Article Text

Abstract
Background Medication adherence impacts health outcomes. Healthcare organisations implementing system-level interventions have potential for greater spread and sustainability than individual-level interventions. Within the integrated US Veterans Health Administration, a multidisciplinary team developed and evaluated a pilot quality improvement programme to assess the feasibility of automatic mailed prescription refills for patients with diabetes and low medication adherence (assessed by medication possession ratio <80%).
Methods Patients were randomised to usual care with self-initiated refills versus automatic mailed refills for 6 months. Process outcomes included glycaemic control measures (HgbA1C), medication possession ratios for both automatic and self-initiated (reference) refills of medications, patient satisfaction and workforce effort (pharmacist time).
Results Overall, 199 patients were randomised to automatic refills (n=99; 40 of whom participated) versus usual care (n=100). In multivariable analysis adjusting for baseline differences, after 6 months there was no difference in the proportion of patients with follow-up HgbA1C <8% (60.8% automatic refills vs 60.5% usual care, p=0.96). In the automatic refill group, the medication possession ratio for reference medicines was significantly higher than usual care (63.9% vs 54.5%, 95% CI (for difference) 3.1% to 15.9%, p<0.01).
Conclusions Implications and lessons from this pilot programme include potential beneficial indirect effects from automatic medication refills on patient self-initiated refills of other medications; the importance of tailoring solutions to patient subgroups and specific adherence barriers; and recognition that the rapid deployment, iteration and evaluation of the project was facilitated by a multidisciplinary team embedded within an organisational learning health system.
- diabetes mellitus
- quality improvement
- chronic disease management
Data availability statement
Data are available upon reasonable request. Data for this study were collected for local quality improvement efforts at the VHA Puget Sound Health Care System. Consistent with operational, non-research activities conducted by the US Veterans Health Administration, a deidentified limited data set that supports the findings of this study is available from authors upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Prior studies have shown some success in improving medication adherence through automating pharmacy refills for chronic disease medications, yet none have occurred in the unique integrated US Veterans Health Administration (VHA), mailed medications to patients’ homes, nor focused on diabetes.
WHAT THIS STUDY ADDS
This project describes a randomised pilot test of automating mailed refills of diabetic medication for patients with low medication adherence. Lessons related to the implementation of the project within the VHA are also reviewed, including the importance of a multidisciplinary project team embedded within the VHA’s learning health system.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Patients with prior low medication adherence randomised to receiving automated mailed refills of diabetic medications had positive associated effects on self-initiated refills for non-automated usual medications, with implications for health systems seeking to improve patient medication adherence.
Introduction
Low medication adherence is associated with adverse clinical outcomes, including increased mortality.1 2 Previous efforts to improve adherence rates frequently employed multicomponent interventions and have had mixed success.3–5 Among individual-level adherence interventions, evidence suggests that behavioural strategies (eg, habit based) are more effective than cognitive interventions (eg, knowledge-based or educational efforts).5–7 System-level approaches to adherence have also deployed choice architecture principles, based on behavioural economics, where individuals are ‘nudged’ towards decisions that promote health through redesign of the environment.8 9 Examples of ‘nudge’ interventions for medication adherence have included pill monitoring, adherence feedback and medication reminders.10–12 Pharmacy-based automated refill programmes, affecting behaviours of individuals through systems redesign, have successfully combined these evidence-based best practices to improve adherence. A multitude of programmes have evaluated autosynchronisation of medication refills, automated reminders for overdue prescriptions or autorefills of chronic medications for pick-up at a pharmacy.13–17 However, to our knowledge, there have not been programmes that automate both the refill and home delivery of medications for chronic diseases, systematically reducing barriers to providing medications ‘in hand’. Furthermore, no automated refill programmes have occurred within the unique integrated environment of the US Veterans Health Administration (VHA).
The VHA is the largest US integrated healthcare system, serving over 6 million active patients and has an increasing ability to act as a learning health system to support improvements in diabetes care.18 Learning health systems play a key role in facilitating improvements in complex areas, including leveraging electronic databases and conducting embedded, operationally partnered research and quality improvement.19 Medication adherence interventions may have differential effects in the VHA for two main reasons. First, patient barriers to adherence may be greater in the VHA. For example, among older (≥65 years) patients eligible for either VHA or Medicare services, those seen predominantly in the VHA had worse social, economic and health risk factors (eg, food insecurity, lower self-rated mental health). Many of these factors are also associated with lower medication adherence for patients with chronic disease.20–23 Moreover, the VHA operates with a standardised patient-centred medical home model in its over 900 primary care sites, which might differentially affect patient adherence to care plans compared with patients seen in other care environments.24 At baseline in the VHA, patients self-initiate medication refills online, by phone or in person at VHA pharmacies. Most (80%) medication refills are then mailed to the home from centralised VHA mail-order pharmacy services.25
This project implemented and tested the feasibility of a pharmacy process change initiating automatic mailed refills of diabetes medications to improve medication adherence among patients with diabetes and low medication adherence in one regional VHA network (VHAPUG). In 2019, the VHAPUG was below VHA national averages for glycaemic control in patients with diabetes, with 60.8% of patients having a well-controlled glycated haemoglobin (HgbA1C <8%) compared with 65.2% of patients nationally. A multidisciplinary team conducted this project, which was facilitated by local and national organisational commitments to operate as a learning health system and enabled by formal, collaborative, existing operational research partnerships supported by the VHA Office of Primary Care.26 27
Methods
Project overview
This was a randomised quality improvement pilot test of the feasibility and preliminary effects of automatically refilling and mailing medications among patients with diabetes and low medication adherence. Data on patient demographics, pharmacy refills and outcomes were from VHA databases.28 Missing demographics for patients (n=5) were supplied through manual chart review. Qualitative patient satisfaction data were collected from notes taken during brief (<5 min) structured telephone follow-up calls with patients. Baseline data were collected in April 2019. The intervention was conducted from April to December 2019, and outcome data were collected through June 2020. Data analysis occurred from April to August 2021. This project was designated non-research quality improvement by the VHAPUG Institutional Review Board. All patients receiving automated refills provided informed consent to participate in the programme. This manuscript follows the Standards for Quality Improvement Reporting Excellence 2.0 (online supplemental file 1).29
Supplemental material
Patient and public involvement
An initial review of the materials, workflows and protocol was reviewed by five veteran patients with diabetes during the preparatory period of this project; iterative updates were made to the programme based on their feedback. Enrolled patient participants provided qualitative feedback to the team after the conclusion of this pilot project; this feedback will be used for adjustments to the protocol and materials prior to future scaling of this process change.
Patient participants
Patients with diabetes were included if meeting the following criteria: (a) military service-connected disability rating >30% (the 2019 threshold for eliminating medication copayments); (b) HgbA1C in the prior 12 months; (c) ≥1 refill of an outpatient oral diabetes medication from the VHAPUG pharmacy in the past 6 months; and (d) a low medication possession ratio (MPR <80%). MPR is a validated administrative measure of medication adherence, defined by the formula: [(Days of medication supply obtained during time period) / (Days in time period)] × 100.30 Patients were excluded if they were unable to be reached for consent, if they declined participation, were unable to receive mailed refills or were unable to communicate in English.
Automatic refills and usual care groups
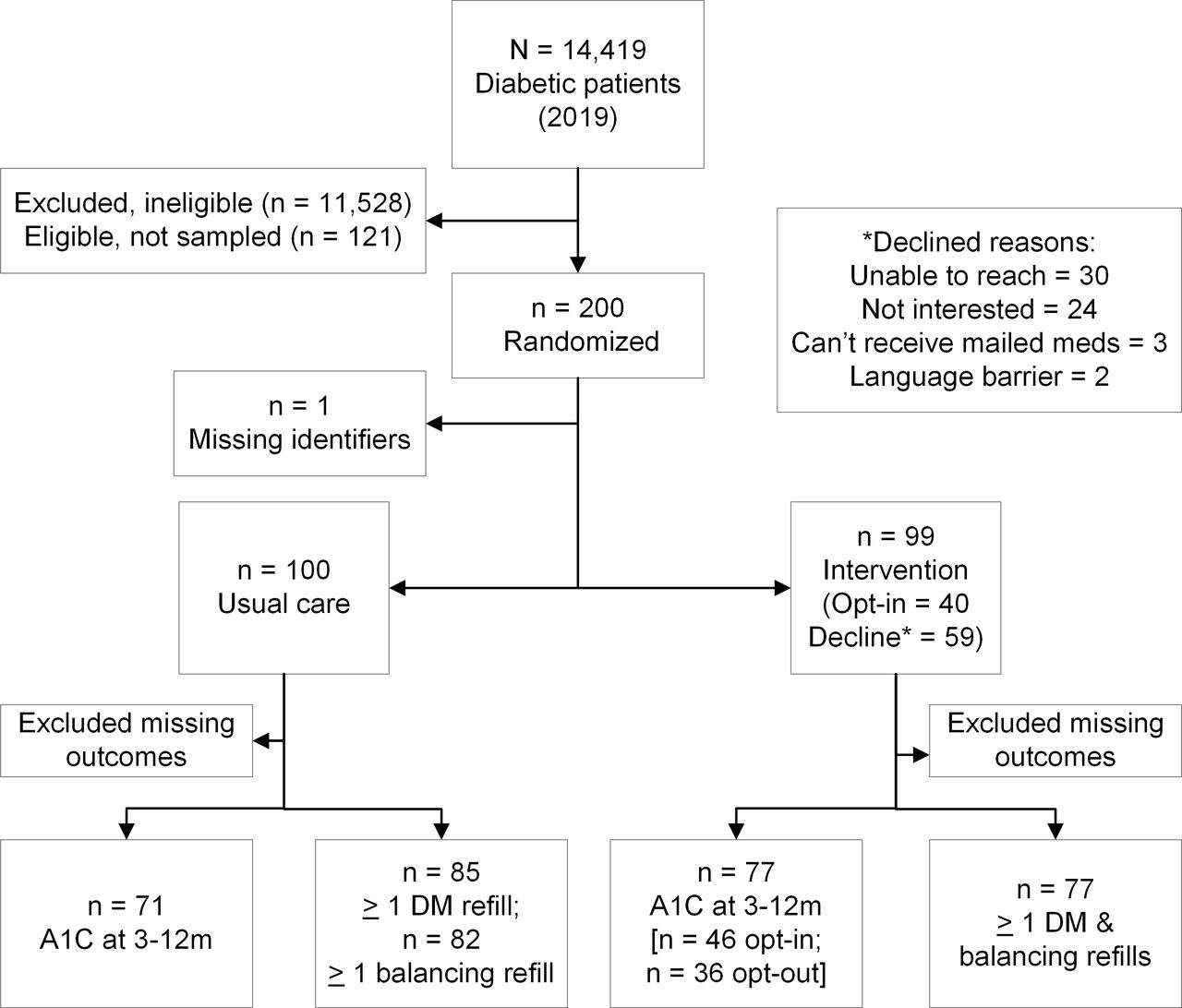
A total of 321 patients were eligible. Based on pharmacy capacity to conduct the process change, a simple random sample of 200 patients was drawn from the 321 eligible patients (n=121 were eligible but not included, figure 1). Patients were allocated 1:1 using a computer-generated random number sequence (non-blinded) to automatic refills or usual care. After randomisation, one patient was dropped due to missing administrative data linkages. Recruitment occurred on a rolling basis for 2 months, then patients received either automatic mailed refills or usual care for at least 6 months.

Patient flow diagram. MPR, medication possession ratio.
Automatic refill patients received a letter explaining the project with consent materials and an invitation to opt-in. VHAPUG pharmacy policy states any process change that impacts patients requires notification and opt-in consent; hence, postrandomisation opt-in was required prior to initiating automatic refills. One week after letters were sent, a team member called automatic refill patients to obtain verbal informed consent. Those reached by phone who opted out were asked why they declined. Automatic refill patients who opted in were automatically mailed refills of oral diabetes medications (detailed below) for a 6-month period. Insulin and injectable diabetes medications were not refilled automatically due to shorter shelf-life, and patients were instructed to continue to self-refill these medications. No outreach was made to usual care patients, who continued to self-initiate all refills.
At 3 months after randomisation, a reminder letter was mailed to all patients without an HgbA1C in the prior 6 months asking them to come in for HgbA1C testing. After 6 months of automatic mailed refills, the intervention period ended and participating patients were instructed to return to self-initiated refills. Patient feedback was collected by phone call at 6 months via a standardised question about patient experience. MPR outcomes were collected after 6 months. HgbA1C outcomes were collected from 3 to 12 months after randomisation to accommodate delays in glycaemic control due to changes in medication adherence (figure 2). Pharmacy effort required to complete the process was monitored weekly.
{kind=link}
{kind=link}
Project timelines. DM, diabetes mellitus.
Included medications and safety monitoring
Medications eligible for automatic refill included select VHAPUG oral diabetes medications (sulfonylureas, thiazolidinediones, biguanides, dipeptidyl peptidase-4 inhibitors and related combinations). We also monitored specific non-diabetic medications as a balancing/reference measure to assess if patients were continuing to self-initiate those medicines, including ACE inhibitors, statins and antiplatelet agents.
Outcomes
Outcomes were selected to establish feasibility of data, measurement processes and workforce capacity. The primary outcome was proportion of patients meeting glycaemic control, defined as mean HgbA1C <8% 3–12 months after automating refills. Secondary outcomes included (a) change in mean HgbA1C (months 3–12) as a continuous measure, (b) change in mean MPR of oral diabetes drugs (months 0–6) to gauge intervention implementation, (c) change in mean MPR of reference drugs (months 0–6), (d) participating patient satisfaction and (e) pharmacy effort.
Data analysis
We assessed quantitative outcomes using logistic and linear multivariable regression models. Given a priori concerns for group imbalance due to postrandomisation opt-in requirements, we adjusted for baseline patient age, race and ethnicity, primary care visit count (3 months prior), service-connected disability rating, community versus hospital primary care clinic affiliation and mean HgbA1C (within 12 months prior). Medication models also controlled for baseline MPR (6 months prior). Outcomes are presented as predicted probabilities using the marginal standardisation method with heteroscedastic cluster robust SEs accounting for repeat measures.31 Patients without a follow-up HgbA1C were dropped from the analysis (online supplemental file 2). Quantitative outcomes were intention to treat, with a per-protocol sensitivity analysis. Randomisation and statistical analysis were done with R and STATA V.14.2.32 33
Supplemental material
Qualitative satisfaction data were extracted from notes taken during follow-up phone calls, and analysed using deductive template analysis within three response categories: positive, neutral or negative satisfaction.34 Two team members independently categorised quotes, reaching consensus.
Results
A total of 199 patients were included and randomised to automatic refills (n=99) or usual care (n=100). Patients were on average 65.7 years old, mostly male (95.5%) and non-Hispanic white (62.8%). While many characteristics were balanced (table 1), the automatic refills group contained more non-white patients (40.4% vs 34.0%), had a higher baseline mean HgbA1C (8.0 vs 7.6) and lower baseline MPR for diabetes drugs (48.7% vs 66.3%). Of patients randomised to automatic refills, 40 opted in (figure 1). Of those randomised to automatic refills who did not receive the intervention, 51% (n=30/59) were excluded because they were not reached for consent and 20% (n=12/59) declined, reporting self-initiated refills was working well for them.
Demographics of patients included in the project (N=199) at baseline
In adjusted intention-to-treat analyses (N=199), there was no difference in the proportion of patients with follow-up HgbA1C <8% between groups (60.8% automatic refills vs 60.5% usual care, p=0.96) or in mean HgbA1C (7.81 for automatic refills vs 7.85 for usual care, p=0.84) (table 2). There was no significant difference in MPR for diabetes drugs (62.2% automatic refills vs 57.1% usual care, p=0.21). However, the MPR for reference medicines was significantly higher in the intervention group (63.9% automatic refills vs 54.5% usual care, p<0.01).
Predicted probability of outcome between automated refills and usual care patients, controlling for baseline differences*
In adjusted per-protocol analysis comparing enrolled patients who received automatic refills to usual care patients, there was no significant difference in glycaemic outcomes at follow-up (table 2). As expected, MPR for diabetes drugs was significantly higher for patients receiving automatic refills than usual care patients (difference=19%, 95% CI 10.1% to 28.1%, p<0.001). However, MPR for non-automatic reference drugs was also 17.2% higher for patients receiving automatic refills compared with usual care patients (95% CI 7.5% to 26.9%, p=0.001).
Qualitative feedback was obtained from 26 patients receiving automatic refills. Most described satisfaction with the process. One participant described how automatic refills were ‘actually quite handy, I didn’t have to do anything, it showed up on time’. Another stated an automatic refill was ‘one less thing I had to be concerned [with], it showed up and I never ran out’. Some felt neutral (‘I didn’t notice a difference; I was ordering my meds as usual’). A few had negative feedback, stating the process ‘overloaded me with diabetic medications’ and ‘it wasn’t established long enough. It would have been better if it was all my medicines’.
Pharmacy staff (two individuals) estimated their combined total time for tracking patients and triggering refills required 60 min weekly.
Discussion
Within this randomised quality improvement pilot project, we found that automatically refilling and mailing oral diabetic medications did not significantly impact glycaemic outcomes for patients with diabetes and prior low medication adherence. However, we did find positive indirect effects from automatic medication refills on patient self-initiated refills of other medications. Furthermore, this project was well received by patient participants and was feasible based on workflows and time required from pharmacy personnel.
There have been a multitude of medication adherence interventions in the literature. Effective interventions have included strategies such as dose simplification, education, reminder systems or financial incentives.5 35 This project was developed to target known individual administrative behavioural barriers to refills (eg, initiating refills, picking up medications at the pharmacy)36 by incorporating principles from behavioural economics9 to implement a system-level redesign to ‘nudge’ patients towards adherence to diabetes medications. This was a novel approach filling a current literature gap by automating and mailing refills of medications for a chronic disease, whereas related interventions to date have included automated reminders, automated refills for pharmacy pick-up or synchronising refills of multiple medications.13–17 Additionally, as context is known to be important for behavioural economic interventions,37 this intervention is novel among refill interventions in its conduct within the integrated VHA. The VHA encompasses a more socioeconomically, racial and ethnically diverse population than non-VHA mail-order programme participants.20 38 39 The VHA is also relatively cost neutral for refills given waived or low-cost copays for most patients; cost is a known barrier to participating in mailed refill programmes outside VHA.40 Beyond the unique intervention and environment for our project, three generalisable lessons based on our findings and implementation process emerged.
First, while we note this was a pilot test, we unexpectedly found a significant improvement in self-initiated refill behaviour for non-automatic, reference medications among automatic refill patients. One explanation is that the mailed arrival of some automated medications may have reminded patients to self-initiate refills of other medications. For health systems considering similar interventions, automating one medication could serve both as a reminder (for non-included medications) and a refill programme—a potential beneficial indirect effect. If scaled across the 120 million plus prescriptions dispensed annually from VHA centralised pharmacies,25 this beneficial indirect effect could have marked effects during future iterations. Given interest in behavioural solutions involving phone or letter outreach for overdue refills,13–16 41 this type of programme presents a novel alternative reminder system.
Second, our project illustrated the importance of tailoring solutions for appropriate patients and adherence barriers. Despite low medication possession history, our project patients mostly had well-controlled diabetes (HgbA1C <8%) prior to the intervention. This may explain why a large proportion of intervention patients (60%) did not opt-in for automatic refills; patients may have felt that their glycaemic control was adequate, and their behaviours were not in need of change. This is supported by the common opt-out reason that the ‘usual system’ was already working. The relatively well-controlled average baseline HgbA1C also likely relates to the lack of improvement in glycaemic control during the study, as these patients may have had a less linear relationship between their medication refill behaviour and glycaemic control. Medication adherence is a complex behaviour, affected by other factors than those from the healthcare system,36 42 and other studies have also shown that improvement in a pharmacy administrative measure of adherence may not translate to improved health outcomes.43 Automatic mailed refills may be more impactful when tailored to patients with excess administrative burden as a refill barrier,44 who may be better represented by having both high HgbA1C and low medication possession history.
Finally, this project was supported by a formal, well-established, collaborative operational research partnership embedded within a learning health systems framework. Specific facultative infrastructure included comprehensive, accessible electronic databases, logistic support (eg, mail systems, phone lines) and operational workflows (eg, pharmacy tracking). The partnership also enabled an interdisciplinary team with involvement of diverse stakeholders across clinical departments, between front-line staff and higher clinical leadership, and between operational personnel and health services researchers. This successful model may provide a blueprint to other organisations seeking to adopt similar partnerships and infrastructure to engage in learning health systems activities.18
Limitations
We note several limitations to this project. As a pilot, we recognise this project was not powered to detect a statistical difference in health outcomes and was not intended primarily to measure the effect of the intervention on glycaemic control. Additionally, we had a lower rate of postrandomisation opt-in to automatic refills than expected. Also, as we were focused on local institutional processes, we did not capture non-VHA prescription behaviour. Finally, we note that our VHA-based lessons may be less generalisable to health systems serving civilian populations or where costs to patients or the health system require different solutions. We note our patients received medications without a copayment, a circumstance that may limit project dissemination to other health systems where copay costs for automailed medications may be more detrimental.
Conclusions
Low patient adherence to chronic disease medications continues to limit the ability of advances in drug therapy to impact health outcomes. Despite initial promising findings from our project, barriers to implementation of automatic mailed medication refills remain, including patient unwillingness or inability to take medications despite presence of medications ‘on-hand’, concerns over medication costs and risk of medication waste or overpossession. Lessons learnt applicable to quality improvement from this randomised pilot test include recognising the potential for beneficial indirect effects from automatic mailed medication refills, the need for careful selection of a target population (ie, patients with worse diabetes control for whom administrative barriers may drive their low medication adherence) and the importance of the contextual setting from a supportive operational research partnership and infrastructure for the implementation and evaluation of future projects.
Data availability statement
Data are available upon reasonable request. Data for this study were collected for local quality improvement efforts at the VHA Puget Sound Health Care System. Consistent with operational, non-research activities conducted by the US Veterans Health Administration, a deidentified limited data set that supports the findings of this study is available from authors upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was deemed non-research quality improvement according to the VHA Puget Sound Institutional Review Board, and therefore exempt from IRB review. We obtained informed consent to participate from all patients who received any project-related process change outside usual care.
Acknowledgments
The authors thank Nicholas Meo, Andrew White and the University of Washington Center for Scholarship in Patient Care and Quality and Safety faculty for their contributions to the initial design of this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Presented at This work was previously presented at the Society for General Internal Medicine Northwest Regional Meeting, 31 January 2019, in Portland, Oregon.
Contributors ALG: writing—original draft (colead), visualisation, writing—review and editing. JG: conceptualisation, methodology, resources, writing—review and editing, visualisation, administration. CO’K: conceptualisation, methodology, investigation, resources, data curation, writing—review and editing, administration. KN, CS: investigation, writing—review and editing, supervision, project administration. CV: conceptualisation, supervision, writing—review and editing. JB: conceptualisation, methodology, resources, project administration, writing—review and editing. AR: writing—review and editing, funding acquisition, supervision. EW: methodology, software, formal analysis, writing—review and editing. LS: guarantorship, conceptualisation, methodology, software, formal analysis, writing—original draft (colead), writing—review and editing (lead), validation, investigation, resources, data curation, visualisation, project administration.
Funding JG, AR, EW and LS were supported by the Primary Care Analytics Team (PCAT), evaluating VHA primary care. PCAT is funded by the VHA Office of Primary Care.
Disclaimer The funders had no influence on the study design, conduct, or evaluation of outcomes, or preparation of the manuscript for publication. The views expressed are those of the authors and do not necessarily reflect the position or policy of the VHA or affiliated institutions.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.