Article Text

Abstract
Background Acutely sick or injured patients depend on ambulance and emergency department personnel performing an accurate initial assessment and prioritisation (triage) to effectively identify patients in need of immediate treatment. Triage also ensures that each patient receives fair initial assessment. To improve the patient safety, quality of care, and communication about a patient’s medical condition, we implemented a new triage tool (the South African Triage Scale Norway (SATS-N) in all the ambulance services and emergency departments in one health region in Norway. This article describes the lessons we learnt during this implementation process.
Methods The main framework in this quality improvement (QI) work was the plan–do–study–act cycle. Additional process sources were ‘The Institute for Healthcare Improvement Model for improvement’ and the Norwegian Patient Safety Programme.
Results Based on the QI process as a whole, we defined subjects influencing this work to be successful, such as identifying areas for improvement, establishing multidisciplinary teams, coaching, implementing measurements and securing sustainability. After these subjects were connected to the relevant challenges and desired effects, we described the lessons we learnt during this comprehensive QI process.
Conclusion We learnt the importance of following a structured framework for QI process during the implementation of the SATS-N triage tool. Furthermore, securing anchoring at all levels, from the managements to the medical professionals in direct patient-orientated work, was relevant important. Moreover, establishing multidisciplinary teams with ambulance personnel, emergency department nurses and doctors with various medical specialties provided ownership to the participants. Meanwhile, coaching provided necessary security for the staff directly involved in caring for patients. Keeping the spirit and perseverance high were important factors in completing the implementation. Establishment of the regional network group was found to be important for sustainability and further improvements.
- Healthcare quality improvement
- Emergency department
- Prehospital care
Data availability statement
Data are available upon reasonable request. Data is uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic?
Quality improvement (QI), by introducing new practices in healthcare, is challenging and require certain theory-based skills.
What this study adds?
In addition to managerial support, it is crucial to engage, involve and ensure that the staff are interested in all parts of the process.
Selecting the right data and measurements can be challenging, but it is important to show improvements.
How this study might affect research, practice or policy?
A concrete example of how the use of knowledge about success factors and structured framework in practical QI work can lead to sustainable QI.
Introduction
Improving the quality of healthcare is one of the greatest challenges in modern healthcare leadership. A systematic approach with improvement in professional knowledge is necessary to increase patient safety in such a complex system. Many factors have been identified essential for successful quality improvement (QI): leadership engagement, clear and specific goals, multidisciplinary teams, continuous and reliable information, systems thinking, data collection/measurement and analysis. Other factors such as coaching, engagement and keeping spirits high have also been deemed important.1–4 The plan–do–study–act (PDSA) cycle is an internationally known method of planning for systematic QI work.5
Several methods are used worldwide to assess and prioritise (triage) patients in the chain of emergency care.6–8 Examples are the Manchester Triage Scale, the Australasian Triage Scale, the Canadian Triage and Acuity Scale and the South African Triage Scale (SATS).9–13 Effective triage should rapidly identify patients with life-threatening conditions in need of immediate care and ensure that each patient receives similar initial assessment, facilitating further diagnostic work-up and treatment.
Over a four-year period, a new triage tool was introduced in the ambulance services/emergency medical service (EMS) and emergency departments (EDs) in the Western Norway Regional Health Authority. Its aim was to improve the quality of the initial patient assessment and increasing patient safety. The need for this new system was indicated by several adverse events related to delayed identification and initiation of treatment for patients with, for example, acute myocardial infarction, stroke and severe infections (sepsis).14–16 Furthermore, there was a need to improve communication and mutual understanding about the patient’s medical condition among nurses and doctors in the EDs, and between the ED nurses and EMS personnel.17
A new triage tool should be symptom based, consist of vital sign scoring, be simple to use and have the possibility of modification to suit local needs and conditions.18 19 After thorough consideration from medical professionals, SATS was chosen because of its intuitive structure, content, simplicity and suitability in our requirements for a triage tool.20
The present article describes the lessons we learnt from the implementation process of SATS, as a new emergency medical triage tool, in the Western Health Region in Norway.
Materials and methods
Organisational description and setting
The Western Health Region covers an area of 43 000 km², with approximately 1.1 million inhabitants. The health region includes 7 EDs: 2 are fairly large with approximately 40 000 patient referrals a year and 5 care for 5000–15 000 patients a year. There are four EMSs in the region. During 2018, approximately 50 000 (41%) of the 120 000 patients referred to the EDs were transported to the EDs by ambulance/EMS. The activity of the four EMSs varies from about 16 000 to 57 000 assignments a year, totalling 130 000 emergency transportations a year in the region. In the Norwegian healthcare system, more than 90% of the patients in the ED are referred to the hospital by a primary care physician, and 10% are referred directly by ambulance without a doctor’s referral. Of these, 75%–80% are admitted to hospital wards, whereas 20%–25% are discharged home from the ED.
Description of the triage tool
SATS is a physiology-based and symptom-based triage scale developed by a multidisciplinary group in the Emergency Medicine Society of South Africa. They have allowed Haukeland University Hospital (HUH) to freely modify the SATS to suit Norwegian conditions. The Norwegian name of the triage tool is SATS Norway, abbreviated as SATS-N, and is the new medical triage tool implemented in the region. The SATS-N prioritises patients into five priority levels (PLs): ‘red’, ‘orange’, ‘yellow’, ‘green’ or ‘blue’. PL ‘red’ corresponds to the most serious conditions. The most obvious difference between SATS and SATS-N is that SATS PL ‘blue’ means the patient is deceased, and SATS-N PL ‘blue’ describes milder conditions with no need for measuring vital signs.20 21
The SATS-N triage tool consists of three parts:
A discriminator list with symptoms and conditions, which prioritises the patient to PL red, PL orange or PL yellow. Several discriminators have footnotes that further describe the symptoms/conditions.
Triage Early Warning Score, based on vital parameters and clinical signs.
An option for upgrading the PL based on the individual healthcare provider’s discretion. Only physicians can lower the PL set according to the SATS-N manual.
The individual patient’s PL is set according to the highest PL of these three. The PL indicates the severity of the patient’s medical condition and how soon a medical examination should be performed.21
Theoretical framework and implementation process
The chain of emergency care is a system of many interconnected actors. The quality and safety of care depends on the quality of the parts and their interactions. This is defined as ‘systems thinking’.22 The Ancient Greek philosopher and scientist Aristotle said, ‘The whole is more than the sum of its parts’.
Implementing a common triage system in an entire health region requires a systematic approach in three stages: (1) testing new knowledge-based ideas, (2) implementing changes that are evaluated as successful and (3) making the changes that appear to be successful and sustainable.23 The PDSA cycle was chosen as the main framework for this QI process.5 The Norwegian Patient Safety Programme and the Institute for Healthcare Improvement (IHI) Model for improvement were additional sources.24 25 This theoretical framework was used as a method and support for the implementation throughout the QI process.
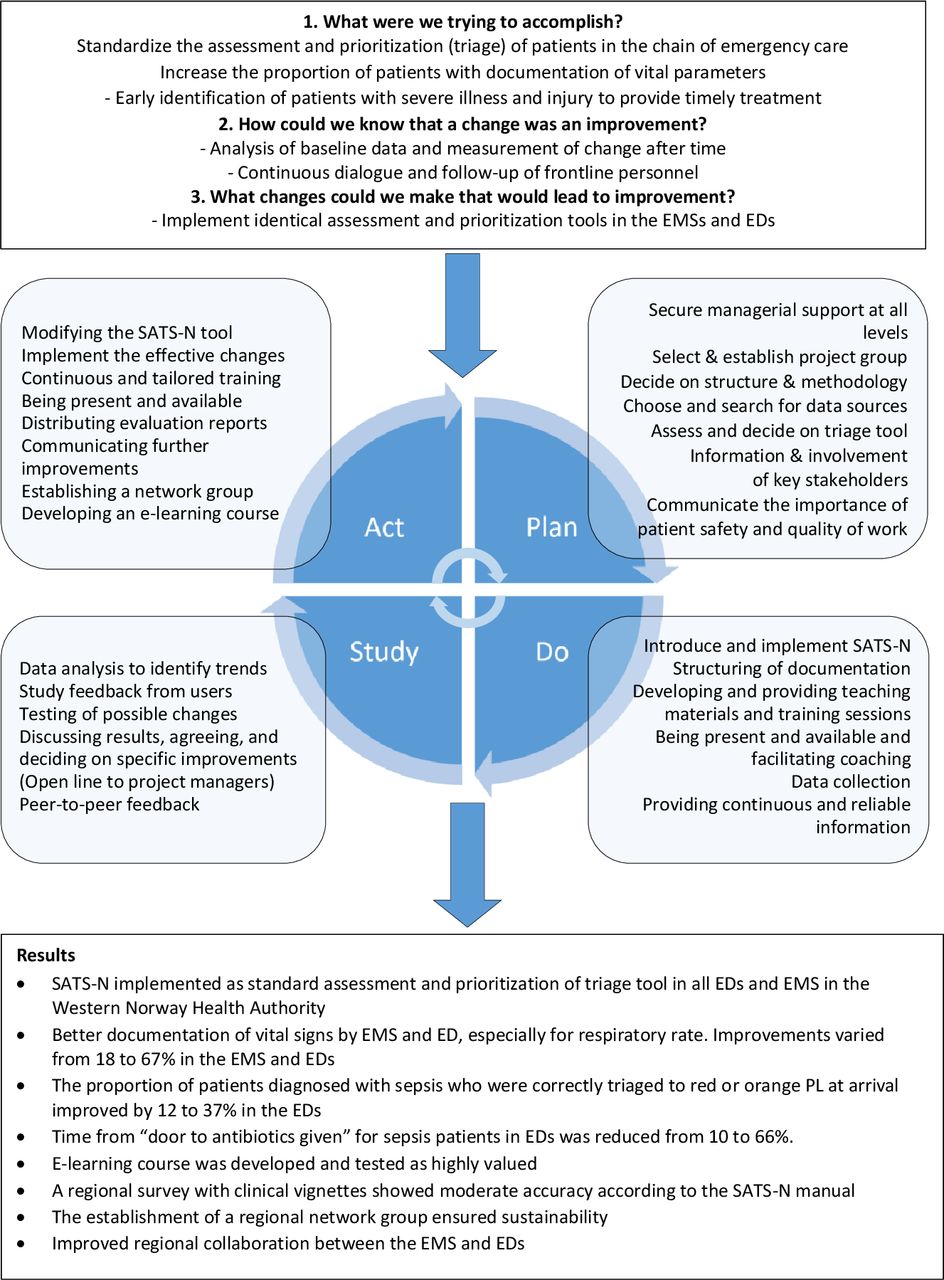
We completed several PDSA improvement cycles, and figure 1 presents a synthesis of the content of this QI work. We planned and tested the triage system, and then collected and analysed data to determine the need for adjustments before the next improvement cycle. In addition, figure 1 provides an overview of some of the results throughout the process.

Overview of the QI. ED, emergency department; EMS, emergency medical service; QI, quality improvement; SATS-N, South African Triage Scale Norway.
Before starting the project, managerial support was obtained by reporting and presenting the case to the hospital’s management team, as well as involving the care staff. This was necessary to start the project and secure the sustainability of changes.
A multiprofessional project group consisting of several healthcare providers, including physicians, ED nurses and ambulance personnel/emergency medical technicians (EMTs), was established. It was important to include people who wanted changes, and were willing to implement them to achieve improvements (the so-called ‘early adopters’ and role models). To spread information, raise visibility and be available, several information meetings with all participating departments were arranged. Early on, physician specialists from relevant hospital departments were involved in modifying the pilot version of SATS-N. They also contributed medical advice, customisation and translation of the discriminators. If there was little interest from any of the project participants, we contacted them, asking for input to make them gain interest in further work.
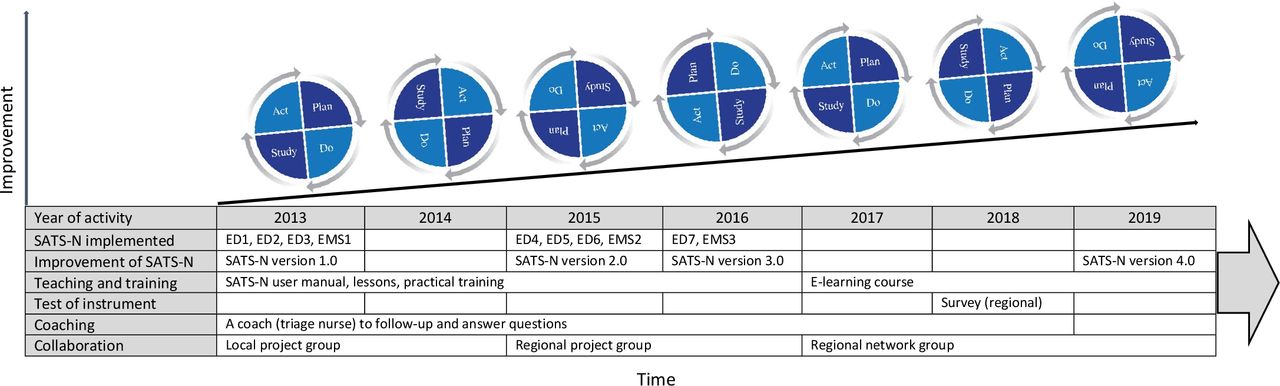
The implementation of SATS-N lasted for several years. Figure 2 shows the main activities in the improvement work from 2013 to 2019.

{kind=link}
{kind=link}
The main activities. ED, emergency department; EMS, emergency medical service; SATS-N, South African Triage Scale Norway.
In 2015, as a part of the National Patient Safety Programme, the Western Norway Regional Health Authority’s executive decided to implement SATS-N in the remaining health trusts. The process was to be led by the HUH, based on the experience from the first round. We used the same method, with minor tweaks and simplifications. For example, we were more specific about the type and amount of data used.
One dedicated triage nurse (the same as in round 1) provided specific coaching, support and training throughout the region and served as a liaison between the main project managers and the teams in each health trust. Each leader involved their own physician specialists, securing local medical support and buy-in from the physician group. In one situation with disagreement, the regional executive medical directors were presented with the case and a mutual decision was made.
The first baseline data were collected in 2012, and the last evaluation data were collected in 2016. Online supplemental appendix 1 shows the time for implementation related to time for baseline data and evaluation measurement. The variables measured were based on what we wanted to improve and what was possible to measure. When the EDs and EMS were included, they had the opportunity to modify variables. However, they measured the same variables. Table 1 presents a selection of measured variables and the improvements achieved in the EDs and EMSs.
Supplemental material
Measurements before and after implementation of SATS-N. Improvements for proportion variables are reported as absolute change (PP), and improvements for time variables are reported as percentage reduction in mean time (%)
Regional network group and survey
In 2017, in the sustainability part of the process, a regional network group, including EMTs, ED nurses, physicians and ED/EMS managers, was established. The purpose was to maintain and improve SATS-N by exchanging experiences and learning from each other. In addition to regular digital meetings, the network group physically met once a year. Developing an e-learning course and offering it as a supplement and alternative to traditional teaching was an important decision.26
In 2018, the regional network group decided to conduct a survey to examine how the users (the EMTs and ED nurses) used and understood SATS-N, according to the official manual and to uncover possible areas for improvement. All health trusts participated in the survey, in which they could assign PLs to a set of clinical vignettes. A triage nurse and a physician prepared assignments (vignettes) based on real adult cases, each with a short description of the patient’s condition and vital signs (online supplemental appendix 2). After pilot testing, the vignettes were distributed to 368 EMTs and ED nurses in the region. The survey also contained questions about some selected background factors, which were believed to be associated with the probability of correct PL assignment for the vignettes.27 28
Results
In a discussion with the front-line personnel and the coach who was in regular contact with the SATS-N users during the implementation process, the project group identified and described a list of challenges and desired effects. Throughout the project, the measured changes were presented and evaluated in each of the health trusts, and feedback was asked for. The project group then prioritised and shortened the list to describe what assumed most relevant. Furthermore, each theme was evaluated against the wanted changes and potential challenges, and connected to QI frameworks and success factors known from the literature. A structured framework like this led to positive results. However, better planning may have reduced unnecessary work in some areas. Table 2 describes the main findings regarding this study; the lessons we learnt connected to the described factors influencing successful QI, challenges and desired effects.
The main lessons learnt from implementing a standardised triage tool in one health region in Norway, connected to the identified challenges and desired effects, and further categorised to the most relevant factors for successful implementation and sustainability
Measurements and improvements
Follow-up measurements, leadership engagement and improvements based on the findings are important efforts in the sustainability part of a QI process.29 The evaluation measurements conducted after implementing SATS-N indicated an increase in the proportion of patients having documented vitals. In addition, we found a decrease in time from ED arrival to patients with sepsis receiving antibiotic treatment compared with baseline measurements (table 1).
Among the 214 EMSs and ED nurses responding to the survey, 82% correctly assigned PLs to the vignettes. This gave moderate agreement and indicated that the EMTs and the ED nurses understood and answered the vignettes according to the SATS-N manual. Online supplemental appendix 2 shows the description of the vignettes with correct PLs. Online supplemental appendices 3–6 present a description about the selection of participants, data collection and statistical methods, the examined background variables for the respondents, the results from the multivariate data analysis and the results of the survey.
The survey uncovered some areas for improvements in the structure of the discriminator list, contents of the discriminators and footnotes. It also led to regional improvement of the content of the discriminators and structuring of the discriminator list according to the ABCDE principles and a new version of the triage tool, SATS-N V.4.0.30–32
Discussion
By implementing a new emergency medical triage tool in one health region in Norway, we learnt the importance of basic measures such as anchoring at all levels: (1) managerial support, (2) support from the EDs and EMSs and (3) support from the involved healthcare providers. Other lessons learnt involved understanding the value of having defined, clearly communicated and specific goals, along with establishing multidisciplinary teams that included the physicians. We learnt that baseline data and evaluation measurement were important for making adjustments and improvements. This was unfamiliar to the EMSs and EDs, and required hard work. The availability of a coach to support and follow-up the users of SATS-N during the implementation phases was a factor for success. Perseverance and keeping spirits high during the QI process were important for the whole process. Using a knowledge-based focus on quality and patient safety, through a systematic theoretical framework like the PDSA process of improvement, was important for the progress and to complete this comprehensive QI work. Significant factors in this QI process correspond to describe success factors that were previously deemed essential for successful QI work in general.
Identifying areas for improving quality and patient safety
Triage ensures that each patient receives similar initial assessment, and should rapidly identify patients in need for immediate care. The EMS and ED take care of a large number of patients in the chain of emergency care. Focusing on quality and patients safety in this part of healthcare can, therefore, have a great effect. Based on this, calculating the cost effectiveness of such measures could have been valuable. This study does not focus on this, but early identification of serious conditions can lead to shorter hospital stays and reduction in complications. These, in turn, can be socioeconomic.
The lack of a common assessment and prioritisation between the EMS and EDs led to disagreement regarding patients’ medical conditions and whether it was necessary for the patient to be transported directly to the hospital. It is of great importance to identify patients suffering from acute conditions, such as sepsis or myocardial infarction, early in the chain of emergency care to provide timely and accurate treatment.15 33–35 Looking back, the focus on implementing a standardised triage tool and timely treatment was a good approach in the process of engaging paramedics, emergency nurses, physicians and their managers in this QI project.
Defining and agreeing on specific goals
Defining goals for improvement was important and a relatively easy process. Patients in Norwegian EDs did not necessarily receive timely treatment.36 The Norwegian health authorities have defined guidance for standard time to treatment for patients with, for example, sepsis. The need for better communication and mutual understanding about patient medical condition between ED nurses and physicians and between EMSs and EDs was a goal several agreed on.
Organisational acceptance and financial support
One of the factors for success in this project, applicable in all health trusts in the region, was to ensure good managerial support before even starting the project. This is because we did not want this to be ‘only a nurse thing’. Involving all levels of care staff, especially the role models, was crucial for success. Without the support of the Western Norway Regional Health Authority’s executive medical directors, the implementation of SATS-N in the entire region would probably not have been achieved. The Western Norway Regional Health Authority funded the project, and this meant that spending time on implementation was acceptable.
Structuring the project
Previous experience with, and the use of, systematic QI tools was valuable when starting this systematic work.5 24 25 37 Even if the first PDSA cycle with one EMS and three EDs was a project itself, it served as a pilot for the whole process. The first cycle gave us valuable experience, useful for carrying out the next cycles, tailoring the SATS-N system to the entire region. The EMSs and EDs which implemented SATS-N later in the process had to complete the same steps in the PDSA cycle as shown in figure 1, except for the choice of type of triage tool. Following all stages in a PDSA cycle can seem overwhelming. However, our experience is that excellent QI work can fail because the necessary steps have not been followed thoroughly. We learnt that one should avoid shortcuts, such as just issuing a new guideline, emailing it to ‘everyone’, and believing the implementation is completed. The work you put into testing and implementation is usually reflected in the results, making sustainability easier to achieve.38
Selecting and establishing the project group
The introduction of a triage system in bureaucratic institutions, such as hospitals, requires multidisciplinary teams of EMTs, ED nurses and doctors with professional and social integrity. In particular, it requires doctors from different professional environments who can be ambassadors for their own departments.39 Our idea was that establishing multidisciplinary teams would raise the chances of success.
Continuous and reliable information to and feedback
Providing continuous and reliable information to the local project managers was a rewarding investment. They communicated directly with colleagues at their own workplace and received important feedback. Feedback on unclear issues often lead to discussions, resulting in necessary adjustments of the tool. We experienced that this increased ownership and team spirit.
Measurements
Selecting the optimal data to be measured was challenging and important for measuring improvements.25 Healthcare providers in the EDs and EMSs were not familiar with systematic QI work or with baseline and evaluation measurements, and required a lot of support from the project management. We learnt that we selected too many variables and records in the first PDSA cycle. For the next cycles, we sampled smaller populations for a smaller data set. One surprise, when measuring baseline data in cycle one, was that respiratory rate (RR) was only documented in 25% of the records in the regional hospital (ED1). The evaluation after implementing SATS-N showed that the proportion of RR values documented increased to 92% (table 1). This project does not contain any specific balanced measures for eventual possible delays in treatment for other patient groups. All health trusts had an adverse event reporting system in place throughout the project, enabling them to identify any negative change in trends. This was not observed, and neither did we perform any cost benefit analysis of the support provided for the intervention versus the cost of some of the adverse events that prompted the change.
Although it took an overwhelming and extensive effort to complete the survey, it was important because it showed the extent to which the users understood SATS-N, and provided a good basis on which areas for improvement could be defined. Analysing the survey led to improvements in the discriminators and the making of footnotes in the SATS-N more understandable, both in content and structure.30 31 40
Coaching and follow-up
One of the most important factors for success was the appointment of one person to be a coach to the health trusts during the process.1 We learnt not to underestimate the importance of having one person who can address questions and relevant issues when they arise—someone who can offer feedback. Besides the patients, the ‘bedside’ workers are important because they contribute to direct value creation in direct patient-orientated work.
Teaching and training
For teaching and training, we used various methods. Initially, we prepared a user manual, presentations and support to give presentations and practical training. Some units accepted offers of training, whereas others wanted to do this on their own. In addition to similar teaching materials and teaching assistance, the e-learning course was an alternative and an addition to traditional training. Not to mention, each chapter in the course ended with a test.29
Implementing the new triage tool in the EMSs and EDS
Introducing and implementing a new triage tool in several EDs and EMSs require knowledge about how people respond to changes and the factors for success and methods of completing QI work.1 5 24 25 The described success factors for QI in healthcare also coincides with the ‘Sigtuna principles’, which describes how organisational interventions need to be implemented.41 It is important to connect with professionals who, despite resistance, are willing to adopt new ideas, are able to convince others of the necessity to test an idea and have the opportunity to implement the desired changes. Rogers’ ‘diffusion of innovation theory’ is still relevant.42 43 Each step in QI work, and the quality of the interactions are important to increase quality and patient safety. This ‘systems thinking’ contributed to set each part together to a whole.22 Implementing SATS-N was a good basis for better communication between nurses and doctors about patients’ conditions in the EDs and making EMTs and ED nurses ‘speak the same language’.
Keeping spirits and perseverance high
Keeping spirits high means spreading enthusiasm from the project managers to local managers, and further to the local teams.3 The project managers’ involvement, combined with an interest from the participants, increased enthusiasm and engagement in developing a tailored Norwegian version of SATS. Perseverance proves to be one of the main key factors in successful QI. Looking back, we thought, ‘Did it really take so long?’
Networking and sustainability
Networking across professions and organisations should not be underestimated. Representation form all participants, in this case from all the EMSs and hospitals in the Western region, ensures anchoring and responsibility for maintaining and updating SATS-N. The regional network group has contributed to keep up the interest and ensure that the triage tool is up to date with medical development and effectively manages changes in the organisation of work. This, in turn, has led to sustainability of the SATS-N.44
Strengths and limitations
This study’s limitation is that other participants in this QI work may have different perspectives and views than described in this study. It can be challenging to describe all aspects that are required by a QI work of this scale. However, this study may provide an overview of lessons learnt. Meanwhile, the evaluations and feedback through the project groups, the coach and the network meetings support the described factors for success. This study’s strength is that the measurements during the test and implementation process are well documented and based on hard data.
In retrospect, we realise that we should have spent more time deciding on how we could have measured whether the changes we made led to improvement, and which variables were important and possible to collect.
Conclusion
Successful QI work in healthcare must combine sound medical knowledge, a systems view and improvement theory and knowledge. We learnt the value of securing managerial support as well as ensuring that the staff is interested and involved in the process. Selecting the best variables for measuring change was another important lesson. Establishing multidisciplinary teams with EMTs, ED nurses and doctors with various medical specialties gave ownership and was a strength in the process of adjusting and implementing SATS to Norwegian conditions. Asking for feedback and being open to questions as well as the availability of coaching during the entire process also provided necessary security for the staff directly involved in caring for patients. In addition, keeping the spirits and perseverance high were important factors in completing the implementation process. Lastly, the establishment of the regional SATS-N network group has been crucial for sustainability and further improvement. Through our project, we experienced that following a structured framework is a critical factor in achieving success in QI work in general.
Data availability statement
Data are available upon reasonable request. Data is uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the data protection officer at Haukeland University Hospital (number: 2017/10514). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors want to thank the colleagues in the emergency departments (ED) and the ambulance services/emergency medical services (EMS) in the Western Health Region, Norway, for relentless participation to make this quality improvement work possible. Participating units: EDs at Førde Hospital, Haugesund Hospital, Stord Hospital, Voss Hospital, Haraldsplass Deaconess Hospital, Stavanger University Hospital and Haukeland University Hospital (HUH) and the EMS at Helse Førde, Helse Stavanger, Helse Fonna and Helse Bergen. We are also grateful to the managers at all levels who supported the project. Thanks to the HUH for providing funds for the initial implementation and to the Western Norway Regional Health Authority who granted funds to complete the implementation of the South African Triage Scale (SATS) Norway. The authors also want to appreciate the permission to modify and use the SATS triage tool free of charge, from the Emergency Medicine Society of South Africa. Special thanks to Aleidis Skard Brandrud (PhD and RN), Mette Engan (MD), Torben Wisborg (professor and PhD) for valuable inputs.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Planning and study design: HSB, MEH and GB. Conducted data analysis for the method in the main manuscript and drafting the manuscript: HSB, MEH, KOH and GB. Advice for data analysis: KOH. Conducted data analysis for supplements: KOH. Revising and finalising the manuscript and final approval of the manuscript: HSB, KOH, MEH, RB and GB. HSB is acting as guarantor of this study.
Funding Haukeland University Hospital funded the initial implementation, and the Western Norway Regional Health Authority granted funds to complete the implementation of SATS-N.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.