Article Text

Abstract
Background Community management of atrial fibrillation (AF) often requires the use of electrocardiographic (ECG) investigation. Patients discharged following treatment of AF with fast ventricular response (fast AF) can require numerous ECGs to monitor rate and/or rhythm control. Single-lead ECGs have been proposed as a more convenient and relatively accurate alternative to 12-lead ECGs for rate/rhythm management and also diagnosis of AF. We aimed to examine the feasibility of using the AliveCor single-lead ECG monitor for diagnosis and monitoring of AF in the community setting.
Methods During the course of 6 months, this evaluation of a clinical service improvement pathway used the AliveCor in management of patients requiring (1) follow-up ECGs for AF with previously documented rapid ventricular rate or (2) ECG confirmation of rhythm where AF was suspected. Twelve AliveCor devices provided to the acute community medical team were used to produce 30 s ECG rhythm strips (iECG) that were electronically sent to an overreading physician.
Results Seventy-four patients (mean age 82 years) were managed on this pathway. (1) The AliveCor was successfully used to monitor the follow-up of 37 patients with fast AF, acquiring a combined total of 113 iECGs (median 1.5 ±3.75 per patient). None of these patients required a subsequent 12-lead ECG and this approach saved an estimate of up to £134.49 per patient. (2) Of 53 patients with abnormal pulses, the system helped identify 8 cases of new onset AF and 19 cases of previously known AF that had reverted from sinus back into AF.
Conclusions We have demonstrated that the AliveCor system is a feasible, cost-effective, time-efficient and potentially safer alternative to serial 12-lead ECGs for community monitoring and diagnosis of AF.
- community health services
- quality improvement
- clinical governance
- continuous quality improvement
- cost-effectiveness
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- community health services
- quality improvement
- clinical governance
- continuous quality improvement
- cost-effectiveness
Strengths and limitations
This is the first pilot initiative to demonstrate the feasibility of using a structured algorithm to facilitate the integration of single-lead ECGs into community monitoring and diagnosis of atrial fibrillation (AF).
The AliveCor is US Food and Drug Administration approved and NICE evaluated, and therefore has the potential for wider integration into community AF management.
The sample size is small, and the study is conducted in a single health board.
Introduction
Atrial fibrillation (AF) is a spectrum of disease and affects around 5.5% of adults aged 55 years and over.1 It can be either paroxysmal, persistent or permanent, and although some patients may be asymptomatic, it is often associated with symptoms such as palpitations, breathlessness, fatigue and reduced exercise capacity. Patients with symptomatic AF are treated with either a rate or rhythm control strategy. Rate control is often the first-line approach for AF with an onset of greater than 48 hours, and can be achieved with acute and then long-term use of beta-blockers, calcium channel blockers, cardiac glycosides or combination therapy. Beta-blockers are considered first-line long-term therapy for patients with persistent or permanent AF and symptoms related to rapid ventricular rate (fast AF) for symptomatic relief. Community follow-up monitoring is necessary to guide effective treatment. Conventionally, 12-lead ECGs have been used, but the advent of reliable single-lead ECGs with accurate built-in AF detection algorithms have the potential to streamline this monitoring process.
Single-lead ECGs could also have a role in community detection of AF. A diagnosis of AF can be difficult to make in the community as up to 62% is paroxysmal and up to 40% is asymptomatic.2 3 In the UK, AF is detected through opportunistic investigation as systematic screening is currently not recommended by the UK National Screening Committee predominantly due to a lack of outcome evidence.4 Detection is important because new-onset AF is thought to account for one-fifth of patients hospitalised for ischaemic stroke.5 Indeed, AF is a well-established independent risk factor of ischaemic stroke,6 with convincing evidence for direct causality.5 Having controlled for confounding, device-detected AF lasting at least 1 hour in 3 months (0.046% of the time) is associated with a 2.11-fold increase in stroke risk compared with no AF.7 Anticoagulation in the form of direct oral anticoagulants or adjusted-dose warfarin reduces stroke risk by over 60%.8 NICE recommends anticoagulation in moderate- to high-risk patients.9
Previously, when ECG investigation had been required, our Acute Community Team in the Neath Port Talbot area have had to rely on undertaking a 12-lead ECG in the community. This can be a cumbersome and lengthy process that risks inappropriate tachyarrhythmia management, missed or delayed diagnosis of paroxysmal AF with adverse implications for initiation of appropriate anticoagulation. There is mounting evidence for the utility of integrating single-lead ECGs into healthcare provision in a number of settings.10–16 This pilot initiative aimed to test the feasibility of integrating a single-lead hand-held ECG system, the AliveCor, into community monitoring of treatment in patients with recently diagnosed fast AF and opportunistic community diagnosis of AF.
Method
Participants and setting
This evaluation of a clinical service improvement pathway enrolled a total of 74 patients from the Neath Port Talbot community between June and November 2017. Participants were eligible for inclusion if patients had been referred to the Acute Community Team with (1) known fast AF requiring monitoring and management, and (2) suspected AF due to an abnormal pulse on manual pulse check. There were no specific exclusion criteria. Baseline characteristics are recorded in table 1.
Patient characteristics
Patient and public involvement
When asked, patients have expressed similar thoughts around the cumbersome nature of obtaining 12-lead ECG monitoring. Patients were involved at the stage of results collection. After providing informed verbal consent, patients were encouraged by the Acute Clinical Team to provide feedback on use of the AliveCor, which contributed to our results and discussion section.
Single-lead ECG device (AliveCor—KardiaMobile)
The AliveCor Kardia Mobile system (AliveCor, Mountain View, CA) consists of a battery-powered pair of electrodes and a Smartphone-based application linked using ultrasonic audio.17 The iECGs produced are a 30 s single-lead rhythm strip likened to lead 1 of a 12-lead ECG. iECGs can be input into accurate automatic algorithms (sensitivity 98%, specificity 97%) to detect AF.18 It is possible to store multiple iECGs and send them using WiFi securely to a physician. In this initiative, a local experienced academic clinical staff member trained the Acute Community Team members in using the AliveCor. Twelve AliveCor devices were provided to the community teams.
Community atrial fibrillation monitoring
Hospital discharges of newly treated AF with rapid ventricular response were referred to the Acute Community Team for ECG monitoring to ensure appropriate rate or rhythm control. Figure 1 shows how in the situation where a 12-lead ECG was not available, the AliveCor was used to direct optimised medical therapy. We recorded the number of iECGs required per patient and whether any further 12-lead ECG monitoring was required after use of the AliveCor (figure 2).
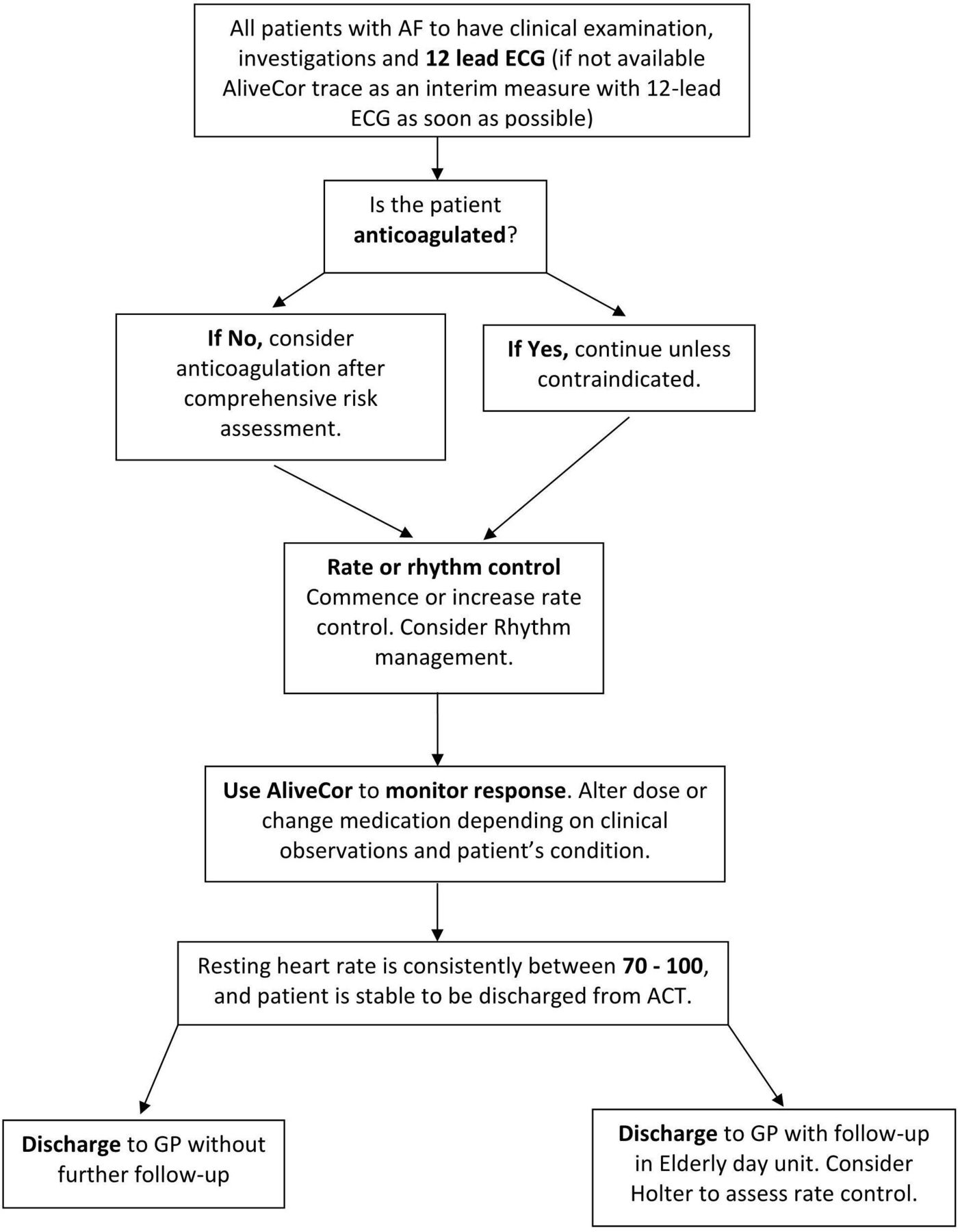
AF monitoring—patient flow for participants referred with fast AF or whom develop fast AF while under the care of the ACT. ACT, Acute Community Team; AF, atrial fibrillation; GP, general practitioner.
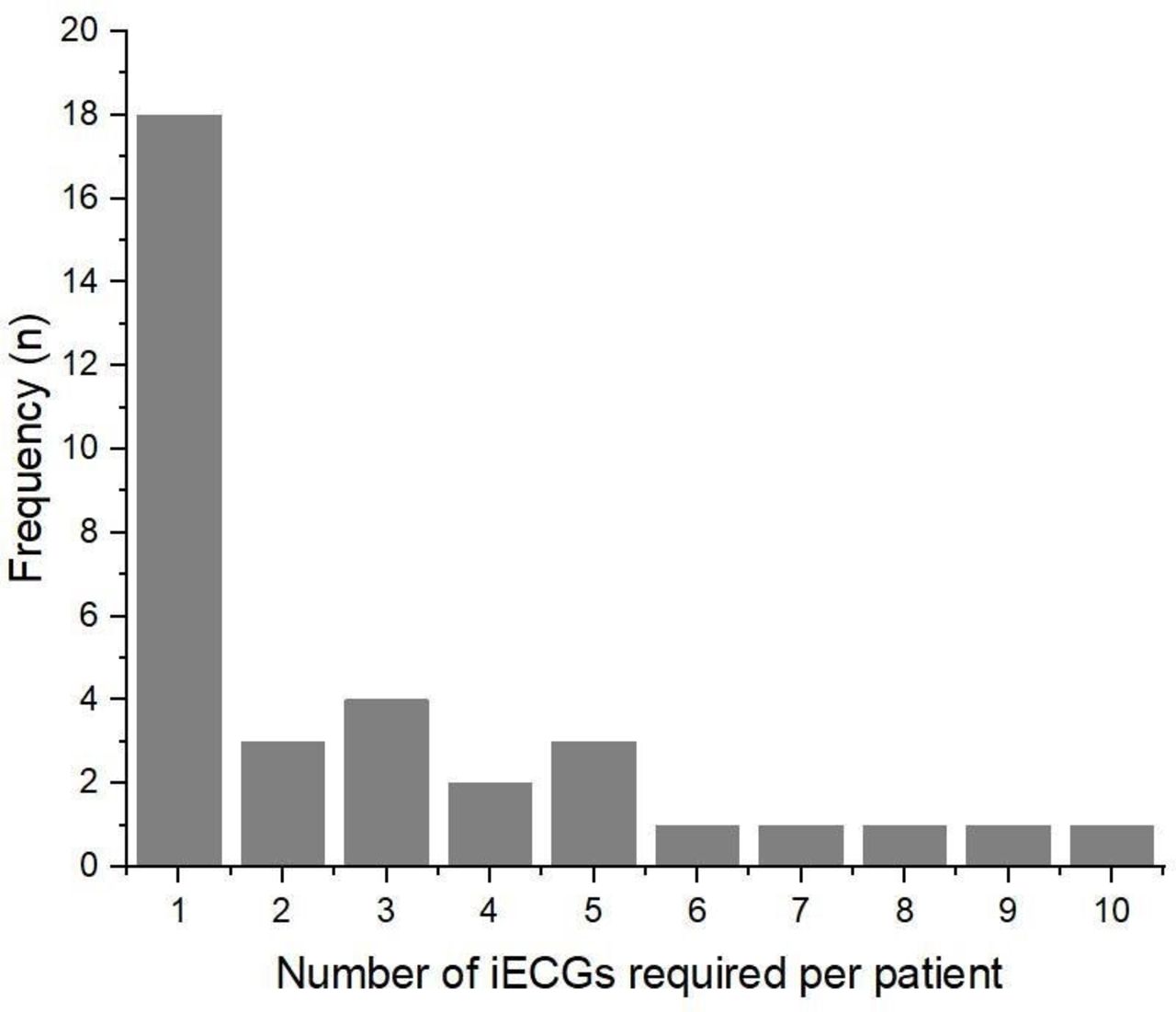
Histogram showing the number of iECGs per patient taken over a 6-month period.
Community atrial fibrillation diagnosis
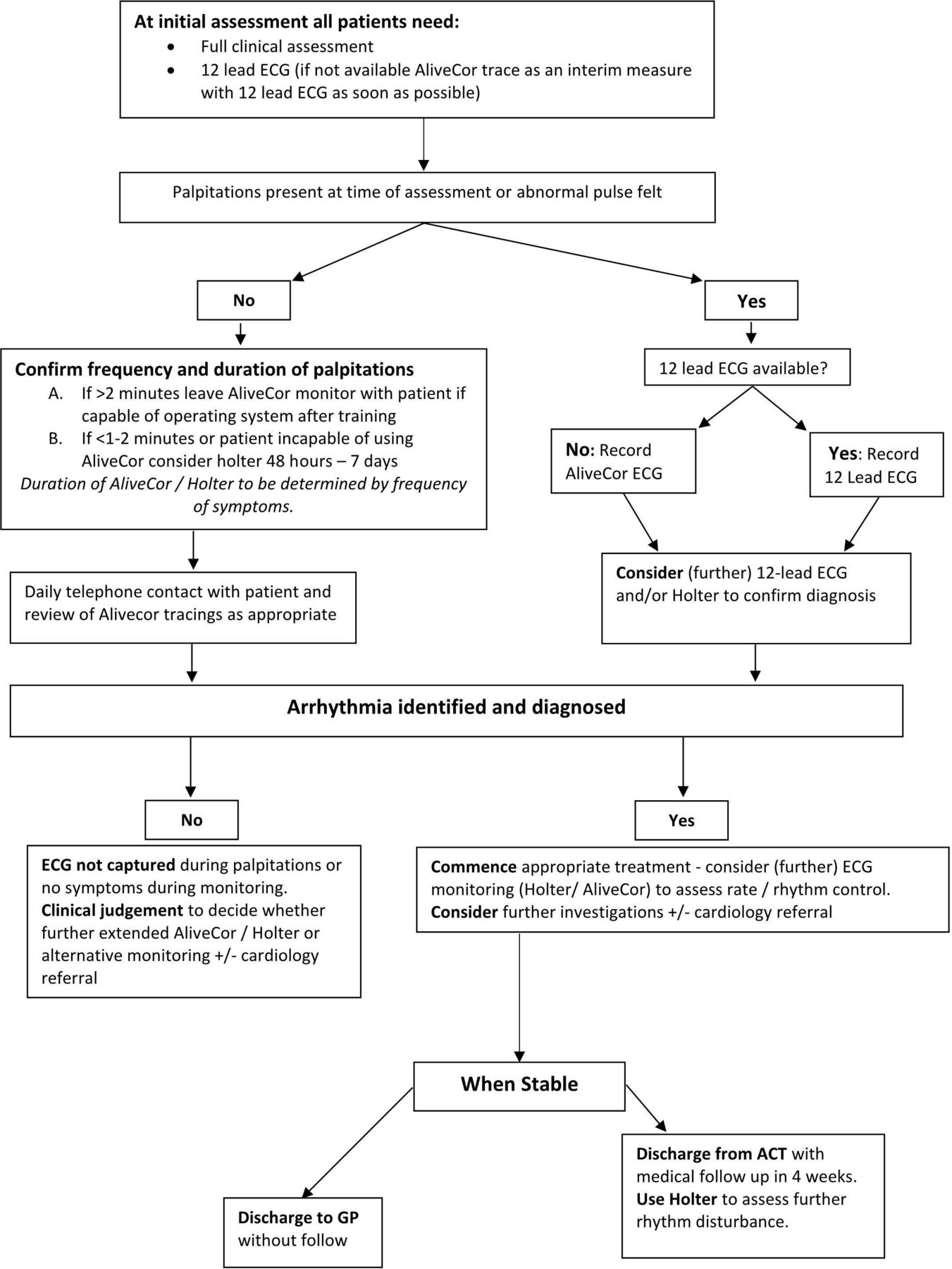
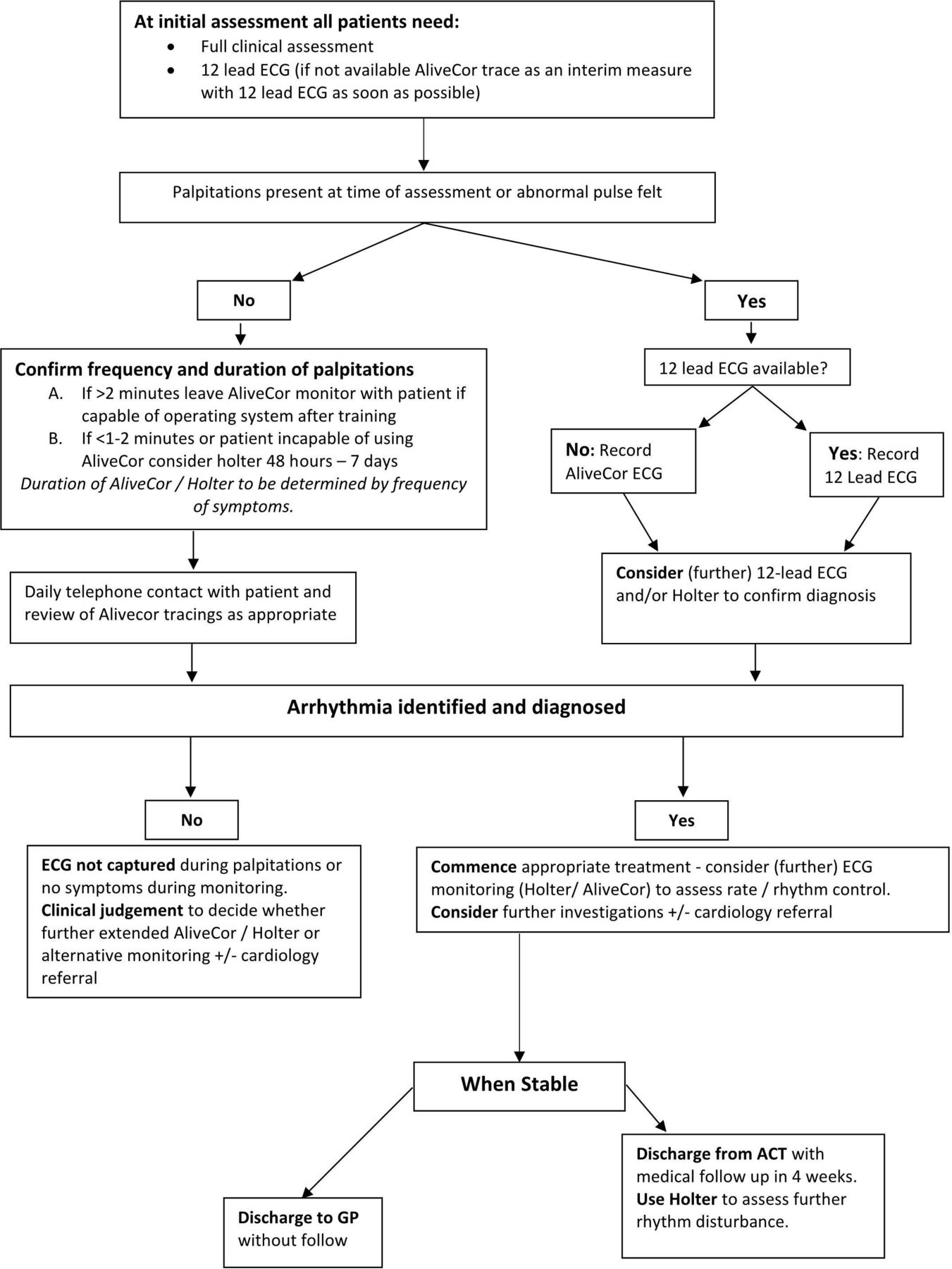
As demonstrated in figure 3, patients with symptoms consistent with AF were referred to the Acute Community Team for an initial clinical assessment. If the rhythm of the pulse was ‘abnormal’ or if the patient reported palpitations at the time of assessment, an ECG would be necessary. The AliveCor device was used if a 12-lead ECG was not immediately available. Had the use of the AliveCor not been possible, ambulatory Holter monitoring would have been arranged. We recorded the number of patients found to be in AF, and other rhythm disorders as interpreted by a cardiologist (table 2).
{kind=link}
{kind=link}
{kind=link}
AF diagnosis—patient flow for patients with symptoms consistent with AF or an ‘abnormal pulse’ on palpation. ACT, Acute Community Team; AF, atrial fibrillation; GP, general practitioner.
Diagnoses using single-lead iECGs
Cost-effectiveness
In 2019, NICE estimated the cost of a 12-lead ECG with either general practitioner (GP) or cardiologist overread to be between £12.34 and £5219 and each AliveCor device to cost £62.49+VAT.20
Statistics
Descriptive statistics were calculated and graphical data were presented using IBM SPSS V.26. OriginPro 2019b was used to construct the bar graph (figure 2).
Ethical considerations
According to WHO and Healthcare Quality Improvement Partnership guidance, risk–benefit analysis was performed internally. The proposal was deemed to be a ‘patient safety activity’ as the AliveCor was used within a standard of care framework, the approach was tailored to improving provision of care in Swansea Bay University Health board, and the initiative did not involve vulnerable populations. The patient safety activity was considered of ‘minimal risk’ as it did not change treatment plans, data were not individually identifiable, the intervention did not divert staff from existing responsibilities and implementation did not constitute an elevated level of risk to patients or staff.
Results
Baseline characteristics of the total 74 participants recruited (n=37 monitoring, n=53 diagnosis) can be found in table 1. Participants were a mean age of 81.3 years and were predominantly female (female:male, 54:20). No participants were lost to follow-up.
Community atrial fibrillation monitoring
The 37 patients requiring ECG monitoring for follow-up of fast AF, required a total of 113 iECGs (median 1.5 ±3.75 per patient). The majority of patients only required one follow-up iECG to confirm adequate rate or rhythm control (figure 2). However, some patients required up to 10 iECGs to titrate medication dose to appropriate clinical effect. There were no cases in which a 12-lead ECG was required due to the single-lead ECG not being sufficient. In terms of cost-effectiveness, assuming a 12-lead ECG would have been performed where in our initiative an iECG was required, the 12 AliveCor devices saved between £495 and £4976 according to NICE 2014 estimates, depending on GP or cardiologist overread.19 20 This equates to an average of £13.37 and £134.49 per patient requiring follow-up ECG monitoring.
Community atrial fibrillation diagnosis
Of the 53 patients assessed, 8 were found to have new-onset AF, 19 patients with known AF (noted to be in sinus rhythm prior to index assessment) were found to have reverted back to AF, 7 had ‘other’ ECG abnormalities and 19 were normal (table 2). Of the eight patients found to have new onset AF, five were female, with an average age of 78.3 years (SD ±7.1 years) and an average CHA2DS2-VASc score of 4.9 (SD ±0.85, range 3–6). All agreed to be appropriately anticoagulated. We found that as iECGs could be easily uploaded via a secure internet connection, they could be overread by a physician in an appropriately timely manner.
Discussion
This single health board clinical service improvement pathway evaluation included 74 participants over a 6-month period using the US FDA–approved AliveCor. To our knowledge, this is the first pilot initiative to demonstrate the feasibility of using a structured algorithm to facilitate the integration of single-lead ECGs into community monitoring and diagnosis of AF. We found that the AliveCor device was easy to use, more time-effective and cost-effective, and successfully prevented the need for serial 12-lead ECGs in the community. Of the 37 patients requiring ECG monitoring, 113 iECGs were needed and of the 53 patients with an ‘abnormal’ pulse, 15% were found to be in new-onset AF and were appropriately anticoagulated.
There are a number of commercially available portable ECG devices which are suitable for out-of-hospital use, ranging from one-lead to three-lead ECG devices. Portable ECGs have the advantage that they are easy to carry, relatively lightweight and low cost. The advantages of the AliveCor system is that it is (1) immediately accessible as an iECG, (2) portable, (3) user-friendly due to a filter for noise reduction and (4) is US Food and Drug Administration (FDA) approved and NICE evaluated.20 A recent meta-analysis by Duarte and colleagues examined the diagnostic accuracy of single-lead ECGs in four studies in asymptomatic individuals by a cardiologist or electrophysiologist and found a sensitivity of 93.9% (95% CI 86.2% to 97.4%) and a specificity of 96.5% (95% CI 90.4% to 98.8%) for diagnosing AF,21 which is considerably superior to manual pulse palpation (specificity 78.8%, 95% CI 51.0% to 94.5%).22
The AliveCor is the most widely studied single-lead ECG device, but there are other examples such as the Omron HeartScan23 or the Zenicor ECG24 which do not require smartphones. There are also wearable three-lead ECGs such as the ZioPatch25 and the Nuvant mobile cardiac telemetry.26 Three-lead ECGs appear to be comparable with single-lead ECGs when assessing most intervals27; however, they do require longer application periods to obtain true readings and there can be a greater delay in accessing and reporting the ECG data.25
Integration of single-lead ECG devices into existing pathways has been demonstrated to be feasible in primary care,10 11 opportunistically in pharmacies,12 13 in low-resource settings,14 in rural areas15 and on a large scale.16 Similarly to our findings, all of these studies found a high degree of successful operator use. Six of these studies comment on uninterpretable traces and describe low rates with an average of 0.82% (SD ±0.52%, range 0% to 1.3%). All of these studies report at least one training session as being sufficient for operators. In comparison with 12-lead ECGs, Holter monitoring and invasive event recorders, single-lead ECGs only require finger contact. Moreover, iECGs are designed to be transferred, analysed and stored. Once the application is set up, the system is relatively straightforward. Indeed, the vast majority of patients also appear to find the device easy to use.28
Limitations and challenges
To further evaluate the incorporation of single-lead ECGs into community AF diagnosis and monitoring pathways, this design can be extended to other health boards, increased in duration and participant number. Use of the AliveCor KardiaMobile was particularly valuable if there was a lack of time or if patients preferred not to undress for a 12-lead ECG. It was not difficult to obtain a trace with help, even in patients with poor dexterity or cognitive impairment. One of the main challenges encountered by the team was WiFi connectivity when out in the community on home visits. This meant that the clinical staff sometimes had to wait for a WiFi signal to resume before upload of iECGs was possible. With regard to documentation, particular care was taken to ensure traces were named. This was less of an issue with the online platform which comes with the AliveCor device (The Kardia Pro system). We collected verbal instead of written consent for inclusion, which limited our collection of patient data.
Cost-effectiveness
Another potential barrier to the integration of opportunistic use of single-lead ECGs in the National Health Service (NHS) is cost-effectiveness. The AliveCor appears to be a sustainable solution in the follow-up of AF with fast ventricular response as we saved an average of £13.37 to £134.49 per patient. Cost-effectiveness of single-lead ECGs have been demonstrated in similar circumstances. The multicentre, randomised trial (n=243) by Reed and colleagues investigated the use of the AliveCor during symptoms over a 90-day period as opposed to ambulatory ECG monitoring.29 They found the AliveCor device saved £474 per patient compared with standard care. Moreover, Duarte and colleagues have estimated the cost-effectiveness of using single-lead ECGs in a primary care setting compared with routine, opportunistic AF detection using manual pulse palpation.21
Ongoing benefits
We found that use of the AliveCor in the community cut down the number of patients needing to return to clinic. Moreover, the AliveCor is now used by our community team’s clinicians in the field and also in clinic to quickly assess and confirm a patient’s cardiac rhythm.
Conclusion
This initiative demonstrated the feasibility of integrating single-lead ECGs into NHS provision of community healthcare for patients with AF. We found that the AliveCor was a useful clinical adjunct to standard care as it provides an accurate, point-of-care elucidation of patient rhythm, saving valuable time and money in the delivery of acute community medical services.
References
Footnotes
JJHB and EFL contributed equally.
Contributors JJHB is responsible for data formulation, data analysis, figure design, literature review, writing the original manuscript, editing the final manuscript and project administration. EFL is responsible for contributing to data formulation, figure design, contributing to writing the original manuscript and editing the final manuscript. FA contributed to running of the initiative and data collection. SK contributed to data collection. KW contributed to data formulation and was in charge of data collection and running of the initiative. JPJH conceptualised the initiative, reviewed the literature and made substantial contributions to editing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.