Article Text

Statistics from Altmetric.com
Introduction
Thyroid nodules are extremely common1 2; however, most nodules are benign, and even malignant nodules typically follow an indolent course.3 4 With the advancement in ultrasonography and diagnostic techniques, thyroid nodules are biopsied more frequently, and the incidence of thyroid cancer has markedly increased.5 However, mortality from thyroid cancer has remained relatively stable,6 suggesting an increasing trend towards overinvestigation.5
The American College of Radiology published the Thyroid Imaging Reporting and Data System (TI-RADS) in 2017 that aimed to reduce unnecessary investigations of thyroid nodules based on findings on ultrasounds.7 Several studies have shown that, when compared with other risk stratification systems, the TI-RADS guidelines led to a reduction in unnecessary fine-needle aspiration (FNA) biopsies while ensuring most malignant nodules were either biopsied or monitored.8–11 The purpose of this study was to implement TI-RADS guidelines in a tertiary care radiology department with the aim to reduce unnecessary FNAs.
Methods
A process mapping analysis was first conducted to understand the process of thyroid ultrasound reporting and subsequent FNA referrals. Our thyroid ultrasounds are performed by sonographers, who document their preliminary findings on a paper worksheet. The images and the worksheet are then reviewed by a radiologist, who dictates the final ultrasound report. However, sonographers and radiologists documented their findings in varying level of detail, and many reports did not provide sufficient description of thyroid nodules for ordering physicians to determine the TI-RADS risk category.
A lead radiologist (JS) was selected to carry out a stepwise approach to implement the TI-RADS system. This involved educational sessions for radiologists and sonographers, a redesigned sonographer worksheet that incorporated the TI-RADS descriptors and development of a structured dictation template. To optimise the design of the new tools, several plan–do–study–act cycles were carried out to obtain and incorporate feedback from sonographers, radiologists and endocrinologists. Please refer to the online supplemental material for the redesigned sonographer worksheet and an example of a report dictated using the template. The redesigned sonographer worksheet and dictation template was implemented in January and February 2020, respectively.
Supplemental material
To measure the fidelity of implementation for our interventions, 10% of all thyroid ultrasound reports reported between July 2019 and December 2020 were randomly sampled to determine whether the new sonographer worksheet and dictation template were used, and whether the report provided sufficient information on the thyroid nodules to determine next steps as per the TI-RADS guideline.
Our primary outcome measure was the percentage of FNAs deemed unnecessary by the TI-RADS guideline. A retrospective chart review was performed to review FNAs performed between July 2019 and December 2020. Thyroid nodules that were identified as a result of post-thyroid cancer surveillance were excluded. The specialty of the ordering physician was noted as there may be varying experience with the TIRADS guideline among specialties.
Of the nodules that were unnecessarily biopsied based on the TI-RADS guidelines, the number of nodules with a non-benign pathology were measured.
The outcome and fidelity measures were analysed using run charts based on monthly data collection. The data pre intervention and post intervention were also compared statistically using independent t-tests. Significance was defined as p<0.05.
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of this study.
Results
Fidelity of implementation
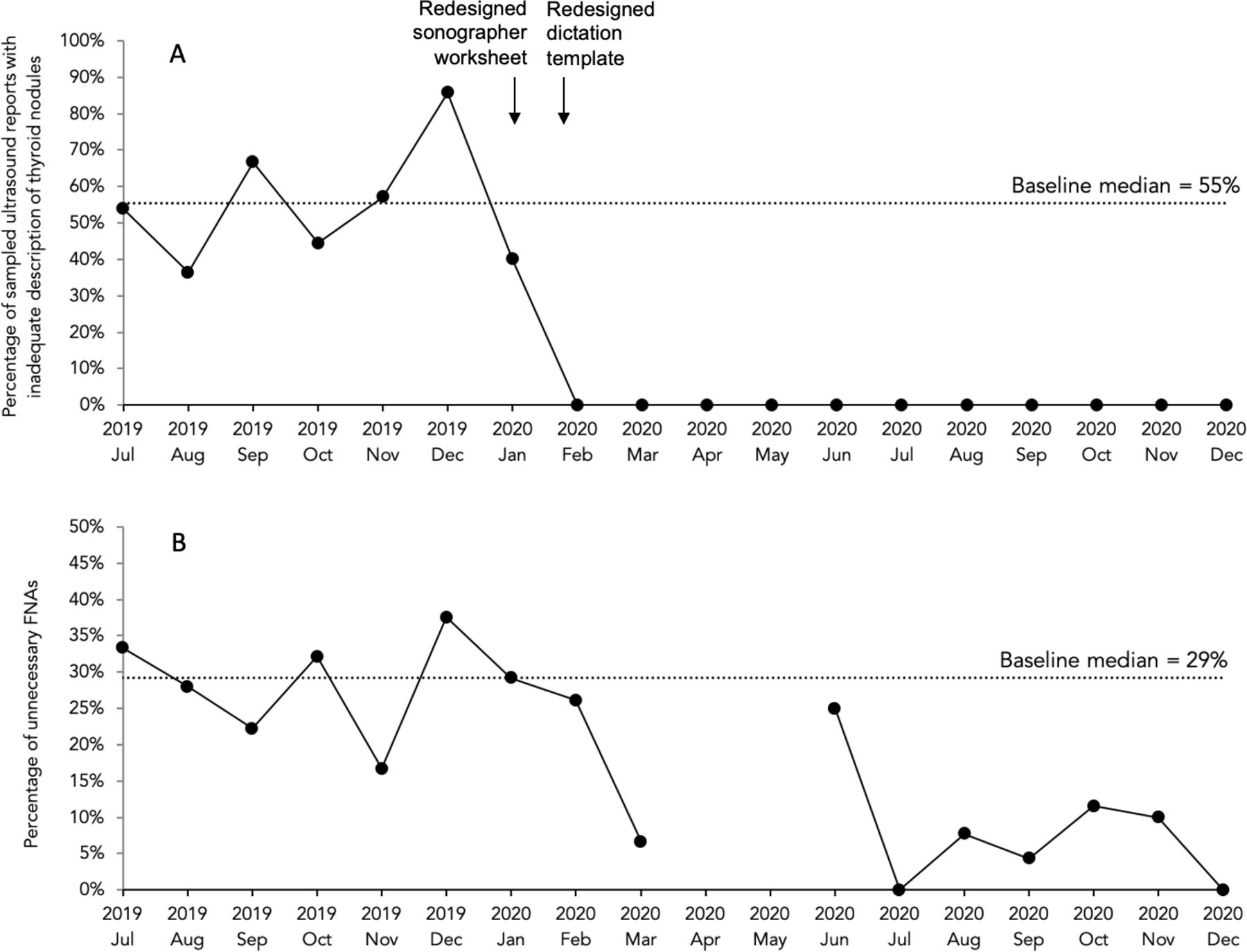
A total of 141 thyroid ultrasound reports (n=63 pre intervention, n=78 post intervention) were included in this analysis. Among the sampled reports, the adoption rate was 100% for the redesigned sonographer worksheet, and 93% for the dictation template. As shown in figure 1, the percentage of reports with inadequate characterisation of nodules decreased drastically after implementation of the interventions (54.9% vs 0%, 95% CI: 0.39 to 0.71, p<0.001).

{kind=link}
(A) Run chart depicting the percentage of sampled ultrasound reports that had inadequate characterisation of thyroid nodules in the preintervention and postintervention period. The arrows indicated when the two interventions were implemented. The dotted line indicates the baseline median of 55% in the preintervention period. (B) Run chart depicting the percentage of unnecessary FNAs in the preintervention and postintervention period. The dotted line indicates the baseline median of 29% in the preintervention period. FNA, fine-needle aspiration.
Percentage of unnecessary FNAs
A total of 334 FNAs were included in this analysis, of which 159 were performed in the preintervention period, and 175 in the postintervention period. Due to the COVID-19 pandemic, there were no FNAs performed in April and May 2020, and only four were performed in June 2020. In the preintervention period, 78.6% of FNAs were ordered by endocrinologists, 10.1% by otolaryngologists, 3.1% by family physicians and 8.2% by other specialists. In the postintervention period, 60.6% of FNAs were ordered by endocrinologists, 11.4% by otolaryngologists, 11.4% by family physicians and 16.6% by other specialists.
The percentage of unnecessary FNAs decreased from 28.3% to 9.7% (95% CI: 0.09 to 0.27, p<0.001) following the implementation of the interventions. As shown in figure 1, there was a sustained shift from June to December 2020 after the interventions were implemented, indicating a special cause variation.
Non-benign nodules not meeting criteria for biopsy
A total of 62 thyroid nodules were unnecessarily biopsied according to the TI-RADS guidelines (n=45 in the preintervention period and n=17 in the postintervention period). Of these, 14 had a non-benign pathology result (n=11 pre intervention, n=3 post intervention); however, 11 of these met criteria for repeat ultrasound follow-up.
Discussion
Our quality improvement initiative led to a significant decrease in unnecessary FNAs. The two interventions to support TI-RADS implementation, a sonographer worksheet and a structured dictation template, were highly adopted, leading to successful standardisation of thyroid ultrasound reports that incorporated the TI-RADS guideline. The result of our study was consistent with that conducted by Griffin et al,12 where a structured reporting template based on the TI-RADS guideline resulted in improved quality of thyroid ultrasound reports with better description of thyroid nodules and definitive management recommendations.
Although a small number of non-benign nodules would have been missed after implementation of TI-RADS, we believe the reduction in harm related to overinvestigation outweighs that of missing a small portion of malignant nodules that are most likely indolent.
Several key elements contributed to our initiative’s success and high adoption rate of the interventions. Education sessions ensured sonographers and radiologists understood the rationale for changing the reporting system and increased engagement. We also employed user-centred design principles and worked closely with our end users throughout the design and implementation process.
In terms of limitations, given the TI-RADS system requires more features of each thyroid nodule to be described, a balancing measure is that sonographers and radiologists have to spend more time assessing and documenting their findings. Thyroid ultrasound appointments were extended by 10 min after implementation of the TI-RADS system, but the amount of extra time required was not formally quantified during our study. It is expected that the time needed will decrease as sonographers becomes more familiar with TI-RADS and with subsequent scans for the same patient.
In summary, we described a successful quality improvement initiative involving the implementation of the TI-RADS reporting system, leading to standardisation of thyroid ultrasound reports and in turn, significant reduction in unnecessary FNAs of thyroid nodules. The general principles of standardisation and user-centred design can be widely applied by others when implementing TI-RADS or other best practice guidelines.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but as per local institutional guideline at Sunnybrook Health Science Centre, REB approval was not required for our local quality improvement project.
Acknowledgments
The authors thank the sonographers, radiology residents and radiologists at Sunnybrook Health Sciences Centre for their input into this project and their dedication to improving patient care.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AW conceived the study. AJC analysed the data and drafted the manuscript. All authors contributed to the development of the study protocol, interpretation of the data, revisions to the manuscript and approval of the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests IJH has received speaker and consulting fees from Dexcom, 374 Abbott, Novo Nordisk, Sanofi and Tandem.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.