Article Text

Abstract
Background Harmful or fatal errors related to accidental overdose of methotrexate tablets are well documented. In England, the coprescription of 2.5 mg and 10 mg methotrexate tablets is not recommended, because both tablets look similar, and may be confused with each other, leading to a potential overdose of methotrexate. It is recommended that one tablet strength (usually 2.5 mg) is prescribed and dispensed. A recent retrospective cohort study identified that while 97% of patients in England were prescribed only 2.5 mg methotrexate tablets, the prescribing of 10 mg tablets or combinations of 2.5 mg and 10 mg tablets was still common practice in a small number of geographical areas across the country.
Aim and methodology To reduce national variation in the prescription of oral methotrexate 10 mg tablets, for non-cancer treatment, by November 2021. A focused, five-stage quality improvement (QI) intervention was used, providing centralised support to a cohort of high prescribing integrated care systems (ICSs) in England.
Findings 23% (10) of ICSs in England were responsible for 76% of prescribing of methotrexate 10 mg tablets. Eight of these high prescribing ICSs participated in the QI intervention between March and November 2021. During the action period, the high prescribing cohort saw a 54% reduction in the prescribing of methotrexate 10 mg tablets, with seven ICSs seeing reductions of between 41% and 75%, resulting in reduced variation between the high prescribing ICSs and all other ICSs. The intervention was well received by ICSs with all making structural changes to their respective systems so that improvement would be sustained.
Conclusions The success of this project raises several exciting opportunities for further work of this nature, particularly where this is significant variation in practice across the country.
- Patient safety
- Quality improvement
- Medication safety
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
In England, it is recommended that one strength (usually 2.5 mg) of methotrexate tablets is prescribed for non-cancer treatment to reduce the risk of accidental overdose; a recent study identified the coprescription of 2.5 mg and 10 mg tablets was common practice in a small number of areas across the country.
WHAT THIS STUDY ADDS
The use of a data-focused and network-based approach that supported high prescribing systems through the stages of understanding the problem to implementing change was recognised as helping those participating get results, reduce variation and improve safety.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The success of this work shows that this style of approach may be of benefit for others trying to undertake similar national or macro system improvement projects where there is significant variation in practice.
Problem
Harmful or fatal errors related to accidental overdose of methotrexate tablets are well documented.1–3 In England, the coprescription of 2.5 mg and 10 mg methotrexate tablets is not recommended, because both tablets look similar, and may be confused with each other, leading to a potential overdose of methotrexate.1 4 A recent retrospective cohort study identified that while 97% of patients in England were prescribed only 2.5 mg methotrexate tablets, the prescribing of 10 mg tablets or combinations of 2.5 mg and 10 mg tablets was still common practice in a small number of geographical areas across the country.5
The aim of this quality improvement (QI) project was to reduce national variation in the prescription and supply of oral methotrexate 10 mg tablets, for non-cancer treatment, by November 2021.
Background
With more than 1.7 million items issued in England during 2020/2021,6 methotrexate is a commonly prescribed medicine for rheumatoid arthritis, Crohn’s disease, severe psoriasis and some cancers. It is also a high-risk drug, with the combination of a narrow therapeutic index and an unusual weekly dosing regimen predisposing patients to an increased risk of harm from accidental overdose. In 2004, the National Patient Safety Agency (NPSA) issued a national safety alert after 25 patients died and 26 were seriously harmed following accidental overdose of methotrexate tablets during a 10-year period.1 Further cases of accidental overdose prompted a further national safety alert,2 the inclusion of overdose of methotrexate for non-cancer treatment as a national never event7 and more recently updated regulatory measures.8
A range of strategies are in place in England to reduce the risk of accidental overdose that include targeting the manufacture, prescribing and dispensing of methotrexate tablets. When the coprescription of methotrexate 2.5 mg and 10 mg tablets is considered, the British National Formulary states4:
To avoid error with low-dose methotrexate, it is recommended that only one strength of methotrexate tablet (usually 2.5mg) is prescribed and dispensed.
Beyond this and other national prescribing guidance,9 there are no nationally led interventions to reduce the prescribing of 10 mg tablets or combinations of 2.5 mg and 10 mg tablets. Instead, a series of independent local safety initiatives10–13 shared care guidelines dissuading methotrexate 10 mg tablet prescribing14–17 and standard operating procedures18 are in place across some areas of England.
MacKenna et al 5 highlighted the prescribing of both 2.5 mg and 10 mg tablets was common practice with 1689 out of 7349 General Practitioner Surgeries breaching national guidance. Substantial geographical variation existed, with a small number of clinical commissioning groups (CCGs) responsible for high levels of coprescription.
Design
Centrally led five-stage QI intervention focused on providing coaching support to a cohort of high prescribing ICSs in England to reduce variation in methotrexate 10 mg prescribing. This work was led by the English Medication Safety Improvement Programme (MedSIP) team, a team of three pharmacists with training in QI methodology, based at National Health Service (NHS) England.
During the intervention, local oversight of methotrexate prescribing was undertaken by 42 integrated care systems (ICS) each covering an average population size of 1.2 million people. Previously known as Sustainability and Transformation Partnerships (STPs), each ICS was composed of between 2 and 3 CCGs, responsible for commissioning most of the hospital and community NHS services in their local areas. Within each ICS, local prescribing support teams were in place, and the MedSIP team supported these teams during the QI intervention.
The intervention was designed to align with the improvement approach, with five consecutive stages moving from understanding the problem, to testing and implementing change, to focusing on quality control and learning lessons. The five stages are sequentially reported in the strategy and measurement section, including how ICS staff were engaged and supported at each of these points.
Patients and the public were not involved in the design of this QI intervention. This was because the prescription of 2.5 mg methotrexate tablets for non-cancer treatment was already standard national practice, with 98.5% of patients during the time of the QI intervention using only 2.5 mg tablets. Patient engagement instead took place on a patient/clinician basis through clinical consultations with collective feedback collected by participating ICSs. This feedback forms part of the design of this intervention and is incorporated in the balance measures for this QI report.
Strategy and measurement
Identifying and engaging high prescribing ICSs
The aim of this stage was to identify and engage the highest prescribing ICSs in England. Data from OpenPrescribing was used, which uses prescribing data published monthly by the NHS Business Services Authority.19 The MedSIP team used the measure ‘Methotrexate 10 mg tablets by all STPs'20 to identify the top 10 prescribing ICSs in January 2021, by undertaking a Pareto analysis. The top 10 ICSs were contacted and invited to take part in the QI intervention.
Understanding the local problem
The aim of this stage was to support participating ICSs/CCGs to understand what was driving methotrexate 10 mg tablet prescribing and to develop a strategy to tackle this problem. A series of coaching sessions were provided to support:
The use of benchmarkable longitudinal prescribing data.20
The identification of patients currently on methotrexate 10 mg tablets and how prescribing varied geographically.
Collaboration with hospital systems to understand how prescribing took place and where variation existed.
The MedSIP team reviewed and thematically analysed information collated from written reports from the ICS/CCG teams, in addition to verbal feedback collated during the coaching sessions, to identify key findings that came out of this stage of the QI intervention.
Action period
The aim of this stage was for each ICS/CCG to carry out their strategy, using data to help them understand the impact of their changes. ICSs supported clinical staff to identify patients prescribed 10 mg tablets, review the patient’s clinical notes to understand the rationale and then where appropriate invited patients to a consultation and used a shared decision-making approach to switch the patient from 10 mg tablets to 2.5 mg tablets. This meant that there were eight simultaneous but independent QI efforts happening in the eight targeted ICSs, all under the coaching and supervision of the centralised MedSIP team.
Outcome, process and balance measures used during the action period are set out in table 1. For the outcome measure, we used the number of items prescribed for methotrexate 10 mg tablets for the high prescribing cohort versus all other ICSs/CCGs in England. This helped us determine whether the aim of this QI project was achieved, which was to reduce variation in the national prescription of oral methotrexate 10 mg tablets, for non-cancer treatment, by November 2021. For the process measure, we used each ICS’s methotrexate 10 mg tablet prescribing data, as this helped us understand how they each were performing, allowing both the MedSIP and ICS teams adjust their approach to achieve the overall aim of the QI project. For balance measures, we used five separate measures to study unintended consequences. Two measures focused on whether any patient safety incidents had taken place because of patient confusion or administrative errors associated with the intervention. Two measures focused on identifying whether there were any negative or positive patient and staff experiences because of the QI intervention. One final measure focused on detecting any financial repercussions because of the QI intervention.
Outcome, process and balance measures for the action period
The observation period for this QI report was from February 2020 to November 2021, with a baseline period from February 2020 to February 2021 and an intervention period from March 2021 to November 2021.
Longitudinal data were analysed using either line graphs or Shewhart control charts. The line graphs provided a descriptive view of general patterns over time, while the Shewhart control charts enabled the identification of common and special causes of variation in the data. Decision making around control chart selection and the detection of special cause variation followed established rules.21 22 An interrupted time series design was used to distinguish between the baseline and action periods, and centre lines were rephased when statistical changes in a measure were detected. Percentage changes were calculated by comparing an ICS’s baseline mean with its action period mean using standard percent change calculations. Experience data were collected using a qualitative approach, based on Woods et al,23 through a series of sessions with ICS staff.
Quality control
The aim of this stage was to support each ICS to implement changes to their local structures and processes to enable them to hold the gains. This took place between March and November 2021. As part of this process, the MedSIP team shared changes that other ICSs were planning to make and used a MOCHA sustainability planning tool to guide ICS thinking.24 The MedSIP team reviewed, and thematically analysed information collated from written reports and verbal feedback from local ICS teams.
Networking and learning lessons
The aim of this stage was to enable networking between the different ICSs in the high prescribing cohort and the identification of key contextual elements that had contributed to the success of this work and hindered it. A qualitative approach, based on Woods et al,23 was used in these sessions to gather feedback. These sessions took place between October and November 2021 and information generated through these sessions was thematically analysed.
Results
Stage 1: identifying and engaging high prescribing ICSs
In January 2021, 2225 items were prescribed for methotrexate 10 mg tablets, representing 1.5% of all prescriptions for methotrexate tablets. As illustrated in figure 1, 10 ICSs were responsible for 76% of total national prescribing, with ICS 1 responsible for 23%. Beyond these 10 ICSs, prescribing tailed off with the remaining 32 ICSs responsible for 24% of national prescribing. Following engagement with the 10 ICSs, two were unable to participate owing to operational pressures associated with their COVID-19 vaccination programmes. The MedSIP team therefore engaged with the remaining eight ICSs (1–2, 4–9) through stages 2–5 of the QI intervention.

Pareto chart of number of items of methotrexate 10 mg tablets issued per ICS during January 2021. ICS, integrated care systems.
Stage 2: understanding the local problem
Six ICSs decided to take an ICS level approach looking to reduce methotrexate 10 mg prescribing across all CCGs in their area (ICSs 1, 2, 4, 5, 8 and 9) with two choosing to focus directly on specific CCGs in their area (ICSs 6 and 7). Four common issues were identified as contributing to methotrexate 10 mg tablet prescribing:
Prescribing was driven by specific localities (5/8 ICSs).
Prescribing was driven by hospital specialists (2/8 ICSs).
Prescribing was a result of historical practice that had gone unchallenged (8/8 ICSs).
Prescribing was driven by subpopulations of patients unwilling to convert to 2.5 mg tablets owing to increased pill burden (3/8 ICSs).
Action period
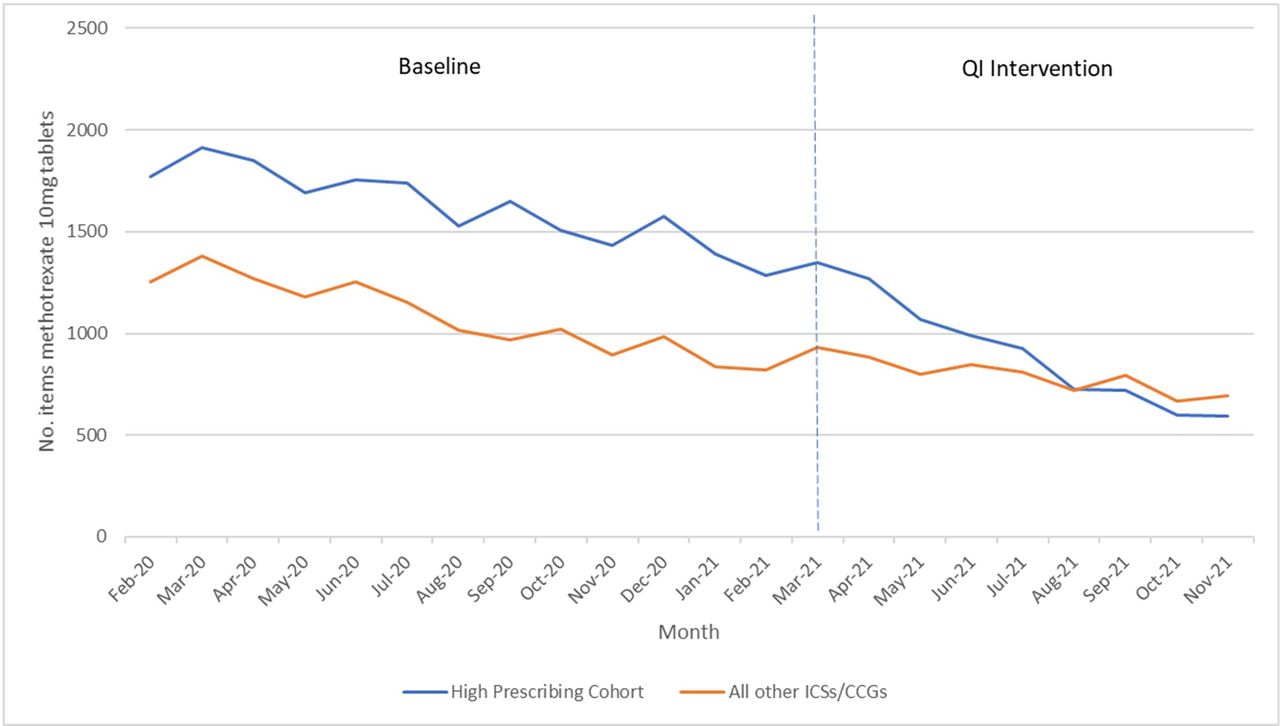
Number of items prescribed for methotrexate 10 mg tablets for high prescribing cohort versus all other ICSs/CCGs in England
Figure 2 shows that before the QI intervention started, a reduction in methotrexate 10 mg tablet prescribing was already taking place, with both the high prescribing cohort and all other ICSs/CCGs reducing at approximately the same pace. During the action period, the pace of reduction for the high prescribing cohort exceeded that of all other ICSs/CCGs. Online supplemental figure 1 shows that special cause variation was evident during both the baseline and action periods for both groups. For the high prescribing cohort, the mean during the action was 660, down from 1438 for the baseline period, a 54% reduction in methotrexate 10 mg tablet prescribing. For the remaining ICSs/CCGs, the mean during the intervention was 717, down from 934 for the baseline period, a 23% reduction.
Supplemental material
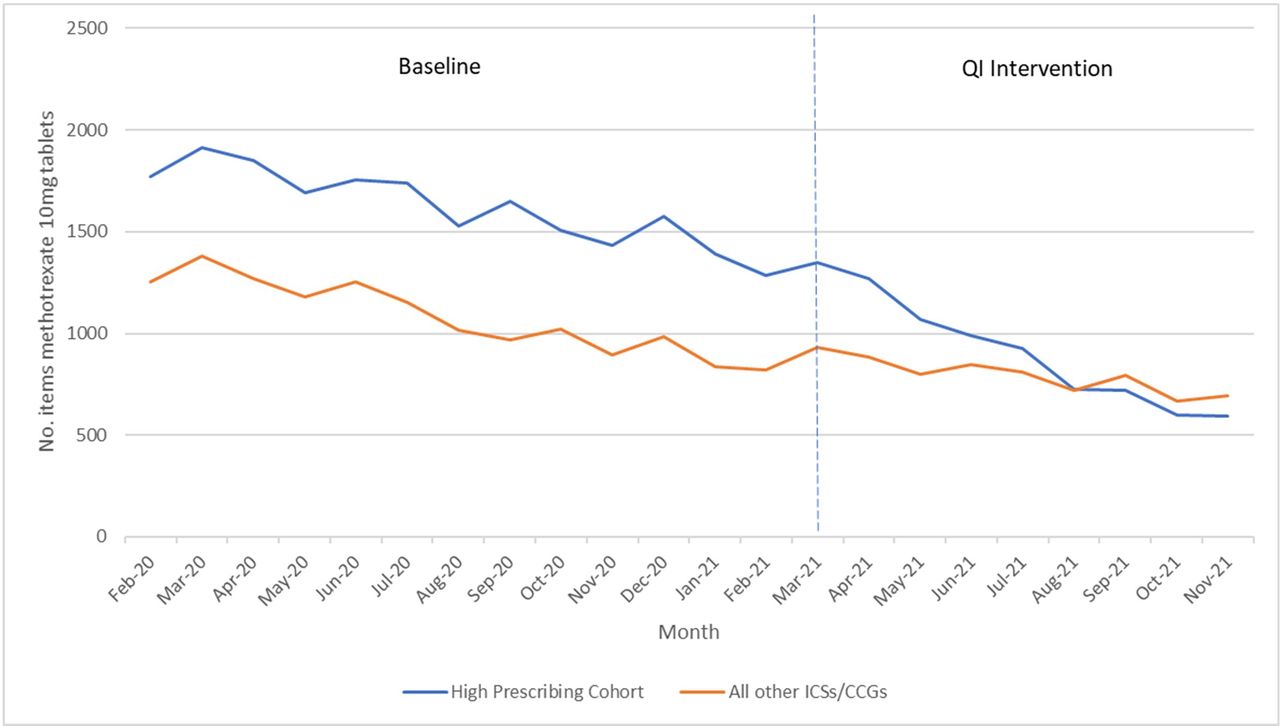
Line graph of methotrexate 10 mg tablet prescribing for high prescribing cohort versus all other ICSs/CCGs. CCGs, clinical commissioning groups; ICSs, integrated care systems.
Process measure: total number of items prescribed for methotrexate 10 mg tablets for each individual ICS/CCG in high prescribing cohort
Figure 3 shows that seven of the eight ICSs (ICS 1, 2 and 4–8) saw special cause variation during the action period with reductions in methotrexate 10 mg prescribing ranging from 41% to 75%. One ICS (9) saw no change. The timing of reductions varied between the ICSs, with four (1, 2, 4 and 5) seeing reductions in the first 3 months of the intervention period and three (6, 7 and 8) seeing later and more rapid change. Figure 3 also shows that not all ICSs/CCGs were seeing reductions in methotrexate 10 mg tablet prescribing during the baseline period. Normal cause variation was present for half the ICSs/CCGs (1, 2, 7 and 8) indicating no significant reductions, with 3 (4, 5 and 6) seeing small reductions during the baseline period. In the case of ICS 9, a reduction of 55% was seen during the baseline period and while no further reductions were seen during the action period, this improvement was sustained.

{kind=link}
{kind=link}
{kind=link}
Methotrexate 10 mg tablet prescribing for individual ICSs/CCGs participating in QI intervention (Individual Moving Range (XmR) control charts).
Balance measure 1: number of patient safety incidents reported to NRLS regarding methotrexate 2.5 mg/10 mg tablet misadministration
There were no patient safety incidents resulting in harm reported to the NRLS during the action period related to methotrexate 2.5 mg/10 mg tablet misadministration.
Balance measure 2: feedback from ICSs on any reported safety issues related to methotrexate 2.5 mg/10 mg tablet misadministration
There was one report of a near hit when a clinician identified that a patient was counselled and switched to methotrexate 2.5 mg, but 10 mg remained on electronic prescribing system, and this was represcribed. There were two reports where patients received a suboptimal dose. In both cases, the prescription was changed from 10 mg to 2.5 mg, but patients went on to take same number of tablets as before, as when on 10 mg tablets. Ineffective patient counselling was identified as the cause of these incidents. All these incidents were immediately share with all ICSs participating in the QI intervention.
Balance measure 3: ICS reported patient experience of QI intervention in high prescribing cohort
In general, the intervention was well received. However, several ICSs identified small populations of patients unwilling to switch from 10 mg to 2.5 mg tablets, owing to increased tablet burden.
Balance measure 4: ICS/CCG reported staff experience of QI intervention in high prescribing cohort
All ICS prescribing support teams provided positive feedback about the QI intervention and the nature in which it was delivered. Direct intervention from the MedSIP team, together with benchmarkable data was particularly helpful in building momentum for change. No feedback was received via ICS staff from clinicians about their experience of carrying out the intervention.
Balance measure 5: total cost of methotrexate tablets for high prescribing cohort
Online supplemental figure 2 shows that normal cause variation was evident during the baseline and action periods for the high prescribing cohort. This indicates that the QI intervention did not have any impact on the financial expenditure of methotrexate tablets.
Quality control
All ICSs/CCGs made changes to their existing structures and processes to ensure that they were able to hold the gains. Seven ICSs created position statements, setting out that 10 mg tablets should not be prescribed. Six ICSs created prescribing alerts on their electronic prescribing systems if the prescriber attempted to prescribe 10 mg tablets. A smaller number of ICSs chose to make methotrexate 10 mg tablets non-formulary for non-cancer use (three ICSs), removed it from the acute Trust hospital prescribing system (one ICS) and asked community pharmacies to store 10 mg tablets in the controlled drug cabinet, separating them from 2.5 mg tablets kept on shelves (one ICS). Several ICSs were planning on introducing standardised methotrexate initiation letters from hospital specialists to GPs stating the dose of methotrexate to be prescribed in multiples of 2.5 mg tablets.
All ICSs opted to continue to use the longitudinal data for the ongoing measurement of methotrexate 10 mg tablet prescribing and agreed oversight would be undertaken by prescribing support teams.
Networking and learning lessons
Contextual elements identified as helping the progress of this work were:
Creating a burning platform: direct intervention from the MedSIP team helped ICSs build momentum for change.
Structured support to understand the problem: coaching from the MedSIP team, together with the use of data was integral to understanding the problem and devising a strategy to reduce prescribing.
Leveraging networks: all ICSs shared the importance of leveraging local networks to enact change.
Systematic approach to improvement: the use of a systematic approach to identify, review and sustain change was critical to the success of this work.
Learning between ICSs: networking sessions between ICSs helped identify barriers and potential solutions to problems.
Contextual elements hindering the progress of this work were:
Lack of national driver around this issue. The historic lack of a central driver had been a barrier to engage and influence prescribers.
COVID-19. This intervention took place during the COVID-19 pandemic and ICSs identified that this may have reduced opportunity for discussions between the patient, GPs and the community pharmacy.
Lessons and limitations
The aim of this QI intervention was to reduce national variation in the prescription of oral methotrexate 10 mg tablets, for non-cancer treatment, by November 2021. Longitudinal data comparing the high prescribing cohort with all other ICSs/CCGs showed that before the QI intervention took place prescribing was already declining with both groups reducing at a similar pace. However, during the action period, the reduction for the high prescribing cohort (54%) exceeded that of the remaining ICSs/CCGs (23%). This increases our degree of belief that some of the reduction seen by the high prescribing cohort was because of the intervention shared in this QI report and not just because of any background reductions that were also taking place.
In the absence of any centrally led interventions to reduce methotrexate 10 mg tablet prescribing since the publication of the NPSA patient safety alerts in 2004 and 2006,1 2 the background reduction in methotrexate prescribing can be attributed to the cumulative impact of national prescribing guidance and local safety initiatives described in the background of this report.4 8–18 Nevertheless, as highlighted in the Pareto analysis, prescribing levels of methotrexate 10 mg tablets varied substantially across England. Ten ICSs were responsible for 76% of prescribing during the baseline period, painting a similar picture to that identified by MacKenna et al.5 A targeted approach, focusing on reducing variation, was the best use of resources, minimising opportunity costs for most ICSs.
For the eight high prescribing ICSs/CCGs participating in this initiative, the intervention was well received, with positive feedback from those involved. ICS prescribing support teams reported the centrally delivered nature of the intervention enabled the creation of a burning platform, where this had previously been lacking. This together with a data focused, systematic, network-based approach helped create a context that made this work thrive.
During the action period, seven of the eight ICSs saw special cause variation with reductions in methotrexate 10 mg prescribing ranging from 41% to 75%. The timing of reductions varied between the ICSs, with four (ICS 1–5) seeing reductions starting earlier during the QI intervention and three (ICS 6–8) seeing reductions later. We believe that the reason for these differences can be attributed to two causes. The first relates to the sequencing of engagement between the MedSIP team and high prescribing ICSs, with some receiving support before others. ICSs 1–5 were the first to connect with the MedSIP team and start working on this issue, with ICSs 2, 4 and 5 receiving coaching sessions first. ICSs 6–8 did not start working on this issue until approximately 1.5 months after ICS 1–5. A second cause related to the ICS’s pre-existing knowledge of this issue. As the highest prescribers of methotrexate 10 mg tablets in England, we found ICSs 1–5 already had a high level of understanding about the issue and were able to develop and enact their strategies quickly. In the case of ICSs 6–8, they needed longer to understand the problem before they could proceed into action. ICS 9 did not see change during the action period, and this may have been because they had already seen substantial reductions during the baseline period and there was a reluctance to restart this work again owing to change fatigue.
While no patient safety incidents resulting in harm were reported via the NRLS, the MedSIP team was made aware of one near hit and two incidents where patients took a suboptimal dose. In the case of the two incidents, the cause appeared to be ineffective counselling. Information about all three incidents was promptly shared with all participating ICSs, and prescribing teams were encouraged to follow-up patients that had a change in tablet strength. In general, the QI intervention was well received by patients, although several ICSs did identify small populations of patients that were unwilling to change from 10 mg to 2.5 mg tablets owing to increased pill burden. Financial analysis indicated that the QI intervention had no impact on methotrexate expenditure.
A substantial part of this QI intervention focused on quality control by introducing changes to local systems so that improvement was sustained. A variety of changes were implemented that in most cases responded to the local causes of methotrexate 10 mg prescribing. The ICSs shared the networking sessions provided by the MedSIP team were a particularly useful way to share these change ideas. In several instances, ICSs adopted other ICSs ideas and implemented them locally. Such instances of sharing, testing and implementing improvement ideas are a key part of national campaigns.
There are four limitations associated with this report that merit further discussion. First, while we used nationally recognised longitudinal data to understand the impact of the QI intervention, we did not use statistical techniques to control for confounding factors. These could have included the National Pharmacy Association’s Methotrexate Standard Operating Procedure, published February 2021, that may have influenced pharmacies during the intervention period18 and the impact of COVID-19 on methotrexate prescribing and on mortality among those on methotrexate. While an inability to control background confounding factors is a common weakness in QI projects, we increased our degree of belief around the QI intervention through observing similar results across seven of the eight ICSs/CCGs participating in this initiative, listening to feedback from those involved in the change and seeing a greater reduction in methotrexate prescribing in the high prescribing cohort compared with all other ICSs/CCGs.
A second limitation relates to the lack of outcome measures looking at harm to patients from methotrexate 2.5 mg and 10 mg misadministration. While there are a range of national safety alerts, prescribing guidance and standard operating procedures in place to reduce accidental overdose of methotrexate tablets, the NHS does not reliably measure the prevalence of methotrexate overdose on admission into its hospital systems. This forced us to use prescribing levels as a surrogate measure for harm. We did, however, include patient safety incidents reported via the NRLS and ICSs as a balance measure. Those considering future work on this topic may also consider obtaining data from the National Poisons Information Service.
A third limitation relates to our dependence on voluntary reporting rather than systematic identification for three of the five balance measures. In the case of ICS reported patient safety incidents, we attempted to mitigate for this by using nationally collated and managed NRLS data. However, in the case of patients and staff experience, we could have considered more systematic surveys and questionnaires for those affected.
A final limitation relates to this QI report’s generalisability. While there clearly may be other opportunities to replicate this style of approach, there may only be a limited number of national opportunities where there is considerable variation, a manageable patient population affected by the change and a discrete and simple intervention that could easily be replicated with a low impact on NHS resources.
Conclusion
In England, the coprescription of 2.5 mg and 10 mg methotrexate tablets is not recommended, because both tablets look similar and may be confused with each other, leading to a potential overdose of methotrexate. The aim of this QI project was to reduce national variation in the prescription of oral methotrexate 10 mg tablets, for non-cancer treatment, by November 2021. Despite reductions in methotrexate 10 mg prescribing taking place across England, variation in practice still existed with 23% of ICSs responsible for 76% of prescribing. A focused five-stage QI intervention was used to reduce national variation by providing centralised support to a cohort of eight high prescribing ICSs. During the QI intervention, the high prescribing cohort saw a 54% reduction in the prescribing of methotrexate 10 mg tablets, with seven ICSs seeing reductions of between 41% and 75%, resulting in reduced variation between the high prescribing ICSs and all other ICSs. The intervention was well received by ICSs with all making changes to their systems so that improvement would be sustained. The success of this project raises several exciting opportunities for further work of this nature, particularly where there is variation in practice across the country.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but the National Medicines Safety Improvement Board exempted this study. Participants gave informed consent to switch their methotrexate tablet strength from 10mg to 2.5mg
Acknowledgments
The authors would like to acknowledge and thank the prescribing support teams from each of the integrated care systems (ICSs) involved in this quality improvement (QI) intervention.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @JInnesMPharm, @PharmSafe, @rlloyd66
Contributors JI led the improvement project, the writing of this QI report and is acting as guarantor for this report . TJ attended some of the coaching sessions, provided input into the overall work and contributed to the writing of the QI report. RD attended some of the coaching sessions, provided input into the overall work and contributed to the writing of the QI report. RL provided specific input into the use of data for improvement and analysis in addition to contributing to the writing of the QI report.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.