Article Text

Abstract
Background Procedural time-outs and checklists are proven to be an effective means of improving teamwork and preventing wrong-sided procedures. The main objective of this study was to ensure that all regional nerve blocks being performed in the preoperative area at our hospital were executed with a proper time-out. The goal of this project was to increase integration of a safe preoperative block process including a time-out checklist to ensure; complete consents, correct patient and laterality were marked prior to each procedure. We focused on recognising events that took place before, during and after the nerve block including non-compliance with the checklist and deviations from protocol.
Methods A safe preoperative block process current and future state flowchart, revised time-out checklist and action/implementation plan as part of our Plan–Do–Study–Act model was constructed using a multidisciplinary approach. Pre-implementation and post- implementation data were collected by medical students acting anonymously via direct observation noting the presence of an anaesthesiologist, resident, nurse, time-out for procedure, checklist completed and procedure start and sedation time representing a complete time-out.
Results The direct observations in the pre-implementation group showed a 20% (3/15) compliance with a correct time-out. The direct observations in the post implementation group showed 85% (12/14) compliance. This revealed a 65% increase in all portions of the time-out checklist completed. Comparative analysis confirmed decrease in non-compliance and deviations from protocol as displayed by 65% increase in all portions of time-out checklist completed.
Conclusion We aimed to improve safety, communication and compliance for preoperative nerve blocks through development and implementation of a safe preoperative block process using a multidisciplinary model. We conclude that creation of a safe nerve block was achieved by integration of a preoperative nerve block process which included increased compliance to the time-out checklist, verifying patients and laterality with marking of patient prior to each procedure, identifying proper consents were completed and ensuring each regional nerve block was executed with a proper time-out.
- anaesthesia
- checklists
- communication
- compliance
- quality improvement
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Preoperative nerve blocks were being performed without a proper time-out, consents were sometimes missing or incomplete, laterality was not consistently checked and there was poor communication between nursing, surgery and anaesthesia.1 While a pre-procedure checklist was informally being used, compliance was only 20% by initial direct clinical observations. There were two ‘never events’ that were wrong-sided blocks within a 6-year period, as well as an incident of wrong medication administration and a recent event when sedation was given prior to a surgical consent being completed. This indicated that the checklist was not being used properly and prompted the initiation of this intervention. Failure to do a pre-procedure time-out is unsafe for our patients and resulting complications are entirely preventable. The aim was to ensure that all regional blocks done in the hospital preoperative and holding area are done with a proper time-out (with registered nurse (RN), anaesthesia attending and resident) immediately prior to the regional block, before sedation is given, as well as optimising compliance with the time-out checklist.2 Time-out will encompass completing all parts of the time-out sheet in the presence of all essential personnel.
The hospital is a busy training institution where the anaesthesia department regularly performs an average of 10–12 preoperative nerve blocks daily. Nerve blocks are used to provide surgical anaesthesia as well as postoperative analgesia, but it is an invasive procedure where sedation and a high volume of local anaesthetics are often administered. The procedure should ideally be done only after completion of surgical consent and marking as well as anaesthesia consent and marking along with verification of limb laterality. However, the busy and pressured perioperative environment is a factor in missing checks that ensure patient safety.
The project team consisted of a multidisciplinary team of leaders in various fields including nurses, physicians, hospital administrators, residents and medical students with an aim to increase compliance of the time-out process from 20% to 80% within 5-month intervention time period.3 Medical students involved contributed by performing direct observations anonymously, verifying compliance with the time-out checklist and presence of each staff member including nurse, attending physician and resident. The residents role was execution of time-out checklist and additionally the writing of the manuscript. Each multidisciplinary field was involved in the Plan–Do–Study–Act (PDSA) cycles contributing their ideas to improving compliance and safety.
Measurement
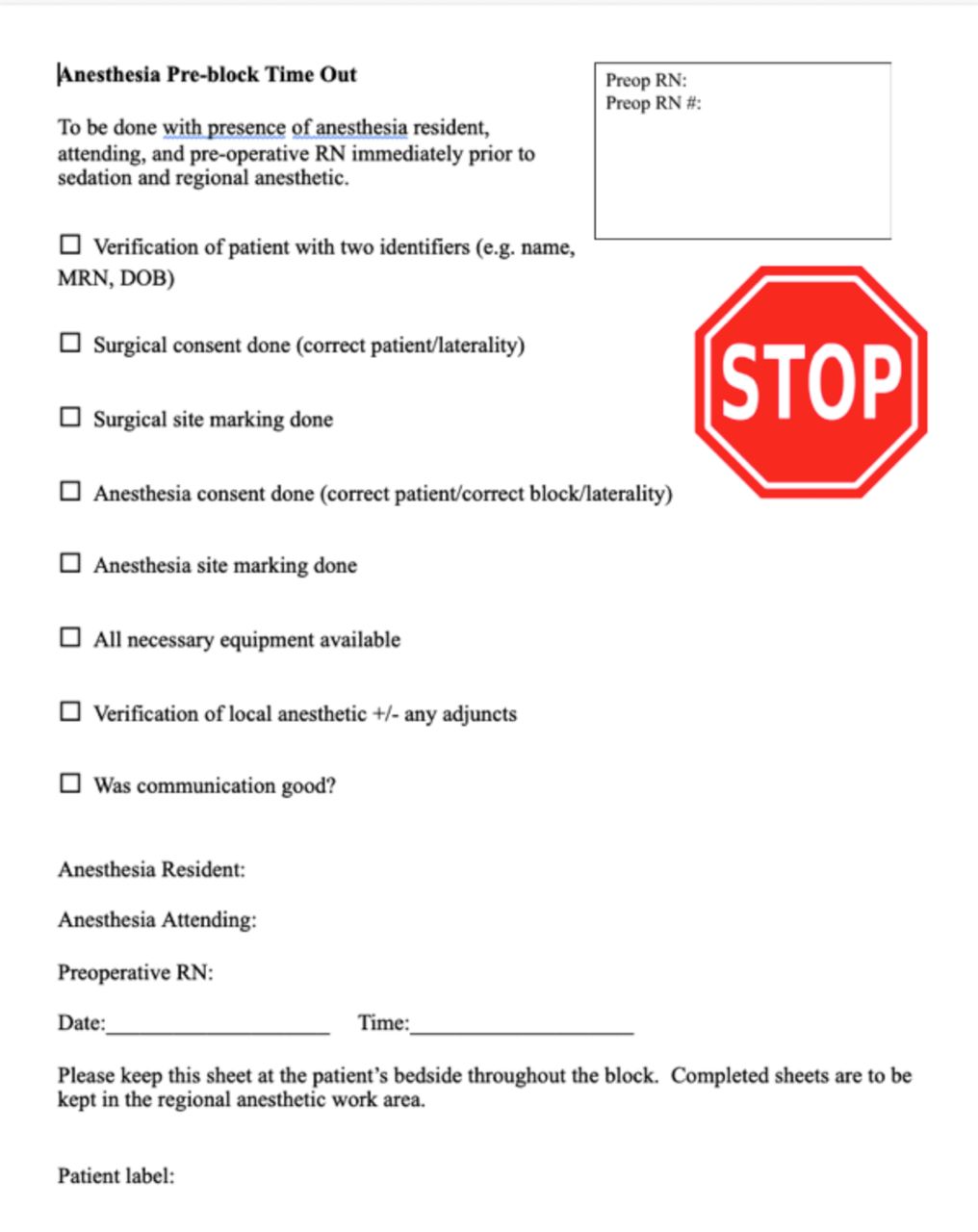
The Standards for Quality Improvement Reporting Excellence guidelines were referred to in the preparation of this report.4 Direct clinical observations of 29 preoperative nerve block time-outs were performed from December 2019 to January 2020 at the hospital which is a large 716-bed, level one trauma academic hospital with 35 operating rooms (ORs) situated on separate two floors. Observations were not randomised and were sampled by convenience. Orthopaedic surgery patients in the preoperative and holding area on the second floor was targeted specifically for observations. No specific person or staff was targeted. The observations were obtained by study staff using a standardised Excel sheet to assess preoperative nurse, anaesthesia attending and resident compliance with the time-out checklist (figure 1). The observers did not divulge their purpose when they entered the preoperative bay for each nerve block, in order to diminish the influence of performance observation on nurse, anaesthesia attending or resident. The observers recorded compliance for each element of the time-out checklist, presence of each member of the team including preoperative nurse, anaesthesia attending and resident, as well as if a time-out was performed or not. Elements of the time-out checklist that were verbalised and filled out in completion by the anaesthesia attending performing the time-out were considered compliant. Other events that occurred were also noted during the time-out process including the verbalised time-out time, the sedation and block start time.

Anaesthesia pre-block time-out sheet. DOB, date of birth; MRN, medical record number; RN, registered nurse.
Design
The quality improvement project team consisted of three project sponsors including the director of quality improvement, the chair of anaesthesia, one perioperative nurse manager, one lead physician anaesthesiologist, two physician anaesthesiologists, two resident physicians, a nurse project facilitator and two medical students. Different tools were used to evaluate and analyse the current process and areas of insufficiency within the patient pathway. Tools primarily used were, first, anonymous direct observations by medical students. In addition, the direct observations were randomised with no specific nurse, anaesthesiologist or resident being evaluated on a predetermined notion. Second, a current state process flow diagram was created to further identify areas of improvement. Lastly a future state process flow diagram was developed and used for continued optimisation of the process and sustainability by being on display in the preoperative areas for education and compliance of current and new staff.
Initially, a current state process map (figure 2) was developed to ensure the project team understood the various members involved and steps required to have the necessary pieces in place to go through a time out. The preoperative surgical patient journey was documented in a progressive manner, from arrival in preoperative area to block time. Areas for improvement and barriers were identified including delays or inefficiencies in the process. A future state process map (figure 3) was also developed for further analysis to determine the necessary interventions to streamline the process.

Flow diagram at initial education meeting reflecting current state. H&P, history and physical; IV, intravenous; OR, operating room; RN, registered nurse.

Flow diagram reflecting changes, future state. anes, anaesthesia; H&P, history and physical; IV, intravenous; IVF, intravenous fluids; PCC, patient care coordinator; meds, medications; OR, operating room; preop, preoperative; pts, patients; RN, registered nurse.
After process mapping, we invited a broader team of OR nurses and administrators from the hospital to further identify details in the pathway and obstacles. This process again exposed deficiencies with the current process and appropriate interventions that could be applied with the broader multidisciplinary team present. The project team met weekly from September 2019 to February 2020 during the cycles. Baseline data was obtained from September to November and implementation began from end of November.
In order to produce improvement consistent with our goal and within our reach we decided to limit our measurement efforts to the preoperative area on a single floor focusing on outpatients with the goal to provide the same care throughout the entire preoperative area.
There were 15 improvement interventions that were created in response to the areas of concern which we tested by completing four PDSA cycles across a 20-week period.5 Most of the practitioners were amenable to the changes though some areas of anticipated risks for unsuccessful compliance with the new process were the time factor for a proper time-out and filling out the checklist in its entirety given the busy and pressured perioperative environment.
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Strategy
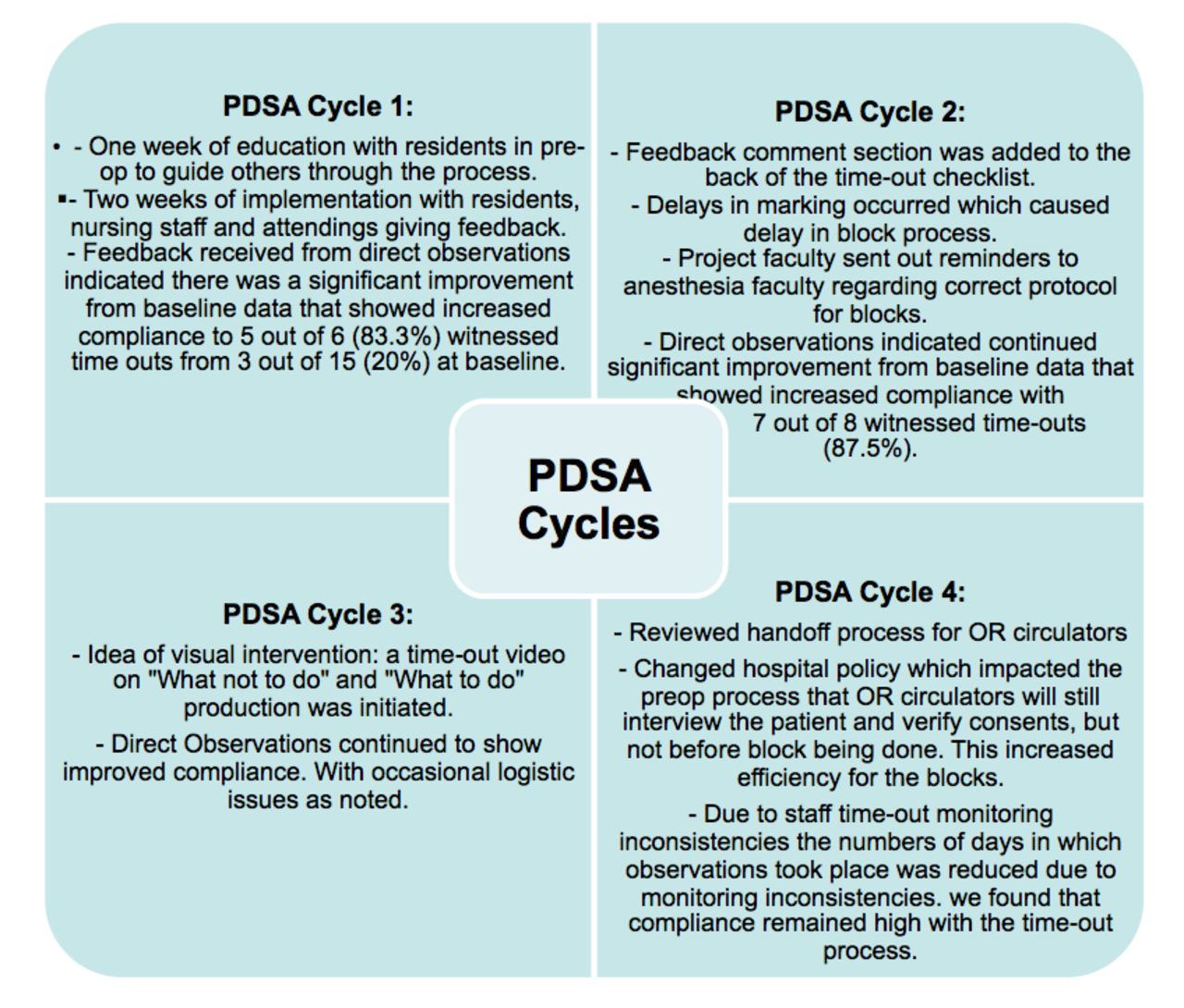
Our SMART aim was to ensure that all our regional blocks done in the hospital preoperative and holding area were done with a proper time-out, which encompassed completing all parts of the time-out sheet in the presence of all essential personnel so that 80% are compliant at the end of 20 weeks.6 Four PDSA cycles were performed to accomplish this (figure 4).
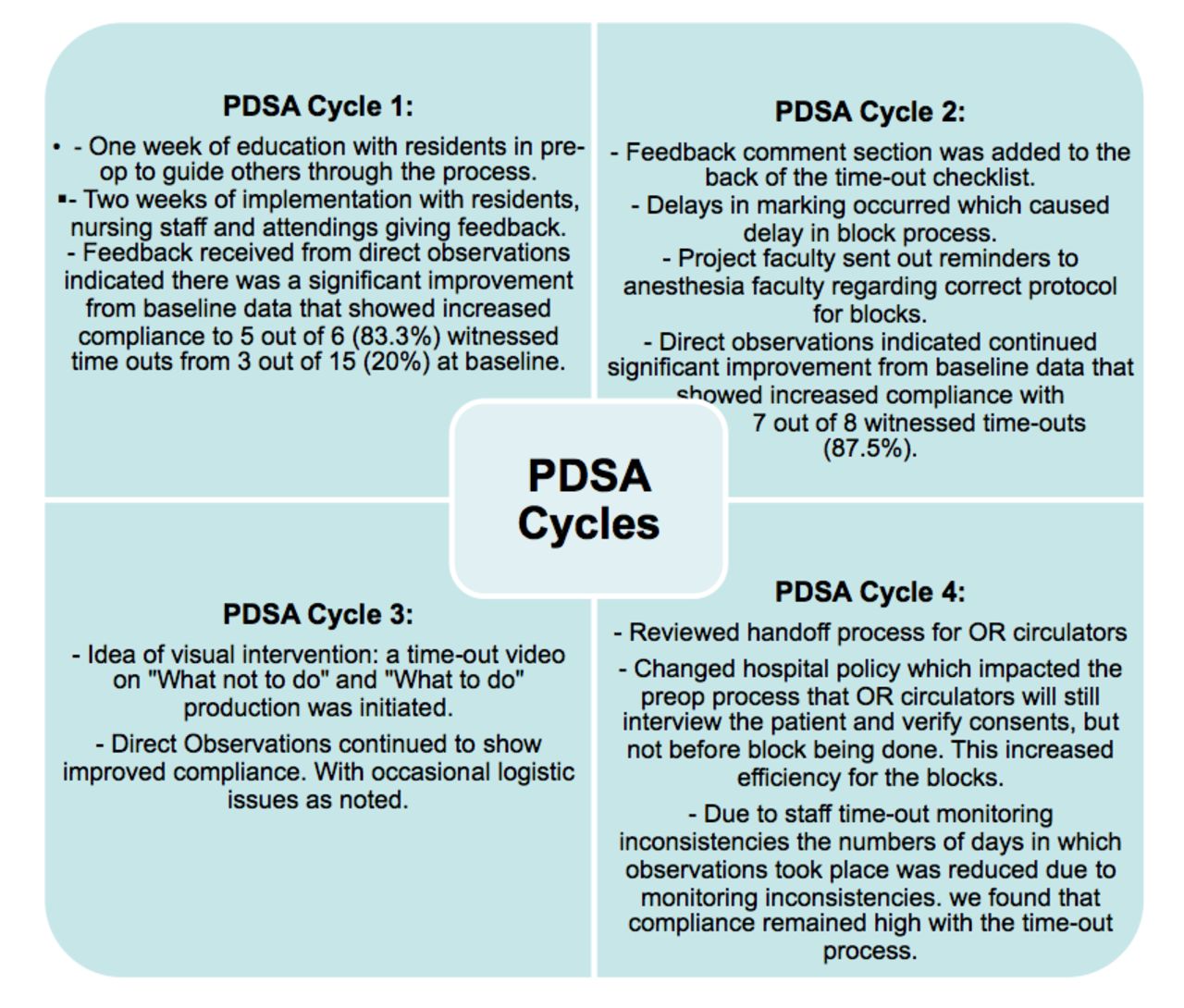
PDSA cycle process diagram. OR, operating room; PDSA, Plan–Do–Study–Act; preop, preoperative.
Our initial intervention consisted of education of staff for 1 week with clearly defined tasks and roles for each team member, and implementation of our action plan for 2 weeks (see online supplemental file 1). Attendings educated attendings, nursing educated their peers and residents educated residents. Measurements and monitoring for compliance took place for 2 week and we reconvened after the cycle for adjustments.7
Supplemental material
Our action plan (see online supplemental file 1) consisted of additional roles and tasks for each member of the team. Including identifying elective block patients 1 day prior by the resident and marking on the electronic operating room schedule board for clarity and so preoperative nurses were aware they would be required for a time-out. Anaesthesia residents were to also contact the orthopaedic surgery attending by 14:00 the day prior to confirm elective block patients and the OR board would be updated with response. On patient arrival, preoperative nurse would then assign elective block patients to specific bays, which also made it easier to monitor post block given that the patients receive sedation. After vitals were, obtained, the preoperative nurse would leave on monitors (blood pressure, pulse ox, EKG), connect IVF (intravenous fluids), check consents, verify surgical site marked, place nasal cannula and make sure time-out checklist is at bedside. Nurse then marked ‘P’ on ORC (operating room computer) board indicating preoperative is done and OR circulator is aware. The preoperative nurse number was presented on the board to contact when ready for block. The OR circulator would then evaluate the patient and a handoff was performed and ‘H’ marked on ORC board indicating handoff is complete prior to block and sedation (preoperative RN follow-up cases preoperative RN will call circulator to do handoff). Anaesthesia faculty and resident team did time-out led by attending with preoperative RN present. The time-out checklist was also completed at that time to ensure patient safety and documentation was complete. When block was complete anaesthesia resident updated board and informed preoperative RN ‘block done’ and preoperative RN continued to monitor patient. The process is reflected in (figure 3) ‘the future state flow chart’.
PDSA cycle 1
During the first cycle we had a week for education where designated residents from the project team were present in the preoperative area on the second floor each morning to follow-up and answer questions about the new process (figure 3). They were also available to remind the various residents who were rotating on regional anaesthesia of their roles with emphasis on the time-out and revised time-out checklist with all essential members present. A PDF of the action plan with various roles was emailed as well as posted in the preoperative block area. We then had 2 weeks for implementation at which point we encouraged the residents, attendings and nursing staff to write comments on the checklists about the process. Feedback included that the time-out checklists are being filled out but without specific comments on the process. Some attendings showed up late or were not involving preoperative nursing in the time-out especially for first start cases. Additional feedback noted that putting on monitors and nasal cannula is really helpful for the anaesthesia team. There was difficulty in locating preoperative nurse sometimes as they were taking care of multiple patients. During this transition an adjustment period occurred, as was expected, due to people being assigned to new roles and responsibilities of specific tasks that they previously did not conduct. Feedback received from direct observations indicated there was a significant improvement from baseline data that showed increased compliance to 5 out of 6 (83.3%) witnessed time-outs from 3 out of 15 (20%) at baseline (figure 4).
PDSA cycle 2
A feedback comment section was added to the back of the time-out checklist. During this cycle there was difficulty with regional anaesthesia residents taking the initiative to contact the orthopaedic surgery attendings the day before. There were delays in surgical teams marking the surgical site in a timely manner delaying block process. The plan was for one of the team attending anaesthesiologists to touch base with orthopaedic attendings to make sure they were on board and understood the process as well as to emphasise the need for early surgical site markings for this process to work smoothly. The project faculty was also sending out emails to anaesthesia attending’s to emphasise the need to arrive on time, lead the time-outs and include nursing staff. Direct observations indicated there continued to be significant improvement from baseline data that showed increased compliance with seven out of eight witnessed time-outs (87.5%) (figure 4).
PDSA cycle 3
We hypothesised that in order to further build and strengthen our new process, a visual intervention would be beneficial for staff. Therefore, a time-out video on ‘What not to do’ and ‘What to do’ production was initiated. We went over producing the time-out video including writing scripts, which was delegated to the medical students and residents. Hospital staff were chosen to be actors for the video. Direct observations continued to show improved compliance with occasional logistic issues as noted (figure 4).
PDSA cycle 4
For our final cycle, we reviewed the handoff process for the OR circulators with the OR nurse managers. Hospital policy was changed which directly impacted the preoperative process that the OR circulators will still interview the patient and verify consents, but they will not have the pressure of doing this prior to sedation or the block being done. This would increase efficiency for the blocks. We found that compliance remained high with the time-out process in the final cycle with the above changes (figure 4).
Results
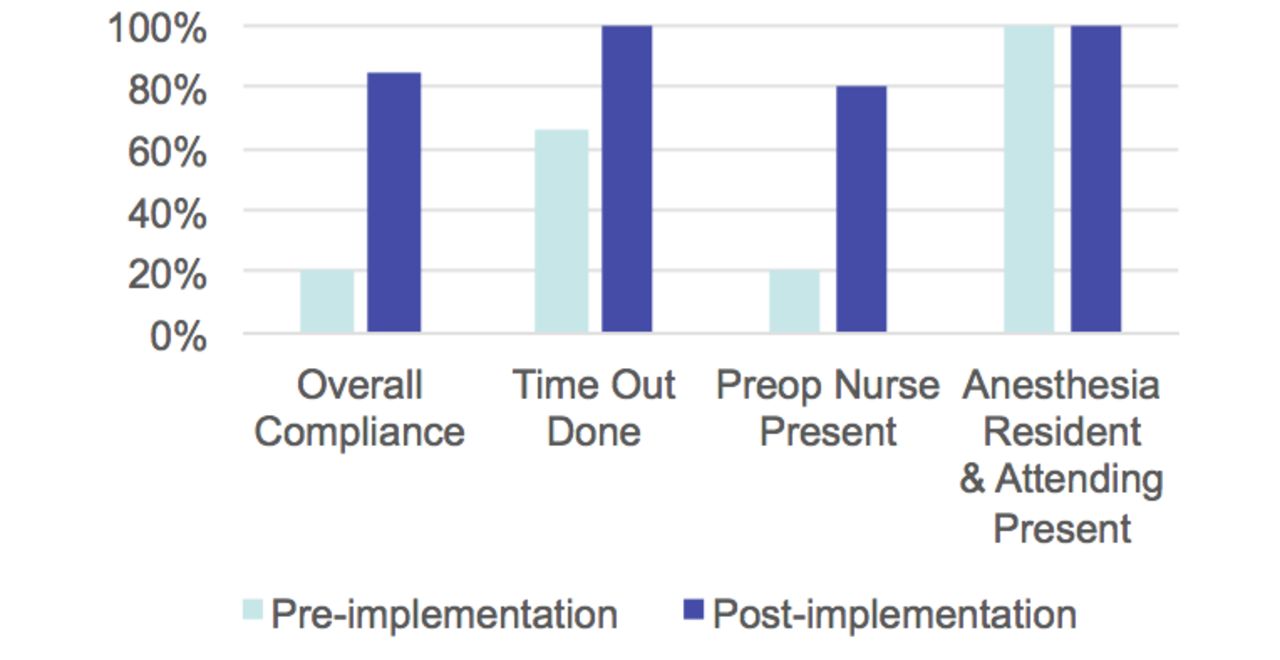
Our main outcome measure was compliance with the time-out process including completion of the checklist with all essential team members present and measured via direct observations of trained project team members.8 The compliance improved quickly from baseline and remained high, from 20% to 85%9 (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
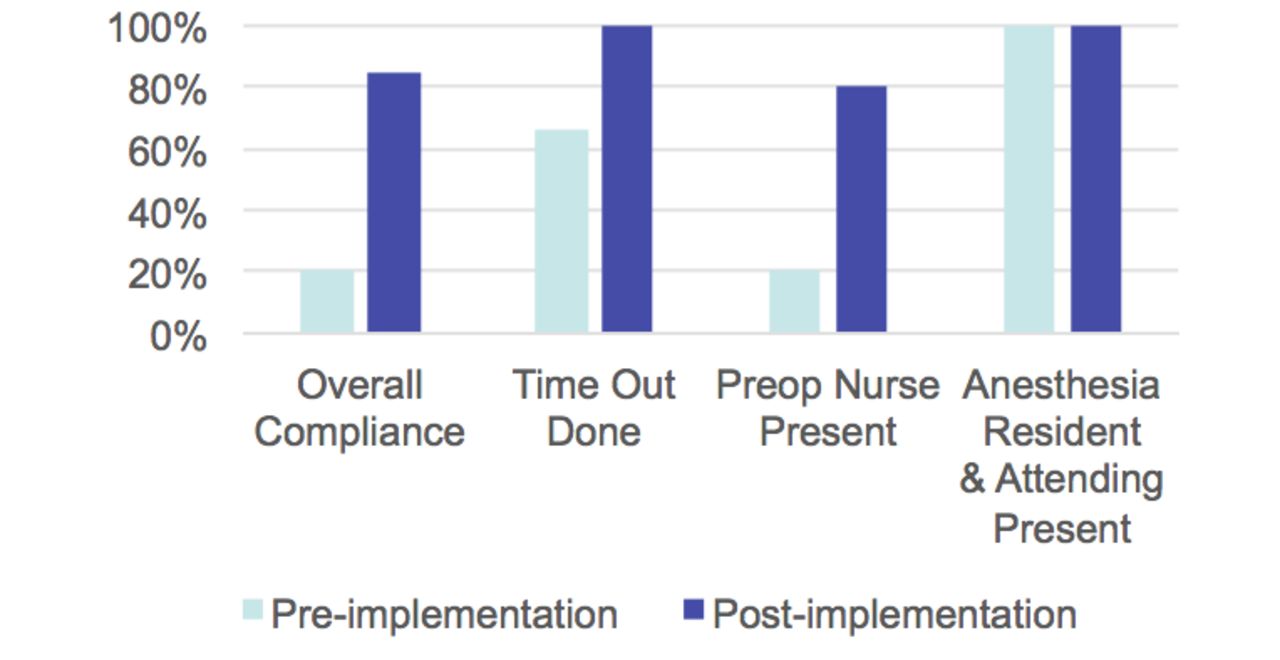
Results bar graph. preop, preoperative.
A period for assessment of baseline data via direct observations showed preoperative nurse was present 20% (3/15) for time-out, anaesthesia attending and resident present 100%, all components of time-out checklist was completed 20% (3/15), time-out for procedure completed in 66% (10/15). Weekly direct measurements were obtained post implementation and showed the preoperative nurse was present 80% for procedure time-out, anaesthesia attending and resident present 100%, all portions of revised time-out checklist was completed 85% (12/14), time-out procedure was performed in 100% (14/14) of cases prior to sedation time and block start time. In two cases the nurse was present for identification of patient and then left and never came back. There was 60% improvement in compliance with nursing staff presence and 44% improvement in compliance with time-out for the procedure. There was 65% increase in all portions of time-out checklist completed. Comparative analysis demonstrated an increase in compliance with the implementation of the safe preoperative block process (figure 5).
Lessons and limitations
The project aim was to ensure that all our regional blocks done at the hospital preoperative and holding area were done with a proper time-out, which encompassed completing all parts of the time-out sheet in the presence of all essential personnel. To achieve this, we made significant modifications to the existing preoperative nerve block process. Building on existing ideas, we also wanted a process that improved safety and communication between anaesthesia, nursing and surgery teams.10 It can be stated that the compliance-promoting measures made an important contribution to this result.11 A key lesson learnt during the process was the importance of PDSA cycles, which helped to ensure the integrity of the multidisciplinary model and that each step was optimised prior to implementation of interventions.
As strong multidisciplinary communication rests at the core of the process, we made sure that anaesthesiologists, residents, nurses and administrators were involved throughout the process including discussions, planning, collecting written feedback and attending meetings.10 Their input during the planning was essential to increase their support for a viable new process. Notwithstanding, we did identify certain implementation problems, which we attribute to the fact that it was not possible to meet with the entire nursing staff, surgery faculty, anaesthesia faculty and residents. Having included a surgery resident or faculty surgeon initially in the project team may have improved this issue of the process.
Project implementation exposed the obstacles of staff acceptance to a new process. Despite prompt positive results it can take time to establish new sustainable routines especially in higher pressured environments where efficiency is important such as the perioperative areas. Qualitative feedback from staff post implementation has been vital in refining the process and we believe is essential for long-term success.8 The qualitative feedback does suggest the need for continued education as staff turnover ensues and new residents arrive. A time-out video of what to do and what not to do is in production in order to encourage long-term sustainability of the process. The hospital’s creative media service has reviewed the script for the block time-out video with plans for filming to commence soon. Additional anaesthesia and orthopaedic surgery attendings agreed to participate in the video improving our multidisciplinary model. We should have a date for filming soon.
Finally, we primarily focused on nerve blocks located on the second floor preoperative area at the hospital and did not obtain data in other areas of the hospital including the third floor preoperative area or post-anaesthesia care units. Therefore, we have drawn our conclusions based on observations restricted to one area, which is a limitation. We have not performed any statistical tests to prove that these results are not a product of chance. In order to overcome this, ideally more data would need to be collected over a longer time period and statistical tests would need to be performed. There is also the possibility of confounding bias, for example, due to the change in anaesthesia residents on regional every 4 weeks, and the hiring of new anaesthesiologists throughout the year both of which may have positively impacted the time-out process, independent of our intervention.
Another limitation is how we collected our data. Ideally, this would be an automated, bias-free, systematic process. However, the project relied on medical students to manually collect and observe each procedure so there is observer bias. There were also limitations to the number of procedures they were able to see because of prior engagements in their own schedule.
Although the new preoperative nerve block process has substantially helped to improve compliance with the time-out checklist and communication between the various teams, continued monitoring for sustained commitment to the process and compliance is necessary. For this to be improved further, a future project should look into applying the safe preoperative block process to all areas of the hospital where nerve blocks are performed. This is an opportunity we hope to pursue in the near future.
Conclusion
Non-compliance with the preoperative nerve block time-out and checklist can lead to adverse events. This study’s goal was to ensure that all regional nerve blocks in the preoperative/holding area at the hospital were executed with a proper time-out with a nurse, anaesthesia attending and resident immediately prior to the regional block and before sedation. The implementation of a safe preoperative block process including a revised time-out checklist was used to increase compliance with the time-out procedure and facilitate good communication between the multidisciplinary teams. Results displayed significant improvement with compliance from baseline data and sustainable over an extended period of months.
Evidence has shown that procedural time-outs and checklists have been proven to be effective means of improving teamwork and preventing wrong-sided procedures. Increasing evidence also shows that these effects translate into safer patient outcomes. Our project has demonstrated that simple interventions can improve compliance and communication among nursing, anaesthesia and surgery teams. There were no wrong-site or wrong-person blocks reported at our hospital during the study period.
Although the new preoperative nerve block process has substantially helped to improve compliance with the time-out checklist and communication between the various teams in a limited area, continued monitoring for sustained commitment to the process and application on a larger scale is necessary. For this to be improved further, a future project should look into applying the safe preoperative block process to all areas of the hospital where nerve blocks are performed. This is an opportunity we hope to pursue in the near future.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Author JCA and coauthors VL, FR, TA and KD conceived initial idea, processed the experimental data, performed the direct observations and analysis, drafted the manuscript and designed the figures. All authors discussed the results and commented on the manuscript, contributed to the design and implementation of the quality improvement report and to the writing of the manuscript. Author and coauthors acknowledge project sponsors: Emily Volk, MD; Lisa Devane, MSN; and Ms Polly Smith, RN; and quality improvement project members: Matt McClure, MD; Wendy Kang, MD; Naveen Mehra, MD; and Beena Chorath, RN, who were involved in planning meetings, implementing and supervising the work. Author JCA is responsible for overall content acting as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.