Article Text

Abstract
Background Long-term care (LTC) residents frequently experience transitions in the location of more advanced care delivery, including receiving emergency department (ED) care. In this proof-of-concept study, we aimed to determine if we could identify measures in quality of care across transitions from LTC to the ED, via emergency medical services and back, by applying Institute of Medicine (IOM) Quality of Care Domains to an existing dataset.
Methods In the Older Persons’ Transitions in Care (OPTIC) study, we collected information on residents’ transitions in two Western Canadian cities. We applied the IOM’s Quality of Care Domains to the OPTIC data to create binary measures of transition quality. We report the median (MED) per cent and IQR of measures met within each domain of quality.
Results We tracked 637 transitions over a 12-month period, with data collected from each setting. We developed 19 safety measures, 20 measures of resident-centred care, 3 measures of timely care and 5 measures of effective care. We were unable to develop measures for equitable care at an individual transfer level. Domain scores varied across individual transitions, with the highest scores in safety (MED 79%, IQR: 63–95), efficiency (66%; IQR: 66–99), and resident-centred (45%; IQR: 25–65), followed by effectiveness (36%; IQR: 16–56), and timeliness (0%; IQR: 0–50).
Conclusions Our results show variation in scores across the domains of quality suggesting that it is possible to track quality of transitions for individuals across all settings, and not only within settings. We recommend that future work in tracking quality of care be performed at several levels (LTC, region, health authority, province). Such tracking is necessary to evaluate and improve overall quality of care.
- transitions in care
- emergency department
- nursing homes
- quality measurement
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. Data requests should be directed to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known on this topic?
Quality measures for transitions in care for older persons exist specific to single care settings; however, few quality measures have been developed for monitoring emergency transitions across care settings using established methods.
What this study adds?
This is the first study to derive measures for quality of care for the whole transition process from long-term care to the emergency department and back using primary data. We developed 49 quality measures to assess quality domains of safety, timeliness, efficiency, effectiveness and resident-centred care during these emergency transitions.
How this study might affect research, practice or policy?
This preliminary suite of quality measures for older persons’ transitions from long-term care to emergency departments can be used to assess variation in quality domains during emergency transitions from long-term care facilities. Quality measures can be expanded on and adapted for other jurisdictions in future research.
Introduction
Healthcare service delivery for Canada’s vulnerable older population occurs in various settings and involves diverse groups of health providers, professions and services. When the health status and care needs of older persons (>65 years of age) residing in long-term care (LTC) settings change, they may require transfer from LTC to the emergency department (ED). These transitions present risks of adverse events, and quality of care concerns are pervasive throughout the transition process, making the events during this period a distinct and important area for investigation.1–4 Many residents in LTC have cognitive impairment including dementia, which can create challenges for residents to communicate their preferences and concerns regarding their care.5–7 Measures of quality are essential for monitoring quality of client care and elucidating potential quality concerns.8–11 Although some quality indicators for transitions in care for older persons are specific to acute care settings, few quality measures have been developed for monitoring transitions across care settings.12 Generally, quality indicators are developed for specific care settings, where measures are typically determined, tracked, interpreted and applied by the same stakeholders.13 Furthermore, despite the importance of developing quality indicators using primary data collection, many quality measures related to transitions in care are based only on expert consensus and selected due to measurement ease rather than clinical importance.14–17 Therefore, rigorous quality indicator development for transitions across various healthcare settings is particularly challenging. Determining measures that (1) focus on older persons’ transitions in care, (2) reflect accepted domains of quality and (3) adhere to established quality indicator development methods is integral to the identification of areas of concern and modifiable practices for improvement.13 18 19
The Older Persons’ Transitions in Care (OPTIC) Framework was developed to explore (or map) the process of care transitions from LTC to ED and back,20 21 We further used the Institute of Medicine (IOM) Quality of Care Domains which include: patient-centred (hereafter referred to as resident-centred to reflect the LTC context), effectiveness, efficiency, safety, timeliness and equity.22 We used these two frameworks to identify and propose system and process improvements that addressed several of these six elements of a quality healthcare system during a transition from LTC to the ED and back. Specifically, the goals of this project were to:
Identify quality measures for transitions from LTC to the ED and back that could be captured within a robust multisetting dataset and categorised based on the IOM Quality of Care Domains.
Examine variation in quality scores within IOM Quality of Care Domains, (A) by transition care settings and (B) stratified by province.
Although the data for this study were collected in 2011–2012, to our knowledge, this is the only study that tracked individual LTC residents from LTC to the ED and back using primary data collection. The call to improve the quality of ED transitions for older persons is long-standing,23 and little progress has been made on the development of formal guidelines, geriatric emergency education and quality measures in this area24–26
Methods
Overview
In this manuscript, we report analysis of efforts to capture quality measures within a comprehensive multisetting dataset, and to determine variation in care quality across settings. Important aspects of quality of care and measures related to older persons’ transitions were identified through systematic literature review and previous research conducted by the Older Persons’ Transitions in Care (OPTIC) team.12 21 Data for this analysis came from an observational, mixed-methods study, in which residents >65 years of age were tracked during acute care transitions from their LTC facility to participating EDs, and back, using a Transitions Tracking Tool (T3) developed by the research team.20 21 Data were collected on LTC residents’ transitions in the Canadian cities of Edmonton, AB (2011 population ~1 159 869)27 and Kelowna, BC (2011 population ~117 315)28 ; both centres were large regional hubs for ED care. We are not aware of any comparable dataset involving long term care and ED settings. Detailed methods for this study are already published.29
Setting
All existing LTC facilities, paramedic services and the most active ED in each of these Canadian cities consented to participate in the study. All 13 LTC facilities in Kelowna and 25 of 37 (67.5%) in Edmonton participated. The Alberta Health Services emergency medical services (EMS) participated in Edmonton. The BC Ambulance Service in Kelowna declined to participate.
Data collection
Trained research assistants (RAs) identified all resident transitions from participating LTC facilities and EDs using ED medical records. RAs collected medical record data across settings for all transitions. LTC healthcare providers were contacted to identify changes in resident condition after emergency transition.
Data sources
Trained RAs collected data directly from resident charts or by administering a questionnaire to clinicians who participated in a resident’s transition, using the piloted T3.18 29 The OPTIC dataset includes over 800 data points collected in 2011 and 2012, describing 637 transitions in care.
Quality measure identification and development
Statistical analyses were conducted using IBM SPSS Amos Statistics V.26 (SPSS). Measures were created with binary outcomes, where a positive outcome was coded as one and a failure to meet the indicator (ie, the healthcare provider did not complete or document the action) was coded as zero. The number and proportion of transitions that met each measure within each domain was calculated. One exception was employed for the resident-centred measure of ‘who made the decision to transfer.’ In this case, we scored results on a scale as follows: 0=other/unknown, .2=resident or family caregiver, 0.4=licensed nurse practitioner, 0.6=registered nurse, 0.8=physician or nurse practitioner by phone, 1.0=physician or nurse practitioner in person. In this context, we deemed a score closer to 1.0 as a more optimal outcome, because we ordered categories from the least responsible caregiver to the most responsible healthcare professional making the decision to transfer. In the best care scenario (score of 1.0), that decision was made following an in-person assessment by a physician or nurse practitioner.
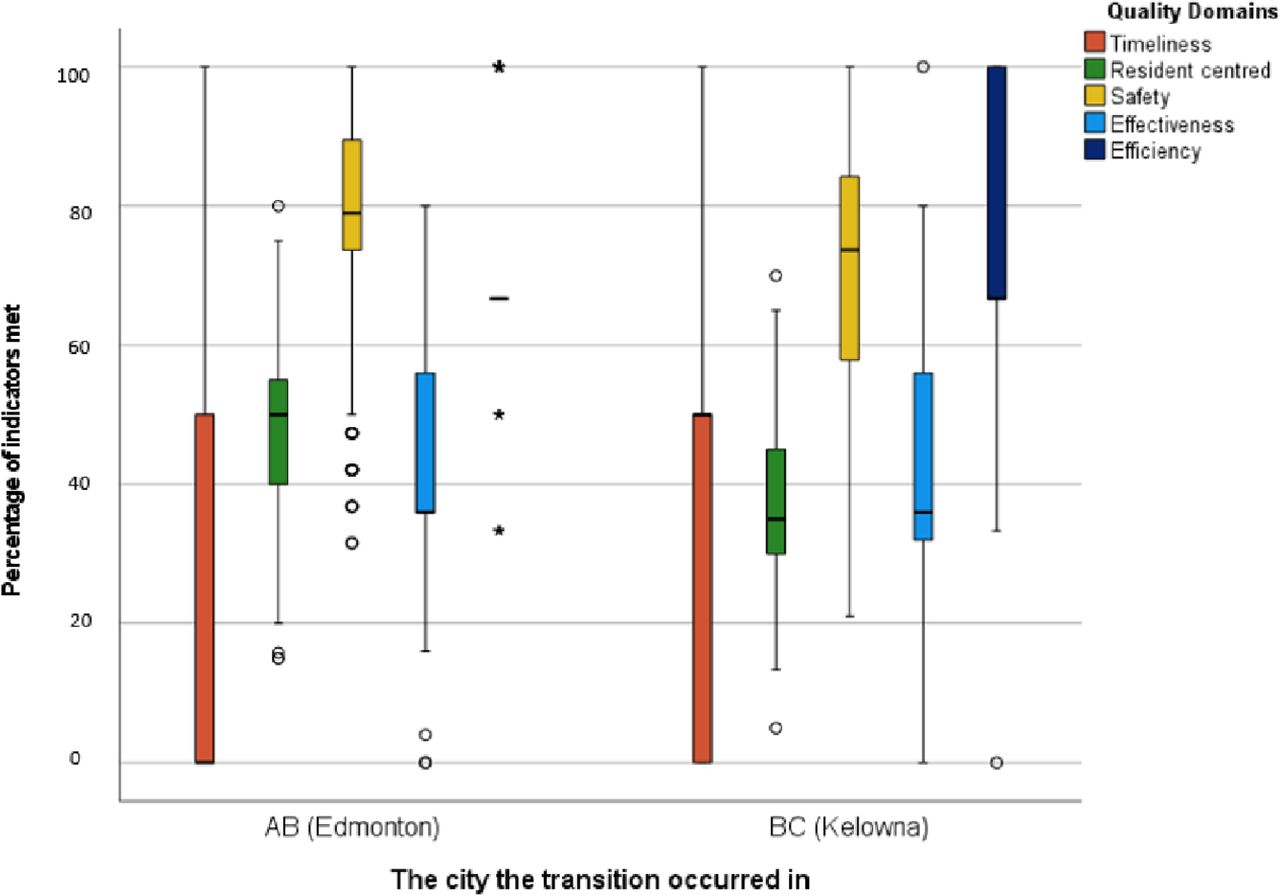
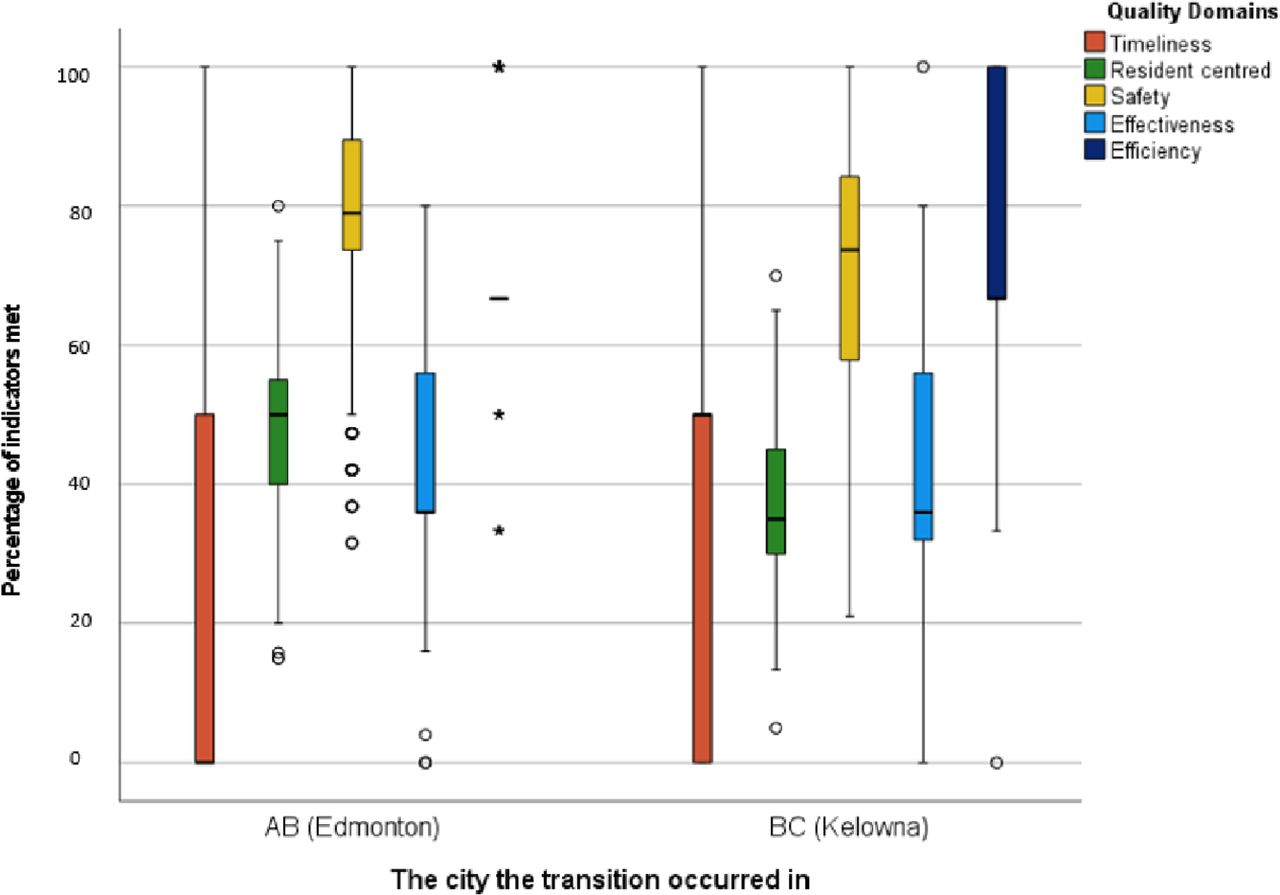
Potential measures of quality of care were categorised according to the IOM domains of quality of care by research team members with clinical experience (ie, physicians and nurses with previous experience in the ED or LTC). Results of a later Delphi process on quality indicators for older persons’ transitions across the care continuum (which included older persons, researchers and clinicians from various healthcare settings) were reviewed to validate the selection of appropriate and relevant measures.12 To determine total domain scores, we summed the number of indicators each transition met within a domain and divided this sum by the total number of indicators within that domain (figure 1). Indicators that related to EMS return trips and LTC on return were not applied to transitions during which the resident died during transition (N=63).30 A timeliness measure related to ED length of stay was not applied to seven of these cases where residents died within the ED.
{kind=link}
Variation in percentage of indicators met by all transitions by domain. AB, Alberta; BC, British Columbia.
Pragmatic decisions through team deliberation and consensus were made to exclude measures where there was a large amount of missing data, or a lack of variation within the measure outcomes. When research staff were unable to obtain data, the case was were excluded for that measure, as we could not determine that reporting on that indicator did or did not occur. These cases were not counted as valid cases for relevant variables. However, if medical records were accessed and nothing was documented, these responses were recorded as 0, or failure to meet the measure. We adopted the principle that if an activity was not recorded, healthcare providers had likely failed to complete the activity in a way that could improve the quality of the resident’s transition (which would require documentation of the activity for reference by the next care provider). We excluded measures with greater than 10% missing data,31 with the exception of some timeliness measures. A higher proportion of missing data was accepted for the timeliness domain, as the need to use two time points to compute measures led to higher missing rates in this domain than in others. A proportion of safety measures relied on clinicians’ reports regarding whether sufficient communication was provided to them by the previous formal caregiver.
Patient and public involvement
Patients and the public were not involved in this study.
Results
Resident sample
A total of 637 transitions were tracked in this study, of which 385 (60.4%) involved female residents. The mean age of residents was 84.3 years (SD=7.7). All transitions included residents with pre-existing diagnoses (eg, dementia, diabetes) with a mean of 8.17 (SD 3.3) per resident. Common functional limitations of residents included impairments in activities of daily living (78.3%), mobility (72%), vision (61%) and moderate to advanced dementia (23.2%). Individual residents had a mean of 3.86 (SD=1.5) selected possible limitations. In 386 transitions residents were not their own decision-makers, and of these, 234 (60.6%) residents also had some degree of dementia (AB=53.5%, BC=73.2 %). Use of advance directives varied by province (AB=87.2%, BC=28.0%). Sixty-three residents died in ED or in hospital, and the quality of their care transitions were measurable only on the transition to ED. See table 1 for resident demographics.
Characteristics LTC residents for all transitions
Quality measure results
We initially developed 33 measures pertaining to safety, 20 for resident-centred care, 8 for effective care and 4 for timely care and 4 for efficient care. As we focused on quality within individual transitions and some resident demographic details were unavailable (eg, race, Indigenous status, socioeconomic status), no measures were identified for equity. Twelve communication specific safety measures, an additional two safety measures, two timeliness measures, two measures of effective care and one measure of efficient care were excluded due to having greater than 10% missing data (see table 2).
Measures excluded due to excessive missing data (percentage missing)
The safety indicators regarding the sufficiency of information at each transition setting except for LTC1 (n=12) had greater than 10% missing data, ranging from 47% to 79% missing data, and thus were excluded.
Following exclusions, we retained a final set of 19 safety measures, 20 measures of resident-centred care, 5 measures of effective care, 3 measure of efficient care and 2 measures of timely care (see table 3). Valid cases for each indicator vary based on whether a resident died in the ED or in hospital, and if research staff were unable to retrieve the relevant document. Total domain scores, for all included valid cases, varied, with the highest scores in the safety domain (MED 79%, IQR: 63–95), efficiency (66%; IQR: 66–99) and resident-centred (45%; IQR: 25–65), followed by effectiveness (36%; IQR: 16–56) and timeliness (0%; IQR: 0–50). See figure 1 for differences in domain scores between Edmonton and Kelowna.
Measures retained and used to calculate domain scores, showing number and percent of transitions meeting each indicator using valid cases (n cases that met measure criteria/valid n, percentage of valid cases met)
Discussion
To our knowledge, this is the first study to derive measures for quality of care for the whole transition process from LTC to the ED and back using primary data. Our results demonstrate that it is possible to measure care in accordance with accepted IOM quality of care domains and across the entire transition. Measurement of quality across a transition is a resident-centred approach, as from the resident’s perspective engaging the health system for a particular health concern may be considered a single episode of care.
We were able to generate clinically meaningful and regularly recorded measures that were primarily in the domains of safety and resident-centred. This is promising, as the literature contains a paucity of established safety quality indicators for provision of care for older persons.32 Our results for measures such as having ‘a medication list available’ highlight areas for further investigation. Medication lists in this study were available in 83% and 84% of cases in the sending LTC facility and during EMS transfer, respectively; however, this decreased to 60%, 46% and 43% throughout the rest of the transition. Although insufficient reporting from LTC settings has been previously identified as a primary source of documentation issues during emergency transitions for older adults, our results instead raise questions about how this information was handed-off on arrival at the ED or accessed by ED clinicians.33–36 Internal or public reporting of this indicator across all involved care settings can support efforts to ensure this quality measure is met. Public or internal reporting may trigger investigation into various reasons for discrepancies in the reporting and administration of medication for older persons, including: the number of medications a person is on, social support from family members and/or a focus on physical assessments without an integrated evaluation of medications in acute care settings.37
Safety measure results in this study also highlight insufficient reporting back to the LTC facility, particularly related to ED summaries not being provided to LTC facilities on discharge from the ED. Hospital-based reporting of such quality metrics could be used to improve care in the future. Although the reported reason for transfer from LTC and EMS was documented in most cases, our research indicates that the reported reason for transition across care settings is inconsistent, or documented in inconsistent places.21 Developing measures that move toward capturing not only whether these types of documentation practices are completed, but whether they are done consistently and in line with current best practices, is warranted. In this study, we used an ‘all or none’ approach (measures were either met or unmet) that equally-weighted existing measures across all eligible transitions within each domain. Equal weighting is recommended unless alternative weightings are theoretically justified.38 However, expert-, opportunity- or numerator-based weighting should be considered in future research and practice depending on the outcome of interest and purpose of obtaining quality scores (eg, numerator-based weightings are more useful when wanting to focus on the prevalence of adverse events at a hospital level).38
Few measures were identified, conceptually agreed on by the research team members and operationalised related to efficiency, effectiveness and timeliness of older persons’ emergency transitions from LTC. Our lack of developed and meaningful efficiency measures echoes long-standing challenges in this area. Efficiency measures such as type of vehicle used on transit to the ED (an ambulance was considered ideal) and number of transport personnel (two was ideal) had little variation in this context, likely due to established structures and policies prohibiting alternative practices. Furthermore, these measures could not be meaningfully applied to the return trip from the ED, as we were not able to determine which type of transport or number of personnel should be most efficient as we did not know the type of care residents needed for the return trip to the LTC facility. For example, a patient sustaining a scalp laceration following a fall should be transported to the ED by EMS; however, following a negative CT scan of the head and laceration repair, that same patient may be most efficiently transported by back to the LTC residence by private vehicle.
Measures with no variation are determined by longstanding organisational structures and policy may not be useful for quality improvement effort in specific contexts. There is a lack of rigorously evaluated efficiency measures for quality management in healthcare in general, and providers and stakeholders often misidentify cost and timeliness measures as efficiency measures.39 Previously identified ‘efficiency’ measures for older persons, and feasibly captured in administrative databases, include: total time in the ED, percentage of hospital emergency transitions that could have been managed in LTC or other settings and structural measures such as the availability of diagnostic testing.12 To develop efficiency measures based on IOM definitions, clear and well-communicated expectations about which inputs are minimally required to effectively provide care for certain conditions and populations would be necessary.22 This would support a focus on reducing waste or improving outcomes without additional labour or supplies, rather than simply using fewer resources.
Quality measures should be used in critical consideration of each other, so that gains in one area are not sought at the expense of other areas. For example, efficiency should not be sought at the expense of safe and effective care.40 41 This applies to quality domains, and the level of data used for quality indicator development. While system-level indicators may illuminate that systemic issues exist, more granular level data can be used to support constructive and context-specific approaches to improving clinical practices. The use of multilevel measures (eg, system, facility, personnel and individual patient level measures) is necessary for evidence informed guideline development and comprehensive reform within and across healthcare settings.26 42–44
Measuring equity when examining an individual transition was not feasible for a variety of reasons. Assessing equity would require analysis of groups of residents and a determination of whether different groups (eg, persons with and without dementia) received the same quality of transitional care using measures for the other five domains. Most importantly, some resident demographic details were unavailable (eg, gender identity, indigenous status, socioeconomic status). Moreover, we propose that equity measures should examine population groups across a data set and in relation to other domains of quality. The measures we developed could be the basis for a future equity-focused analysis. In future research, equity analysis could be conducted to examine whether quality measures we identified for other domains are impacted by resident demographics. Specifically, we must identify the ways that intersecting aspects of diversity (eg, sex, race, and disease status) could influence care.45 For instance, care experienced during emergency transition from LTC by Indigenous persons may differ from non-indigenous individuals, or care experienced by women may differ from that experienced by men. Furthermore, more research is warranted to examine suboptimal care for lesbian, gay, bisexual, transgender, queer and two-spirit residents experiencing transitions in care, older persons with HIV, and visible minorities and Indigenous residents presenting to the ED to rigorously develop equity measures for transitions in care.45 46 Equity can also be considered through risk-adjusted measures; however, this can only statistically control for the potential effects of health inequities and is not the same as developing measures that intentionally compare groups based on inequities.32
Many timeliness measures must be derived from multiple time points, resulting in higher missing cases for the computed variables. For this proof of concept study, we accepted higher missing rates (>10%) given this consideration. Collecting these data elements in electronic health records through electronic time stamps will reduce missing data while supporting data quality. The increasing adoption of electronic medical records (EMR) suggests that such quality metrics will be more easily assessed in the future. Issues meeting timeliness scores may point to larger systemic issues related to availability of ambulances, staff, ED beds or issues of ageism.12 32 42 A recent study demonstrated that a specialised protocol to triage older persons in the ED significantly reduces time to physician assessment, as well as overall ED length of stay.47 This is further supported in other research that suggests triage processes may not address the special care needs of older persons in the ED.48 Further investigation into these types of interventions could support changes in practice guidelines and the development of new quality measures, such as a structural measure for the presence of a geriatric triage protocol. Timeliness scores such as response transport times are often the focus for EMS care; however, extant literature supports that multilevel measures (around oversight/governance, EMS agencies, EMS personnel and patients) for processes, structures and outcomes are needed to advance quality management for this setting in particular.
Finally, although necessary for initial development and testing of quality measures, we would not recommend that health systems rely on survey data collection for judging the quality of particular care episodes (eg, transitions in care) as part of usual operations. Integrating measures into standardised electronic documentation will allow for feasible and reliable capture of data,49 50 while also mitigating the effects of clinician or resident difficulties with recall51 and other reasons for survey non-response (eg, respondent burden, resident deceased, clinicians choosing not to respond to surveys, failures to contact clinicians for data collection). Ensuring effective systems for capturing data for quality measures will allow for future work at a variety of levels (LTC facility, region, health authority, province). Such tracking is necessary to evaluate and improve overall quality of care. Ultimately, this suite of theory- and evidence-informed quality measures should be expanded on using established quality measure development guidelines and stakeholder engagement.26 Residents, family members and stakeholders from all transition settings should be engaged in research processes to develop, pilot test and, importantly, agree on the interpretation of, quality measures for quality improvement practices. Measures should be developed with the intention that they be collected through standardised electronic documentation and be tested to examine their effects, or combination of effects, on particular outcomes of interest during transitions in care for older persons (eg, resident satisfaction, prevalence of adverse events).
Strengths and limitations
This study has several limitations that need to be considered. First this study was intended to demonstrate proof of concept for measuring quality across a transition process, so we have not tested whether these measures correlate with resident outcomes such as mortality, nor have we tested for relationships among the measures. Second, the study was conducted in two Canadian cities, so the generalisability to other jurisdictions and non-publicly funded health systems remains to be seen. Some quality measures, such as Canadian Triage Acuity Scale scores, may not appear to be clinically meaningful in some jurisdictions; however, multilevel triage scoring is universal in EDs in most high-income countries where these transfers largely occur, and would not invalidate these results. Third, despite concerted efforts to collect all necessary data points, missing data were common as neither site employed an EMR. A repeat of the study may be fruitful once EMRs are more widely available. Finally, the data were collected several years ago and processes of care change regularly; however, we do not feel that the timing of the data collection invalidates the findings. Advancement in quality measure development for older persons’ transitions in care is still novel and in line with current literature,26 in part because to our knowledge, this is the only study that collected data over the entire transition process from LTC to the ED and back.
Notwithstanding these concerns, this study has many strengths. First, this study used robust primary data to develop and determine variation and clinical importance of quality measures based on a theoretical framework of the transition process. Second, to our knowledge, this is the first study that collected data on residents of LTC over the whole transition process from LTC to the ED and back via EMS. Finally, we included data from a relatively large sample, collected through multiple strategies in two jurisdictions. Despite the findings being limited to jurisdictions, we included quality measures identified as important to transitions in care for older persons through a systematic review of published international literature.26
Conclusions
Despite the complexities involved, our results demonstrate that transitional quality of care, can be measured and that there is variation among domain scores. These findings suggest that it is possible to track quality of care across all settings involved in a transition, and not only within settings. Rigorously developed measures for efficiency, effectiveness and equity are critically needed, analysed using data sourced from clinical health records augmented by healthcare provider knowledge of the resident as needed. We recommend that future work in quality tracking be performed at different system levels (LTC, region, health authority, province/state). Comprehensive tracking across domains will be helpful in evaluating complex interventions, and in detecting unexpected consequences of such interventions.
Data availability statement
Data are available on reasonable request. Data are available on reasonable request. Data requests should be directed to the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
University of Alberta Health Research Ethics Board (HREB B: Pro00010666; Pro00017240). Interior Health Research Office and Research Ethics (UBCO BREB: 2010-017). University of British Columbia Okanagan Behavioural Research Ethics Board (UBCO BREB: H10-00127).
Acknowledgments
This work was supported by the Canadian Institute of Health Research (CIHR PHE (101863)), the Michael Smith Foundation for Health Research (MSFHR), Alberta Foundation of Medical Research (AHFMR), Alberta Health Services (AHS), Interior Health Authority, Kelowna, British Columbia (IHA). A partnership made possible by the Partnership for Health Systems Improvement Program offered by the Canadian Institutes of Health Research. We also acknowledge funding from the following organisations: University of Alberta Hospital Foundation; and the BC Network for Aging Research (BCNAR). We are grateful for the active partnership and full contribution of the research team of decision-makers and researchers. We would like to thank Peter Norton, MD for contributions in identifying and developing quality measures, Sarah Cooper, RN NP for contributions in the preliminary literature review for this paper and Maggie Wang, MSc for data cleaning, coding and early analysis.
References
Footnotes
Correction notice This article has been corrected since it was first published. Figure 1 has been updated.
Contributors All authors participated in quality measure identification and development. BHR, GEC, CAE and GGC provided expertise regarding clinical practice and clinical importance of quality measures and reviewed drafts or the manuscript. KT and PM drafted the initial manuscript with CR and GEC. GGC, as senior author and guarantor, reviewed and edited all versions of the manuscript.
Funding We acknowledge funding from the following organisations: This work was supported by the Partnership for Health Systems Improvement Programme offered by the Canadian Institutes of Health Research (CIHR PHE 101863), the Michael Smith Foundation for Health Research (MSFHR), Alberta Foundation of Medical Research (AHFMR), Alberta Health Services (AHS), Interior Health Authority, Kelowna, British Columbia (IHA). GGC holds a Centennial Professorship at the University of Alberta; CAE holds a Tier I Canada Research Chair in Knowledge Translation from CIHR; BHR held a Tier I Canada Research Chair in Evidence-based Emergency Medicine from CIHR during the study period.
Disclaimer These funding bodies had no role in design, collection, analysis or interpretation of data.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.