Article Text

Abstract
Background Carbon monoxide (CO) is an odourless gas produced by the incomplete combustion of carbon containing materials. CO poisoning causes a range of symptoms of which headache is the most common, occurring in up to 90% of patients. An audit in the Emergency Department at University Hospital Aintree, Liverpool, UK found a lack of clinical awareness among healthcare professionals (HCPs) with CO exposure being considered in only 0.8% of patients presenting with non-traumatic headache. This Quality Improvement Project (QIP) aimed to increase this consideration to 50% of presentations.
Methods Three separate sequential Plan Do Study Act (PDSA) cycles were instigated. Interventions involved verbal reminders to frontline HCPs (cycle 1), using strategically placed CO posters (cycle 2) and finally designing and introducing a CO sticker education scheme (cycle 3). These stickers, highlighting the approved CO COMA acronym, were placed in patient notes to serve as a physical reminder for HCPs when seeing patients. Rapid cycle sequencing was used with each cycle lasting 2 weeks. Patient notes were analysed for evidence that the HCP considered a diagnosis of CO.
Results An average of 61 patients were included in each PDSA cycle. Given baseline findings, each cycle demonstrated positive results with CO awareness being considered in 1.7% and 10.0% of patients with non-traumatic headache following cycles 1 and 2, respectively. The final PDSA cycle demonstrated significant increase in consideration of CO to 42.1% of non-traumatic headache presentations.
Conclusion This QIP demonstrated that even small interventions can lead to significant change in awareness of CO exposure. Implementation of a CO sticker education scheme is a feasible way of increasing awareness among emergency care professionals and serves as a low-cost, easy to use, transferable and sustainable solution to address the lack of CO awareness in acute emergency settings. Importantly, this serves to promote improved patient safety.
- PDSA
- Quality improvement
- Emergency department
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Headache is often the most common symptom of carbon monoxide (CO) poisoning which otherwise does not produce a characteristic toxidrome. A high degree of clinical suspicion is thus needed for CO exposure cases to be identified.
What does this study add?
There is a lack of clinical awareness of CO exposure among healthcare professionals. Implementation of a CO sticker education scheme in emergency care is a low-cost, easy to use, transferable and sustainable solution to this clinical problem.
How might this study affect research, practice or policy?
Changes can be implemented to address the lack of CO awareness in emergency care. Further development of non-invasive methods to screen and detect CO exposure within such settings will make diagnosis and management of these cases more accessible in the future.
Background
Carbon monoxide (CO) is a silent killer. Produced by the incomplete combustion of carbon containing fuels, CO is a colourless, odourless and tasteless poisonous gas. Inhalation of CO causes hypoxic injury by displacing oxygen from haemoglobin and myoglobin, compounded by formation of reactive oxygen species. Thus, acute exposure can cause a range of symptoms such as headache, flu-like symptoms or gastrointestinal disturbances. At higher concentrations, it can cause long-term neurocognitive deficits,1–3 seizures, coma and death. Headache is the most common symptom of CO poisoning,4–9 occurring in up to 90% of patients.9
Aside from a patient’s clinical history, CO poisoning is currently most accurately diagnosed via a blood test using the biomarker carboxyhaemoglobin (COHb). However, a low COHb percentage cannot rule out CO exposure as a patient’s COHb level rapidly normalises following removal from the CO source (particularly if supplemental oxygen has been administered before the blood test is taken). In addition, tobacco smoking raises COHb levels and patients may be reluctant to admit to smoking. Nevertheless, a study examining presentations at four large Emergency Departments (EDs) found raised COHb levels in 4.3% of patients presenting with non-specific symptoms.10
The exact prevalence of CO poisoning in the UK is currently unknown. Various studies have attempted to reach an answer, with the Department of Health in 2011 reporting that over 50 people die annually due to CO poisoning in England and Wales with an estimated 200 people requiring hospital admission11, but this is widely accepted to be an underestimation. Overall, they estimate that 4000 people per year are diagnosed with CO poisoning in EDs in England and Wales12; however, this figure does not include those in whom the diagnosis is missed. Studies taking a different approach, focused on identifying sources of CO poisoning by detecting defective gas appliances, found higher than expected levels of appliances deemed to be unsafe.10 13 The All Party Parliamentary Carbon Monoxide Group (APPCOG) has estimated that the consequences of CO poisoning incidents cost the UK taxpayer approximately £178 million every year.14
Limited studies are available on how often CO poisoning is accurately diagnosed in the ED and how often a diagnosis is missed. One study found a survey suggesting the possible probability of missing a diagnosis of CO poisoning to currently be up to 98%.15 Alternatively, anecdotal evidence exists in the form of cases reported in the press where patients who have been unknowingly exposed to CO from domestic sources have been sent home after seeking medical attention for their symptoms and have died from the continued exposure.16 17
CO exposure and subsequent poisoning are thus an important clinical differential that all clinicians should be aware of, particularly among frontline specialists in the National Health Service (NHS). It has long been suspected that medical professionals lack awareness about CO18; toxicology is not routinely taught at undergraduate medical schools and is considered to be a ‘fine print’ subject at postgraduate level. This is compounded by a lack of an easily recognised toxidrome meaning diagnosis is easily overlooked. The APPCOG published three reports between 2009 and 2017 which have included recommendations for efforts to be made to increase awareness of the features of CO poisoning to healthcare professionals (HCPs).19–21
A number of initiatives have been set up including: a large epidemiological study currently running in the south of England to more accurately identify the extent of the problem12 22; public education initiatives by Merseyside and West Midlands Fire and Rescue Services and studies of how CO might spread through domestic dwellings by Liverpool John Moores University. Despite national campaigns such as CO awareness week, a current search of the literature identifies no Quality Improvement Projects (QIPs) or initiatives within local frontline clinical settings.
Consequently, this QIP was conceived. University Hospital Aintree (UHA) in Liverpool, UK, is home to a large, busy ED providing treatment for over 80 000 adult patients yearly and is a major trauma centre serving a population covering Merseyside, North Wales and regions of North West of England. The project targeted all HCPs in the department who clinically assess patients presenting to the frontline. The aim of this project was to increase the consideration of CO exposure in patients presenting with non-traumatic headaches in the ED to 50% of presentations by May 2021. Importantly, this project aimed to ascertain how often ED HCPs consider CO exposure as a differential when assessing patients with non-traumatic headache, not to identify how many patients with headache have been exposed to CO.
Baseline measurement
Baseline research into this issue was carried out at UHA, where presentations of non-traumatic headaches were audited. Given the setting, the decision was taken that analysing cases over the course of a 1-month period would provide the needed sample size to accurately assess the scale of the problem. The aims of this baseline audit were first to ascertain the current consideration of CO exposure and second to gain an accurate idea of the number of non-traumatic headache cases presenting to guide future interventions.
A total of 121 patients with non-traumatic headache were identified. Patient case notes were analysed for evidence that the HCP seeing the patient in the first instance considered a diagnosis of CO. Suitable evidence was deemed to be any mention of CO directly (the terms: ‘carbon monoxide’, ‘CO’ or ‘gas’), or indirect evidence such as questions relating to the COMA acronym.23
The audit found that CO exposure was only considered in one of the 121 patients included, accounting to roughly 0.8% of patients presenting with such symptoms.
Thus, improved awareness was certainly warranted. This would serve to improve both patient care and safety by eliminating the risk of missed clinical cases that can and should be otherwise easily avoidable.
Design and measurement
The QIP team for this project consisted of two junior doctors and an emergency medicine consultant working within the department at UHA. Patient and public involvement was not sought for this project as it aimed to increase awareness for HCPs by introducing system level change. It was crucial to first gain a better understanding of the current processing of patients presenting with headaches to the ED. Thus, the patient journey from initial presentation to assessment was mapped. Understanding both the patient journey and clinical pathway allowed identification of areas for future interventions.
Patients presenting to UHA are coded on admission by an administrative staff member who briefly asks for presenting symptoms and enters them as codes on the ED database. These staff members then print out case notes for each patient that are used throughout their clinical journey within the ED. Following each intervention the ED database was searched using the terms: ‘headache’, ‘migraine’, ‘tension headache’ and ‘cluster headache’. All identified case notes were then analysed for mention of any trauma preceding the headache, and those case notes were then excluded from the project.
Patient case notes were then analysed for evidence that the HCP considered a diagnosis of CO. Suitable evidence was deemed to be any mention of CO directly (the terms: carbon monoxide, CO or gas), or indirect evidence such as questions relating to the COMA acronym.24
The COMA acronym was first proposed by Kar-Purkayastha et al24 and has since been adopted by the Royal College of Emergency Medicine and Public Health England (now UK Health Security Agency) as a useful mnemonic to rule out CO poisoning.23 25 The COMA acronym relates to four simple questions:
C—do any cohabitees have any symptoms?
O—do your symptoms improve when you go outside?
M—do you have any fossil fuel burning appliances maintained by a registered engineer annually?
A—do you have a functioning CO alarm?
Various methods were considered in order to raise awareness of CO as a differential for non-traumatic headaches in the ED setting. Three key strategies were used to increase awareness and education around CO poisoning:
Verbal reminders.
Physical reminders in the form of a poster.
Creation of a tool to act as a reminder for HCPs.
Each intervention followed a rigid Plan Do Study Act (PDSA) cycle, with evaluation occurring after each intervention as part of the study phase. The number of PDSA cycles undertaken was determined by the success of each intervention.
The baseline audit found approximately 121 non-traumatic headache presentations at UHA each month. Thus, a rapid cycle sampling method was used. Each cycle was carried out over a 2-week period to allow for significant patient numbers to assess the impact of the intervention. Following each 2-week intervention, the effects were studied before considering further cycles if the project aim was not reached. A final cycle was expected to be conducted to confirm sustainability of successful interventions.
Strategy
Three PDSA cycles were undertaken, with a final cycle to ensure sustainable change.
PDSA 1: verbal reminders
The first intervention introduced verbal reminders at handover for HCPs. Verbal reminders were scripted to ensure the same level of information was provided to all HCPs and included a brief background on CO and baseline audit findings and the COMA acronym as a useful mnemonic in ruling out CO.
Handover was chosen as most, if not all, HCPs on shift attend handover, which occurs at three points during a 24-hour day: morning handover at 08:00, evening handover at 17:00 and overnight handover at 01:30. The morning and evening handovers were chosen as best times to capture HCPs due to the fact that the night and day team both attend the morning handover, and the day, afternoon and evening team attend the evening handover. Thus, by targeting these times the greatest number of HCPs would be reached at once within the department. Three separate handovers were attended on three separate days in order to ensure a wide audience was reached. It was anticipated that several HCPs who may be on leave, rest days or unable to attend handover owing to various reasons including clinical pressures would be missed. To overcome this, an email was sent out to all HCPs working within the ED outlining the background to the project and encouraging use of the COMA acronym.
It was anticipated that verbal reminders would prompt an increase in awareness of CO however the change would be short-lived and would fail to meet the study aim.
PDSA 2: physical reminders
In this cycle, physical reminders in the ED were introduced through the use of strategically placed posters. The ED consists of a majors department, trauma and resus bay and minors department as main areas of patient contact. Owing to the study only focusing on non-traumatic headaches, the trauma and resus bay was excluded in this intervention. Strategic areas were identified within the majors and minors departments as being areas of focus when clerking patients and areas at eye level for HCPs. Posters placed in the department were produced by the Royal College of Emergency Medicine.25
It was anticipated a further increase through the use of physical reminders would be observed; however, whether this would lead to a significant change in relation to the study aim was unclear. Within a busy ED, HCPs are often stretched due to clinical demands and thus these posters may be easily overlooked in such cases.
PDSA 3: COMA sticker education scheme
The third cycle focused on the use of individualised stickers placed in case notes serving as a physical reminder when seeing patients. Stickers, which included the COMA acronym (figure 1), were designed by the project team. Informal feedback was obtained from HCPs while designing these stickers to ensure they were user-friendly and easy to interact with.
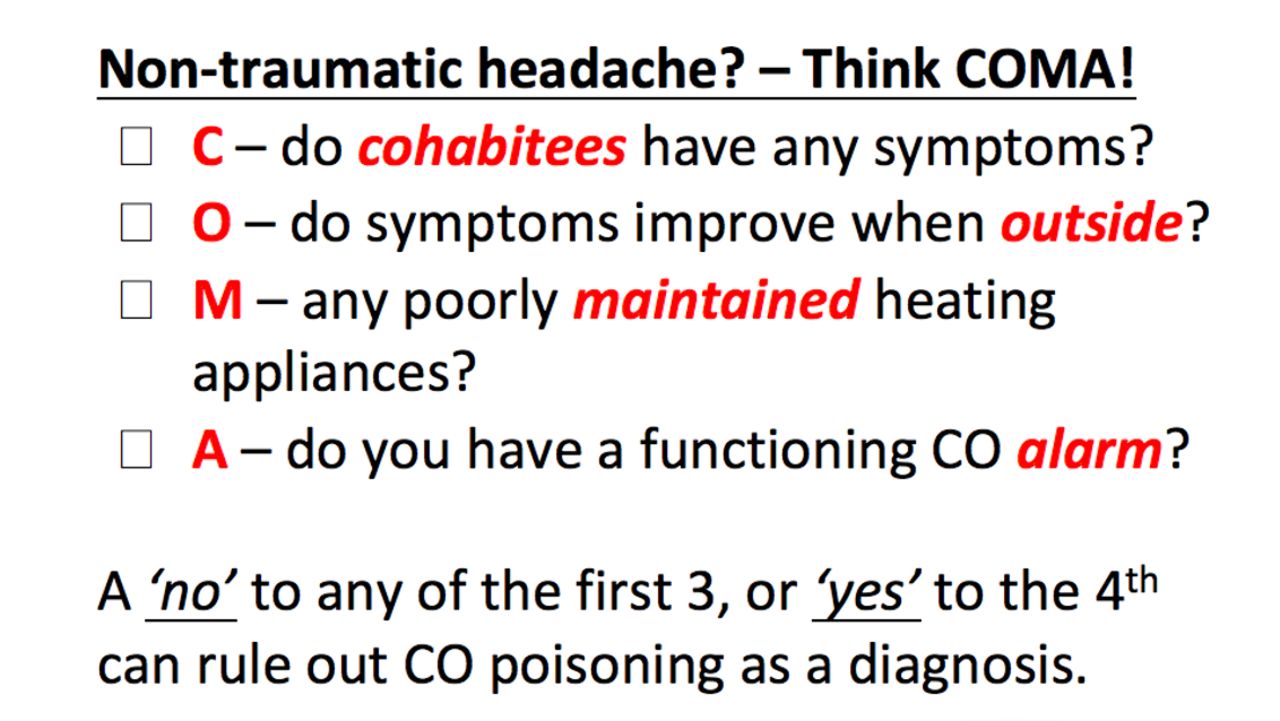
The COMA sticker designed to be used as a physical reminder in patient case notes.
The COMA stickers were printed in mass and provided to the administrative team who admit and print case notes for all patients presenting to the ED. The administrative team were sent an email outlining the project and highlighting the stickers for placement in case notes for patients presenting with non-traumatic headaches.
It was anticipated that the third cycle would lead to a significant change in the department. It would address any discrepancy experienced by using physical reminders (cycle 2) by making the limiting factor the implementation by the administrative team rather than placing the burden on HCPs seeing the reminder.
PDSA 4: sustainability cycle
Following the success of cycle 3, it was theorised that increasing CO consideration could be obtained through the use of COMA stickers and by ensuring they were placed appropriately in patient case notes. Thus, to confirm that it was the COMA stickers leading to results obtained in cycle 3, the cycle was repeated with no added changes for a further 2 weeks.
Results
An average of 61 patients were included in each PDSA cycle of which the median age was 48 years with more women than men presenting. Each PDSA cycle demonstrated positive results with CO awareness being considered in 1.7% and 10.0% of cases following cycles 1 and 2, respectively. Cycle 3 demonstrated that in cases with stickers, CO exposure was considered in 42.1% of cases. Following the positive result in cycle 3, a sustainability cycle 4 was carried out showing CO awareness stayed stable at 41.7% of patients (figure 2).

{kind=link}
{kind=link}
The percentage of HCPs considering CO as a differential for patients presenting with non-traumatic headaches, across our baseline audit and PDSA cycles.
Importantly, the results highlighted continued increasing awareness of CO by HCPs despite turnover of medical staff. In line with training guidelines set out by Health Education England, junior medical staff (Foundation Doctors) rotate three times a year, which occurred once during PDSA cycle 2. Similarly, senior medical staff (those above Foundation level) rotate twice a year, which occurred once during PDSA cycle 1. Despite this, the interventions continued to show a positive increase.
The results also demonstrated that the COMA stickers (used in cycles 3 and 4) led to a significant increase in CO awareness and consideration (table 1). Data for this was obtained as not all patients presenting to ED with non-traumatic headaches had COMA stickers placed in their notes for unknown reasons. On average 24.5% of patient notes had COMA stickers placed in them across the two cycles. Within the cohort where COMA stickers were present in their notes, CO was considered in roughly 41.9% of cases; however if stickers were absent, this fell to an average of 7.2% of cases across the two cycles, in line with earlier PDSA cycles (figure 2).
Comparison of CO consideration by HCPs between patient notes with COMA stickers and those without.
Lessons and limitations
All interventions led to positive results, and increased consideration of CO for patients presenting with non-traumatic headaches. These changes are likely a result of increased awareness of CO as a potential diagnosis among HCPs, which led to a change in attitude when seeing patients.
Of the interventions, introduction of the COMA stickers led to a substantial increase in awareness and as such the sustainability cycle was born. It was theorised that the change seen in cycle 3 was sustainable and indeed could be increased on a longer time scale. This theory was partially true, in that the stickers did lead to a significant increase in CO consideration, however they also highlighted a key limitation of this project—insufficient placement of COMA stickers in case notes. The reasons for this are unknown and warrants further discussion with the administrative team to understand what led to this decreased placement rate and how best to combat it. A second QIP was designed with the explicit aim of increasing placement of COMA stickers by the administrative team, but was hindered by a second limitation.
Recently UHA has moved towards an online platform for storing, recording and interacting with patient case notes. As such, paper case notes are no longer used with all clerking and documentation being undertaken on an online platform. This hindered the use of COMA stickers serving as physical reminders and hindered efforts to introduce a second QIP. However, the potential of introducing a virtual sticker for patient notes to serve as a physical reminder for HCPs is possible. The use of coding in such an instance could remove the variability seen among administrative staff as all patients coded with the term headache could automatically be picked up electronically thus removing human error.
The QIP did not reach its target of having CO considered in 50% of patients presenting with non-traumatic headaches. Timing was a major constricting factor in reaching this target, as the authors felt a sustainability cycle, in the form of cycle 4 would be better served rather than introducing a new intervention.
Conclusion
CO exposure is an important differential to consider in the ED given current national underestimates of patients presenting with CO poisoning owing to difficulty in diagnosis. This was supported by the baseline audit which found only 0.8% of patients presenting with non-traumatic headaches had CO exposure considered as a differential.
While the QIP did not reach its aim, the cycles have highlighted the lack of consideration of CO exposure as a differential for non-traumatic headaches in the ED setting. Yet through educational interventions this can be addressed. Cycles 3 and 4 have shown using a physical COMA sticker can act as a sustainable way of ensuring CO exposure is not missed as a differential. However, further work is still needed to ensure all patient case notes use the COMA sticker scheme and to increase awareness further with educational initiatives required at both undergraduate and postgraduate levels. Additionally, work is required to adapt the physical paper COMA stickers to be used on virtual and online platforms as the NHS shifts into the digital age and paper notes are phased out.
This QIP has shown that even small interventions in the ED can lead to a significant change in consideration of CO exposure as a differential. COMA stickers serve as a low-cost, easy to use and potentially sustainable solution to address the lack of CO awareness in acute emergency settings, thus serving to promote improved patient safety. Having proven such intervention brings positive change; this should be rolled out and evaluated at further local hospitals to replicate findings.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
The authors would like to thank the staff at University Hospital Aintree emergency department for actively engaging with this project. In particular they acknowledge the efforts of Dr T Wharton and Dr C Kelly in getting this project set up and running. The authors would also like to acknowledge the International Carbon Monoxide Research Network and the Carbon Monoxide Research Trust for their support in helping get the results of this project out in the public domain.
References
Footnotes
Contributors FSM and RGA contributed equally to this publication. SC is the consultant lead for the project and undertook the initial phase of the project. Both authors FSM and RGA act as guarantors for this project.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.