Failure Modes and Effects Analysis (FMEA)
- PDSA
- Teamwork
Data availability statement
Data sharing not applicable as no datasets were generated and/or analysed for this study. N/A.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Prior to March 2020 and the COVID-19 pandemic, telehealth (TH) provided an alternative to routine in-person care as a way to increase access to healthcare for patients with chronic conditions, including cystic fibrosis (CF), who reside in remote areas and who have difficulties travelling to their centres.1 2 However, most US CF centres were unfamiliar with incorporating TH or telemedicine techniques into routine CF care. During the COVID-19 pandemic, in an effort to minimise person-to-person transmission of SARS-CoV-2 and spare scarce resources, including personal protective equipment (PPE), routine in-person visits were abruptly halted. This forced CF care centres, like many other outpatient practices, to rapidly embrace virtual visits.3 4
Problem description
Pandemic demanded a change in care delivery from in-person to virtual care. Few CF teams had TH experience. Teams needed to learn together best practices for interdisciplinary, coproduced care in a virtual setting.
The Cystic Fibrosis Learning Network (CFLN), formed well before the COVID-19 pandemic, is comprised of 39 interdisciplinary paediatric and adult CF teams from centres accredited by the Cystic Fibrosis Foundation (CFF). Transition from a paediatric to the adult team usually occurs when the patient is ready for transition and is recommended at the latest when the person with CF turns 21 years. All CFLN teams are multidisciplinary teams that are part of CFF-accredited centres. The team structure differs slightly from centre to centre and generally includes CF physicians, nurse coordinators, respiratory therapists (RT), registered dietitians (RD) and social workers (SW). Some teams also include advance practice practitioners, physical therapists, pharmacists or pharmacy technicians and psychologists. A CFLN centre quality improvement (QI) team may include all interdisciplinary team members or only some team members. In addition, when joining the CFLN, the teams identified, on-boarded and included a patient and family partner (PFP) in their QI team. Pre and post pandemic structure of the CFLN teams was supposed to be identical. Due to furloughs, at the beginning of the pandemic, the team structure shifted, with less team members being available for CF clinics. Based on 2020 registry data, subspecialty (RT, RD, SW) care was provided for 95% of people with CF (PwCF) on annual bases.5 The CFLN teams work together on network-level measures to improve care and outcomes for PwCF and their families through innovative learning structures.6 7 To achieve success, CFLN care centre teams ideally maintain a leadership triad, including a physician leader, QI leader and a PFP. The QI leader is a team member who helps with QI tools, measurement, data collection and data submission. A PFP, is a PwCF or family member of a PwCF who collaborates closely with the CF teams, participates to meetings, helps make decisions and share responsibilities with the team, related to CF centre, QI and leadership activities, locally and/or at the network level. The network leadership team (NLT) guiding CFLN’s priorities includes CF clinicians, adults with CF and parents of children with CF (PFPs).8 The CFLN is in turn supported by staff and faculty based at Cincinnati Children’s Hospital Medical Center.
An innovation lab (ILab) comprises a subgroup of centres interested in learning and innovating in a specific domain. Participating centres are provided the tools and resources to collaborate and create new processes that are then adapted, adopted, shared, tested and refined. The goal of an ILab is to creatively design or redesign systems and/or processes to achieve positive impact through reliable and sustainable processes.
Rationale
The CFLN’s robust infrastructure, experience with agenda setting (AS) and existing ILab learning structure allowed CFLN to pivot quickly to establish the TH ILab early in the COVID-19 pandemic. CFLN teams recognised TH as a priority and gathered together in the TH ILab to create a new CF model of care that would serve families and PwCF, while aiming to maintain a high quality of CF care.
Global aim of TH ILab
Global aim of TH ILab is to deliver coproduced, interdisciplinary CF care that includes TH visits during the COVID-19 pandemic.
Specific aims of TH ILab
Increase the percentage of TH visits with IDC from 60% to 85% by 31 December 2020.
Increase the percentage of TH visits in which patients and families participate in shared AS from 52% to 85% by 31 December 2020.
Methods
Context
In order to minimise person-to-person exposure to COVID-19 at the onset of this pandemic, CF centres were pressured to change from the classical model of CF care to a model of care that included virtual visits. The CFLN’s robust infrastructure, including CFLN teams with extensive QI experience and ILab experience, allowed CFLN to pivot quickly to the TH ILab. We defined TH according to US Health Resources and Services Administration, as using ‘electronic information and telecommunication technologies to support long-distance clinical healthcare, patient and professional health-related education, public health and health administration’. We considered telemedicine a part of TH as defined by the US Centers for Medicare & Medicaid Services, a ‘two-way, real-time interactive communication between the patient and the physician or practitioner at the distant site using interactive telecommunications equipment that includes, at a minimum, audio and video equipment’.9 10 In addition, we define hybrid clinic as visits that occur in person and in clinic and include a virtual component (PwCF interact with the physician in person and some non-physician providers virtually).
Two of the core values of the CFLN teams are to provide interdisciplinary and coproduced, patient-centred care. Interdisciplinary care (IDC) and patient engagement and empowerment have been shown to improve outcomes in CF care. High performing CF programmes have been found to encourage patients to be active participants in their healthcare decision and see themselves as part of their CF care team.11 Interdisciplinary CF care was defined as patient care that included multiple discipline collaboration before, during and after patient visit, as well as with the PwCF or family, to improve patient care. AS was defined as coproduction between the CF team and PwCF and/or families in creating an agenda for the CF visit.
Interventions at TH ILab level
TH ILab work was divided into several phases: pre design, design, launch, active testing and sustainability (figure 1).
During the design phase, NLT members, along with TH experts from University of Virginia and Oregon Health and Science University, served as the design team. Since the NLT is composed of equal numbers of clinicians and PFPs, it was possible to use this existing group to coproduce the design. The model for improvement methodology was used to determine the ILab aims, theory, interventions and measures. The design team developed a high-level process map (figure 2), simplified failure mode effects analysis (sFMEA) (online supplemental appendix 1), aims and a simple key driver diagram (KDD). The specific aims for TH ILab were decided based on prepandemic IDC and AS CFLN data. The goals for the specific aims for the project were informed by registry data related to percentage of PwCF seen by subspecialties prior to the pandemic. During the active testing phase, review of submitted orchestrated plan–do–study–act (PDSA) cycles and tracking of teams with reliability, two separate, robust KDDs regarding IDC and AS were developed based on the initial KDD (figure 3). In addition, during the testing phase, the sFMEA was improved as teams reported unanticipated barriers and their solutions. Finally, the initial PDSA cycles were developed by the design team. However, additional PDSA cycles were developed from the learning gleaned from PDSA cycles submitted by teams. Their testing influenced subsequent orchestrated tests. (For definitions of these QI tools please see online supplemental appendix).
Establish TH ILab coleaders meetings on regular basis.
During the rapid testing phase, TH ILab coleader meetings were held on weekly basis; these meetings were focused on reviewing the data and tools shared by the participating teams, and team huddle preparation.
The TH ILab leadership continued to meet throughout the final stage of the TH ILab with a focus on collection of tips and tools from teams with reliability. Leaders were also involved in the design of a TH ILab change package. Finally, the leaders also developed a strategy for spread of reliable processes to entire CFLN.
Orchestrated PDSA cycles: develop a process for participating teams to share and collaborate in regular meetings/huddles and via a secure CFLN-maintained platform.
Virtual huddle meetings for participant CF care centre teams to share learning and to facilitate the collaborative process were organised on a weekly then biweekly basis. Orchestrated PDSA cycles for the TH ILab community were presented during the huddles to promote shared learning and improvement. CF care centre teams able to execute processes at 80% reliability presented their work in the virtual huddles to benchmark learning. Teams also shared tools created at the local level via huddles and a collaborative platform. Teams shared surveys and processes with one another to learn how to adapt clinic flow and AS processes to meet patient and family needs.
Collect data at the TH ILab level regular basis. REDCap survey data were collected, analysed and shared with the TH ILab teams weekly. The data collected included number of TH visits, percentage of TH visits versus in-person visits and percentage of TH visits that provided IDC and in which the patient and/or family participated in setting the agenda.
Supplemental material
Supplemental material
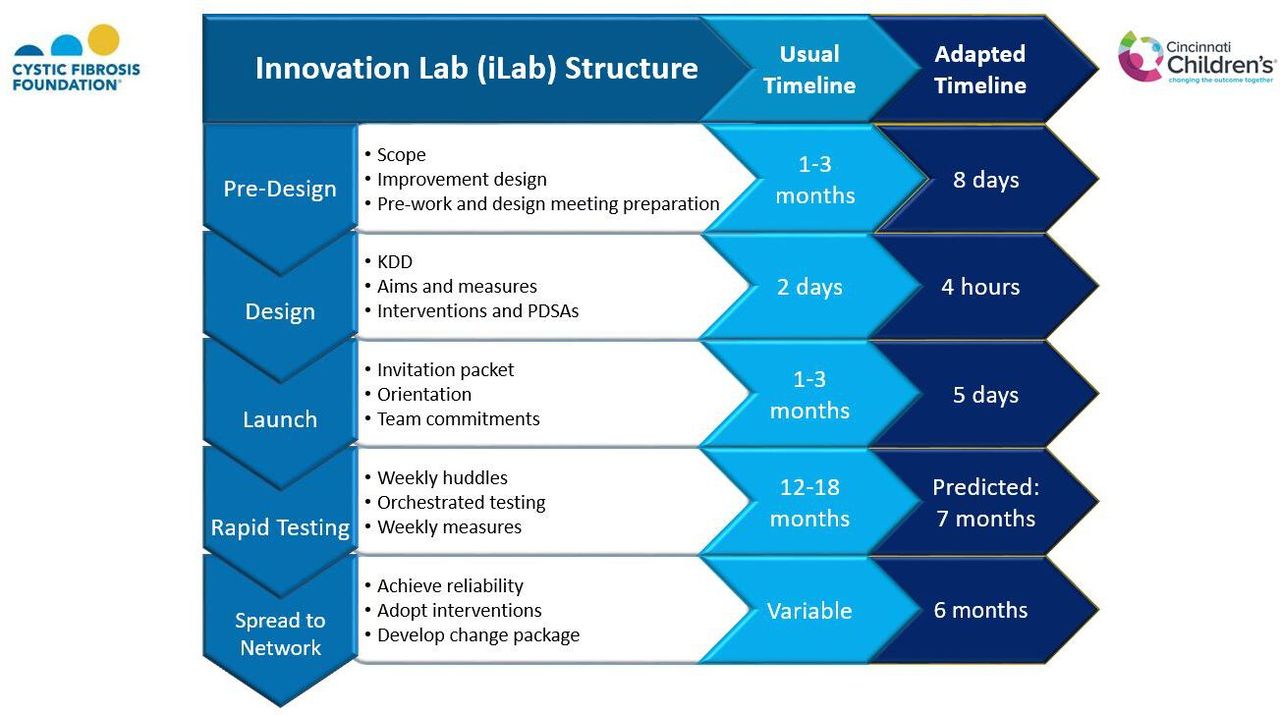
Telehealth innovation lab design. KDD, key driver diagram; PDSAs, plan–do–study–act cycles.
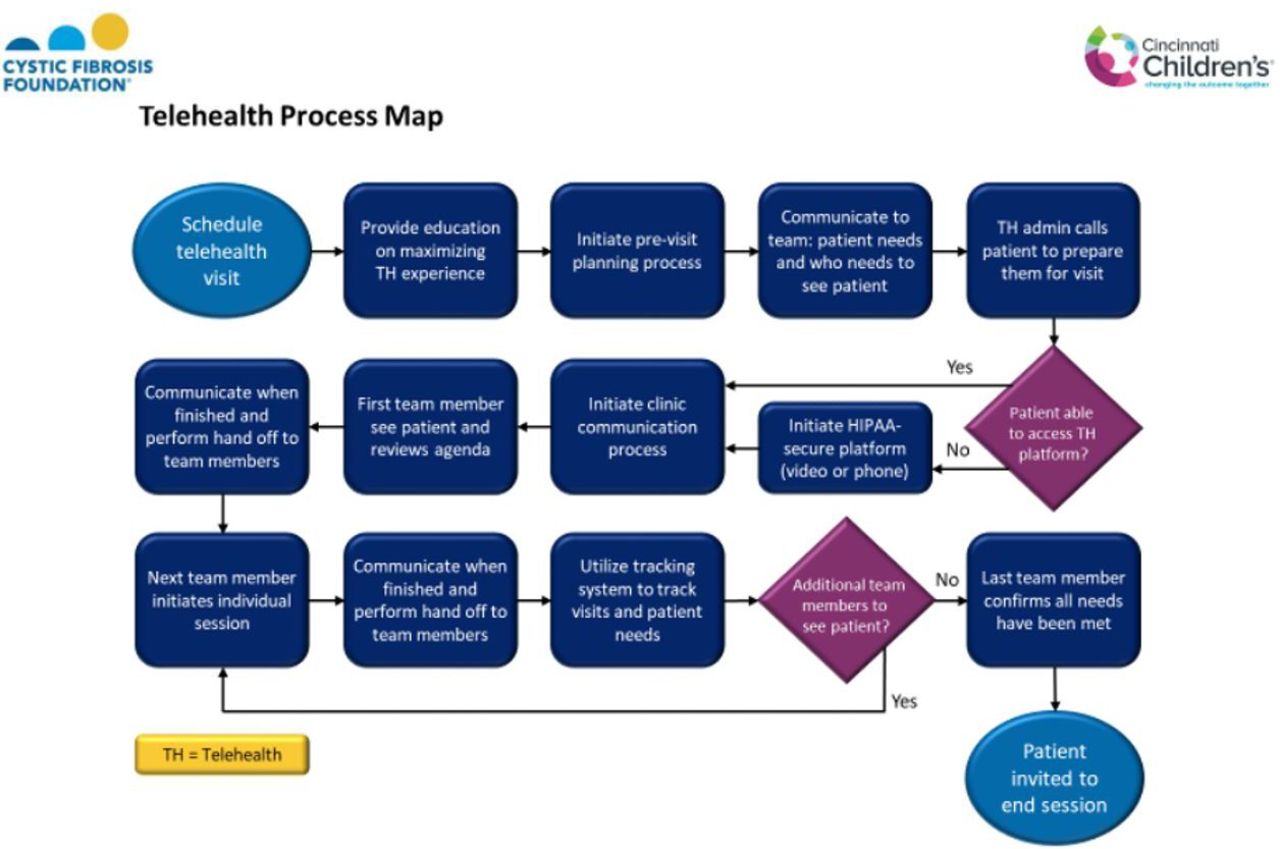
High-level process map for a TH visit, which includes agenda setting and interdisciplinary care. Adapted from TH innovation lab (ILab) package, designed by the TH ILab change package writer group. HIPAA, The Health Insurance Portability and Accountability Act.

(A) Telehealth (TH) innovation lab (ILab) interdisciplinary KDD, cystic fibrosis (CF), CF learning network (CFLN), adapted from Cincinnati Children’s Hospital Medical Center. (B) TH ILab, agenda setting, KDD, CF, CFLN, adapted from Cincinnati Children’s Hospital Medical Center.
Interventions implemented by TH ILab participating teams locally
Create a process to provide IDC through TH
The key drivers and interventions for IDC at the local team level are detailed in the KDD (figure 3A). Each team designed their own PDSA cycles for the following processes: (1) clinic flow for virtual IDC: process with clear steps and role assignments, (2) process for clinical previsit planning (PVP), (3) process for virtual meetings and remote collection of patient history through the Electronic Medical Record (EMR) and CFF patient registry, (4) process to determine and track patient needs as determined by the IDC team, (5) process for virtual meetings with shared tracking documents and (6) process for hybrid visits: adaptation in clinic flow process with steps that incorporate virtual team members into an in-person visit for patients and one to two team members.
Teams also tested a team-driven triage process for TH versus in-person visits (figure 4A). The triage process was based on multiple factors, some of them being related to team local environment, number of COVID-19 cases and healthcare risk for exposure and PPE availability. PDSA cycles related to the triage process at team level were influenced by learning from the other teams in the ILab during the huddles.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cystic Fibrosis Learning Network (CFLN) telehealth innovation laboratory. (A) Interdisciplinary care. (B) Agenda setting.
This testing occurred late in the ILab as team PDSA cycles indicated that many teams were offering in-person visits. Although the ILab did not have access to patient outcomes to determine which patients benefited most from virtual visits, teams did share some alignment in their determination of which patients should be seen in person versus virtually. Alignment among teams for in-person visits included imminent transition to new CF centre; procedure(s) needed onsite; coordination of care with other sub-specialties; recent change in health such as an acute illness or new comorbidity; and severe symptoms for which a hospitalisation might be required. Alignment for virtual visits included increased frequency of visits; alternating quarterly with in-person visits; difficulty with self-management; limited access to transportation; and stable health.
Develop an AS process for the CF TH visits
The key drivers and interventions for AS at team levels are detailed in the KDD (figure 3B). Each team designed their own PDSA cycles for the following processes: (1) process to prepare patients and families for the visit. (2) Process for AS, with clear steps and role assignments with multiple modalities for input from patients and families, for both in-person-hybrid visit and TH visit. The urgent need to adapt processes in the early days of the pandemic helped teams to think about new and redundant processes to increase patient and family participation in AS, including phone, text message, secure portal, day of visit form or face to face (online supplemental appendix 2B). (3) Process for patients feedback and response, to learn with patients and families how to improve and adapt both clinic flow and AS processes. (4) Process to determine and track patient needs as determined by patient and families and ensure that these needs were met during and after the visit. The ILab teams had to learn new ways to meet together and plan for patient needs. These solutions included not only virtual meeting platforms but also shared documents, platforms and EMR communication tools to communicate asynchronously.
Supplemental material
Study of the interventions
Submitted PDSA cycles and measures were monitored for positive shifts as PDSA cycles were conducted.
Main measures
Per cent of TH visits that provided IDC: each TH ILab participating centre provided weekly data on percentage of TH visits with at least one discipline seen by PwCF other than the physician/nursing staff.
Per cent of visits in which the patient and/or family participated in setting the agenda: each TH ILab participating centre provided weekly data on percentage of TH visits in which the CF team and PwCF and/or families collaborated in creating an agenda for the CF visit.
Additional measures
Team engagement was measured by participation to TH ILab team meetings or huddles (number and percentage of CFLN TH ILab teams participating in each meeting), data submission (number and percentage of CFLN TH ILab teams submitting data on weekly bases) and PDSA submission (number and percentage of CFLN TH ILab teams submitting PDSA cycles on weekly bases).
During TH ILab participation, CFLN TH ILab teams also submitted weekly numbers for TH versus in-person visits.
Analysis
Analysis was done by p-chart of IDC and AS.
Results
In the launch phase of the CFLN TH ILab, an invitation package was submitted to the network teams. Teams interested, committed and able to participate to the TH ILab responded to the invitation. Of 39 CFLN care centre teams, 29 (10 adult CF teams and 19 paediatric teams) enrolled in the TH ILab. The 10 teams that did not participate included 7 freestanding paediatric hospitals across the USA. Freestanding children’s hospitals had different institutional supports for TH than academic adult centres or children’s hospitals. The three adult centres that did not participate to the TH ILab have small clinical teams with limited capacity for the intensity of an ILab.
The TH ILab CF centre team meetings or huddles started on 27 April 2020. A total of 22 huddles were held through the end of 2020. The TH ILab coleaders met weekly and 34 coleader meetings were held in 2020. An additional 12 coleader meetings occurred in 2021. The percentage of teams attending TH ILab huddles was 66% on a weekly basis and 72% on a monthly basis; 68% of TH ILab teams submitted data weekly and 79% of the teams submitted data at least once monthly.
A few teams had difficulties engaging in the TH huddles during the duration of the TH ILab being related to (a) changes in institutional policies which encouraged in-person visits and (b) increased incidence of COVID-19 cases leading to decreased team capacity for QI work and/or huddle participation.
TH ILab CF teams submitted an average of 1.4 PDSA cycles per week, with a range of 0–10 PDSA cycles submitted per team per week. The TH ILab teams were highly engaged in testing rapid TH innovations and shared multiple tools developed at their centre according to their local environment. As teams reached reliability and/or moved to in-person clinics, PDSA submissions decreased.
The total number of TH visits reported by teams submitting data from April 2020 to December 2020 was 8223 visits with a monthly average of 914 virtual visits and a range of 486 (October 2020) to 1427 (May 2020).
Interdisciplinary care
Percentage of TH ILab participant CF teams with all disciplines available for patients and /or families reached 95% in July. Percentage of TH ILab teams visits with at least one discipline seen other than physician/nursing staff reached 90% in early August 2020. The TH ILab exceeds its goal of 85% of TH visits with IDC by 31 December 2020 (figure 4A). The main factors identified by TH ILab teams as supporting IDC were: using a robust interdisciplinary communication process, using a platform that supports IDC, ensuring discipline access to virtual platform, having a standardised PVP process and a hand off to next discipline (online supplemental appendix figure 2A).
During huddles, many legal and institutional barriers for all disciplines to access the video-enabled platforms were identified. Some disciplines, such as physical therapy, psychology and dietitians, reported both billing issues and out-of-state licensure issues. Some institutions were not supportive of non-physician provision of care via telemedicine. Therefore, many teams reported that non-physician disciplines provided care via telephone within 1 week before or after the provider telemedicine visit.
Agenda setting
Percentage of TH visits with patient and/or family participation in AS reached 90% in early September 2020. The TH ILab exceeded the goal of 85% of TH visits being conducted with shared AS by 31 December 2020 (figure 4B). The main factors identified by TH ILab teams as supporting AS were: having multiple processes in place for AS (eg, via phone, electronic medical record), having a standardised PVP process and day of visit plan for AS when previsit AS did not occur (online supplemental appendix figure 2B). An example of a PVP questionnaire is provided in online supplemental appendix figure 3.
Supplemental material
Discussion
In a period of 6 months, the CFLN ILab structure allowed 29 centres to coproduce, test and implement TH leading to reliable and sustainable processes. TH was not widely used in the CF community as part of the care model prior to COVID-19. Now it has become a part of a new CF model of care as evidenced by the thousands of virtual visits conducted during the COVID-19 in the CF care network in 2020.10 TH has proven to be a valuable tool to meet the CFF guidelines for quarterly visits for PwCF in the setting of COVID-19 pandemic.3 4 11 12
Previous data have shown that patient communication with AS can optimise patient care and a strong interdisciplinary team involved in routine CF visits can improve patient outcomes.12 13 IDC has historically been a cornerstone for CF care, while AS was an early area of improvement work in the CFLN. It seemed natural to transition this work into the TH ILab aims.
In the CFLN TH ILab, the majority of the participating CF centres were able to reach reliability for IDC and AS. Some of the barriers the CFLN TH ILab teams identified to achieving these results were: staff access to technology and credentialing to use TH as a method of care, staff availability and furloughs and layoffs. In addition, clinical team’s attention to shifting TH requirements created a new work environment and the addition of new technology added challenges.14
PwCF also encountered barriers to care as their team’s availability changed because of aforementioned challenges. In addition, PwCF also have barriers to virtual visits related to access and use of technology, limitations of routine assessments such as lung function and sputum cultures and fatigued related to the use of virtual platforms for so many everyday functions such as work, school and healthcare (see PwCF testimonials in online supplemental appendix).
The TH ILab used the ‘all teach all learn’ improvement strategy and this proved to be successful in supporting teams to overcome barriers for themselves and their patients. It is hard to understand the exact influence of the TH ILab versus the local teams on producing these overall results, given the close collaboration. In addition, given the pandemic and the necessity for TH, balancing measures were not considered in the design of the ILab. The main goal was to provide quality care TH since the teams were forced to provide TH in order to continue to provide CF care. Each CF team participating in the TH ILab adapted and adopted to TH and shared their learning with the TH ILab community. The majority of the teams participating in the TH ILab contributed data, submitted PDSA cycles, presented their work in the weekly huddles and shared their successes in the TH ILab. Data from the TH ILab were shared with the participating teams during huddles and teams were able to see their individual data in a password protected community shared platform. High performing teams’ success was highlighted via network communications and conferences. There was a high willingness of the participating teams to share their results and contribute to the improvement process. With this process the set aims were achieved early and the TH ILab data showed reliability and sustainability. This process could be reproduced by the CFLN in other ILabs and by other learning networks.
A unique aspect of the CFLN TH ILab is the willingness of the participating CF teams with solid QI knowledge and expertise in IDC and AS to collaborate, contribute, adopt and adapt rapidly to TH in context of environmental pressure from the COVID-19 pandemic. In this article, we present the multicentre collaborative work of these high performing CF teams, which recognised early the value in TH care and the importance of IDC and AS, regardless of the CF care platform used and despite environmental and institutional pressures. Other strengths of the TH ILab are: the close collaboration with CFLN PFPs involved in all stages of TH ILab production and the collection, analysis and reporting of data within the TH ILab for process improvement. The PFPs participated in the CFLN meetings regularly and also contributed to the writing of the CFLN change package and of this manuscript.
Despite the success of the CFLN TH ILab, there are many aspects of TH care which were not the emphasis of the work and which need attention for TH to become a major cornerstone of the future model of CF care. First, teams overcame many institutional and credentialing barriers to IDC through workarounds of phone visits rather than video-enabled platforms. These barriers must be overcome for TH to be a sustainable model. In addition, emergency state and federal guidelines for TH reimbursement must be maintained in order to deliver virtual care.
Second, many routine tests, such as spirometer tests, blood draws, sputum culture and physical examinations, cannot be performed during virtual visits. Because the results of these tests are a marker of health status, the lack of these tests can result in less incentive for all stakeholders to participate virtually. A different strategy to obtain CF microbiological cultures would be required for CF TH visits to be successful.15 16 Some teams were very successful in monitoring lung function, forced expiratory volume in one second (FEV1) using home spirometers with TH, while others were not able to monitor FEV1.17
Of paramount concern, barriers involving ease of TH access and increased burden of participation for PwCF and families requires focused efforts and advocacy. As mentioned, early fatigue with virtual platforms combined with technology literacy challenges might have resulted in a degree of avoidance of virtual and tele-appointments on the part of some patients. According to previous surveys, PwCF think that there is a role for TH in the future CF chronic care model.18 Nonetheless, attention needs to be given to identifying what subgroups of patients benefit the most from TH and what subgroups do not. In addition, patient preferences for virtual or in-person visits need to be respected in order for the CF clinic visit to go well.
Further attention also needs to be directed towards equity of care. TH has the potential to increase access to care, as it did during the pandemic. However, it also has the potential to decrease the access for certain subpopulations as shown in other chronic condition.19–22 The CFF State of Care Survey administered at the beginning of the COVID-19 pandemic showed that PwCF from racial/ethnic minorities were less likely to have had a TH visit compared with white PwCF. PwCF and their families who reported financial difficulties found TH more difficult to use and were less likely to think that their concerns or issues that mattered most to them were addressed during TH.23 Beyond the importance of providing equitable care for PwCF from all social, ethnic and racial groups, implementing QI process that address equity is also paramount and should be a future goal of TH.24
The TH ILab IDC and AS processes could spread successfully outside of the TH ILab, to highly proficient QI CF teams with strong QI infrastructure. Due to the pandemic, the process of spread from the CFLN to the entire CF care centre network has been delayed. In the spring of 2022, a focused effort by the CFLN/CFF leadership will be to develop a strategy and communication plan for spread and to develop a measurement system to monitor spread performance. The spread of innovations and improvement in healthcare is challenging.25 Further research and QI work are needed to establish the best strategy for spread between the CFLN teams and the entire CF care centre network.
Conclusion
Employing QI tools in the CFLN TH ILab, to standardise TH IDC and AS, through a collaborative, data-driven process, achieved reliable and sustainable outcomes. The CFLN TH ILab process could be reproduced by other networks interested in implementing TH, IDC and/or AS.
Data availability statement
Data sharing not applicable as no datasets were generated and/or analysed for this study. N/A.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors would like to thank Kathy Sabadosa, MPH, and Dr Bruce Marshall for their continuous support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @LindsSomerville, @pedpulmmike
Correction notice This article has been corrected since it first published. Figure 3 has been updated.
Collaborators Telehealth working group: List of site physician leads, quality improvement leaders and patient and family partners: Cori Daines, MD, Glenda Drake, RRT, Amy Lucero (Banner Children's - Diamond Children's Medical Center, Tucson, Arizona, USA), Lilly Mees, LMSW, Amanda Sharpe (Banner University Medical Center, Tucson, Arizona, USA), Gregory Sawicki, MD MPH, Rachel Gordon, MHA, Lucinda Murphy (Boston Children’s Hospital, Boston, Massachusetts, USA), Ahmet Uluer, DO MPH, Lindsey McMahon, MPH, Melanie Abdelnour, Meghan Murray (Brigham & Women's Hospital, Boston, Massachusetts, USA), Meghana Sathe, MD, Preeti Sharma, MD, Traci Liberto (Children’s Health of Dallas/UTSW Dallas, Texas, USA), Rachel Linnemann, MD, Sydney Schiff, Alexia Hernandez Cargal, Heather Tucker (Children’s Healthcare of Atlanta - Emory University, Atlanta, Georgia, USA), Pornchai Tirakitsoontorn, Maivy Sou, MSN, RN, CPNP, Alicia Maciel (Children's Hospital of Orange County, California, USA), Michael Schechter, MD, MPH, Andrea Molzhon, PhD (Children's Hospital of Richmond at VCU, Richmond, Virginia, USA), Nicholas Antos, MD, Nicole Brueck, APNP, FNP-BC, Karen Wunschel (Children's Hospital of Wisconsin, Wisconsin, USA), Christopher M. Siracusa, MD, Lisa A Mullen, MHSA, Kyle Traver, Travis Burgett (Cincinnati Children’s Hospital Medical Center, Cincinnati, Ohio, USA), Alex Gifford, MD, Nicola Felicetti, RN, MSN, Heidi Dolan, Tracey Gendreau (Dartmouth Hitchcock Medical Center, Dartmouth, Lebanon, New Hampshire, USA), Danielle Beachler, MD, Shine-Ann Pai, BSRC RRT, PFP, Stephanie Robbins (Dell Children's Medical Center of Central Texas, Texas, USA), Ben McCullar, RN, Zoe Orcutt, LCSW, Lindsaey Deveaux (Doernbecher Children’s Hospital, Oregon Health & Science University, Portland, Oregon, USA), Christian Merlo, MD MPH, Lauren Mitchell, PT, DPT, Andrew Scaljon (Johns Hopkins University, Baltimore, Maryland, USA), Rebekah Brown, MD, Stefanie Rushing, RN, Virginia Birnbaum (Monroe Carell Jr. Children's Hospital at Vanderbilt, Nashville, Tennessee, USA), Hossein Sadeghi, MD, Golnar Raissi, MD, Bean Corcoran (Morgan Stanley Children's Hospital, New York, USA), Michelle Prickett, MD, Rachel Nelson, MPH, Joanne Cullina, APRN (Northwestern University, Chicago, Illinois, USA), Fadi Asfour, MD, Anne Snuggerud, RN, Stacy Allen (Primary Children's Cystic Fibrosis Center, Salt Lake City, Utah, USA), Thida Ong, MD, Sabrina Gorry, BS, Lisa Greene (Seattle Children’s Hospital, Seattle, Washington, USA), Peter Michelson, Sara Renschen, Mike Price, Betsy Price (St. Louis Children’s Hospital, St. Louis, Missouri), Catherine Kier, MD, Teresa Carney, NP, Sandy Corr, Barbara Leyva, Jillian Salvatore (Stony Brook Children’s Hospital – Stony Brook University, Stony Brook, New York, USA), George M. Solomon, MD, Julianna Bailey, MS, RD, LD, James Lawlor (University of Alabama at Birmingham, Alabama, USA), Samya Z Nasr, MD, Rebekah Raines, Catherine Enochs, BSN, RN (University of Michigan Health System, Michigan, USA), Jordan Dunitz, MD, Kristen Jesse, RN, Kayla Warner, RN, Jonathan Flath, Mackenzie Wharram (University of Minnesota, Minnesota, USA), Deborah Froh, MD, Holly Carroll-Owens (University of Virginia Children's Hospital, Charlottesville, Virginia, USA), Rhonda List, BS, Lauren Williamson (University of Virginia Health, Charlottesville, Virginia, USA), James Tolle, MD, Susan Eastman, FNP, Marrisa Benchea (Vanderbilt University Medical Center, Nashville, Tennessee, USA), Nauman Chaudary, MD, Mahsa Farsad, MS, RD, Kimberly Wingo (Virginia Commonwealth University, Richmond, Virginia, USA), Kathryn Moffett, MD, Erin Brozik, RN, APRN, and Jillian Huffman (West Virginia University Medicine Children's, Morgantown, West Virginia, USA).
Contributors DA, LT and MP: primary conceptualisation, project administration including methodology, data acquisition and investigation, critical revision for intellectual content and writing and approval of the manuscript. LH and SS: project administration including methodology, data acquisition and investigation and critical revision for intellectual content. LS, PV, EB, MR, MTB, RSA and MS: critical revision for intellectual content and writing and approval of the manuscript. MM, EG and CG: data acquisition and investigation and critical revision for intellectual content. DA is the author acting as guarantor.
Funding This study was funded by Cystic Fibrosis Foundation (SEID19AB0).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.