Article Text

Abstract
Access to medical devices are vital to deliver safe patient care. In the context of constrained resources, however, clinical areas often have insufficient basic equipment, which tend to be shared among multiple clinical teams. This can result in delayed patient management and reduced institutional productivity. In our experience, in 2019, while working at Carseview Centre, an inpatient mental health unit in Dundee (National Health Service Tayside), there was only one functioning ECG machine shared between the five wards.
Using the work WhatsApp chat, we aimed to facilitate better sharing of the one machine. Plan, do, study, act (PDSA) 1 intervention introduced the project protocol, which encouraged doctors to post a photo of the device after use, captioned with its location. PDSA 2 involved printing a physical copy of the memorandum and attaching it to the machine to prompt further compliance. In PDSA 3, concise photo-posting guidelines were established and adherence was encouraged to mitigate concerns for potential confidential-data leaks.
A dynamic outcome measure, the overall effectiveness metric (OEM), was conceived to prospectively monitor the effectiveness of our interventions. An OEM ≥1 indicates engagement and thereby improvement, whereby <1 indicates no change compared with baseline.
The intervention in PDSA 1 was a success with an OEM of 3.5. Although no actual data leaks occurred, a potential for concern was raised by a senior doctor. This limited engagement with the protocol during PDSA 2 and 3, causing the OEM to decline to <1 towards the end of the project. Sixty percent reported that the protocol saved them time in locating the machine.
Individual factors, mainly frustration with the current situation, was a primary driver for the initial engagement among doctors. Although other factors such as senior doctor buy-in, may play a greater role in directing longevity of a technology-based quality improvement solution.
- equipment and supplies
- quality improvement
- communication
- efficiency
- organizational
- social media
Data availability statement
Data are available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Access to medical devices are vital to deliver safe patient care. In the context of constrained resources, however, clinical areas often have insufficient basic equipment, which tend to be shared among multiple clinical teams. This can result in avoidable delay in patient management and reduced productivity.
In our personal experience while working at Carseview Centre, Dundee (National Health Service, NHS Tayside) in 2019, an inpatient mental health unit, there was only one functioning ECG machine shared between the five wards. Anecdotally, clinicians reported searching over 1 hour for the machine. Royal College of Psychiatrists and local protocols dictate that ECGs need to be performed and interpreted by medical staff ≤24 hours of a new admission, particularly because they also form part of the initiation and monitoring requirements for many psychotropic medications.1 The junior doctors expressed frustration in locating the one machine when required. In addition to this, one of the wards was located across a garden away from the main building. Often, there were lapses in communication regarding the location of the machine, especially when it was being used by the ward furthest from the main building. There were orders in place for more machines, but the delivery of these were at least 3–6 months away. In the interim, a cost-effective intervention was required to facilitate better sharing of the one machine.
A WhatsApp messenger group with all the current junior doctor’s at the unit was frequently used for communication. A common message posted on a near-daily basis by most members was ‘Where is the ECG machine?’ or ‘Has anyone seen the ECG machine?’.
This quality improvement (QI) project aims to implement a WhatsApp based intervention, using multiple plan, do, study, act (PDSA) cycles, so doctors can easily source the one ECG machine when required. The interventions will be monitored throughout, using a simple proxy indicator suggesting effectiveness; a reduction in the frequency of posts stating, ‘Where is the ECG machine?’ or similar. Additionally, the frequency of engagement with the implemented interventions will also be monitored. Both of these frequencies will be combined into a single number to give an overall effectiveness metric (OEM) for each stage of the project. The OEM that we are aiming for is stated in the design section, with detailed explanation of how the metric was derived from our raw data.
Background
Sufficient availability of essential medical equipment and devices are paramount for service delivery. Equipment shortfall could be an early proxy indicator of other structural and process measures that require improvements within a healthcare system. These measures include staff numbers, communication issues, service delivery times and medical equipment upkeep.2–4 This problem not only impacts low and middle income countries but also developed healthcare systems, although to a lesser extent.2 3 In 2019, an independent investigation was carried out following the death of a mental health service user in Lincolnshire, England.5 Among its 26 recommendations for the trust, it stated that essential equipment such as an ECG machine should be functional and accessible, with clear plans in place to deal with faulty equipment.5
The use of WhatsApp messenger has proliferated rapidly and is now ubiquitous among clinical teams.6 The rate of adoption for any new technology is dependent on two factors: (1) it’s perceived usefulness and (2) it’s perceived ease of use, as outlined in the technology acceptance model.7 WhatsApp groups have been created informally by medical staff to successfully arrange work-rosters, teaching sessions, emergency triage, educational and clinical updates, audits and QI interventions.6 8–12 The social media platform has also provided a faster method to reach colleagues, especially in time-critical situations, surpassing the convention of bleeping or diverting the call through switchboard.8 11 13 Furthermore, doctors have commended the non-hierarchical tone created within a WhatsApp group chat, which facilitates free discussion and instant responses among colleagues.13
Despite its widespread usage in clinical settings, no current guidelines exist to inform clinicians on best practice when using WhatsApp for workplace communication.6 14 Instead clinicians have adopted a common-sense approach to ensure patient confidentiality is preserved and mitigate data breaches. Although messages are encrypted, concerns have been raised, that data could be backed from the user’s mobile device onto unsecure cloud servers overseas, and sensitive information may be leaked if a user’s devices is left unlocked or misplaced.13
Given WhatsApp has previously been used in QI projects to improve the speed of obtaining senior advice, and facilitating patient triage and transfers, it has the potential to offer a creative solution to our problem.8 10 11 From our literature search, no reports were found which tackle our specific problem, of effectively sharing limited equipment in a medical setting. A cross-specialty solution transpired to author AA, taking inspiration from his experience of using Lime scooters while on holiday.15 These electric scooters are dispersed throughout a city, whereby a user can unlock the scooter via an app with a linked credit card. The scooter can be dropped off at any location within the city after use. For the user to unlink their credit card from the scooter, the app requires the user to post a photo from their smartphone, in order to aid search and retrieval of the scooter for the next user. A similar concept can be adopted within our work WhatsApp chat, to facilitate search and retrieval of the shared ECG machine.
Baseline measurement
Baseline data were collected over a 3-week period, from 12 August 2019 to 1 September 2019 by monitoring the group’s WhatsApp chat. Every occurrence of a member posting, ‘Where is the ECG machine?’, ‘Has anyone seen the ECG machine?’ or a statement of similar effect was recorded as an ‘event count’. The event count over the 3 weeks of baseline data collection was 7, (average weekly count=2.3).
Design
Author’s AA and HK are both junior doctors who have faced the stated problem in their day to day clinical work at their respective hospitals. The inception and ground level implementation of the project was done by AA. AA and HK jointly analysed the data prospectively, conceived updates to the interventions and prepared the manuscript. Advise on QI methods and local QI protocols was offered by author VT who is the teaching lead for patient safety at the University of Dundee. This QI report is drafted in accordance with the Standards for Quality Improvement Reporting Excellence reporting guidelines.16
No suitable validated measures were found to monitor interventions for our proposed problem. Henceforth, we conceived a simple outcome measure, the OEM, which will indicate the effectiveness of our interventions solely from monitoring the WhatsApp chat activity on a prospective basis. The OEM is a ratio calculated as follows; OEM=event count/engagement count. An event count is defined in the baseline measurement section. An engagement count is every time a user engaged with the WhatsApp protocol detailed in the strategy section below. An OEM ≥1 indicated engagement with the intervention and improvement, whereby<1 indicates no change compared with baseline. Three PDSA cycles were designed, each lasting for 3 weeks in duration. The PDSA cycles ran consecutively after the end of the baseline data collection period. The total project length was 12 weeks, from 12 August 2019 to 3 November 2019 (inclusive of the 3-week baseline data collection period). The OEM was calculated every week throughout the three PDSA cycles. Our project aim was to ensure the OEM remained ≥1 with each PDSA cycle.
Our proposed data collection method has numerous benefits which includes: (1) simplicity, (2) maximises event capture rate as data is collected live, (3) requires little manpower, (4) eradicates recall bias from participants, to which quantitative questionnaire based methods are susceptible, (5) data remains on the chat history to aid verification retrospectively and (6) evolving group sentiments can be tracked in real-time, with interventions to influence change designed in a dynamic manner.
In order to ensure engagement and sustainability, the WhatsApp group chat was used as the main tool in delivery of this project. This is because the chat was already used heavily between the junior doctor’s in Carseview Centre, so it was assumed that the initial effort required to engage with the project will be low, henceforth maximising uptake. Furthermore, it did not require learning a new system or software nor the physical effort of returning the machine back to a central location after use.
An end of project questionnaire was sent to all of the junior doctors (n=12) using Google forms. All responses were automatically anonymised by Google forms, and the authors could only view the summary responses. At least one doctor from each of the five wards was requested to complete the survey.
Strategy
The intervention for PDSA cycle 1 involved creation and posting of a digital memorandum on the WhatsApp group (figure 1). We aimed to establish the WhatsApp protocol and promote its use in these 3 weeks. The memorandum illustrated a two-step protocol, that junior doctors were encouraged to follow after using the ECG machine. The protocol dictated doctors to: (1) take a photo of the secure location they have left the machine and (2) post the photo on the group WhatsApp chat with caption in the form such as, ‘ECG machine, ward 2, storeroom’. This meant that when the next doctor required the ECG machine, they simply had to search the term ECG on the chat search function, which would have taken them to the most recent post, revealing the current location of the machine. Prior to starting PDSA 1, we ensured that all of the current staff were part of the WhatsApp group and active. As the project went live, the initial feedback was positive, and doctors were appreciative of the initiative. Although by the end of week 3, engagement was dropping, and we realised that the doctors needed to be reminded again of the memo to prevent them from falling back into former habits. Here it was realised that changing behaviour at a group level requires persistence and prompts at critical points where old habits can filter through.
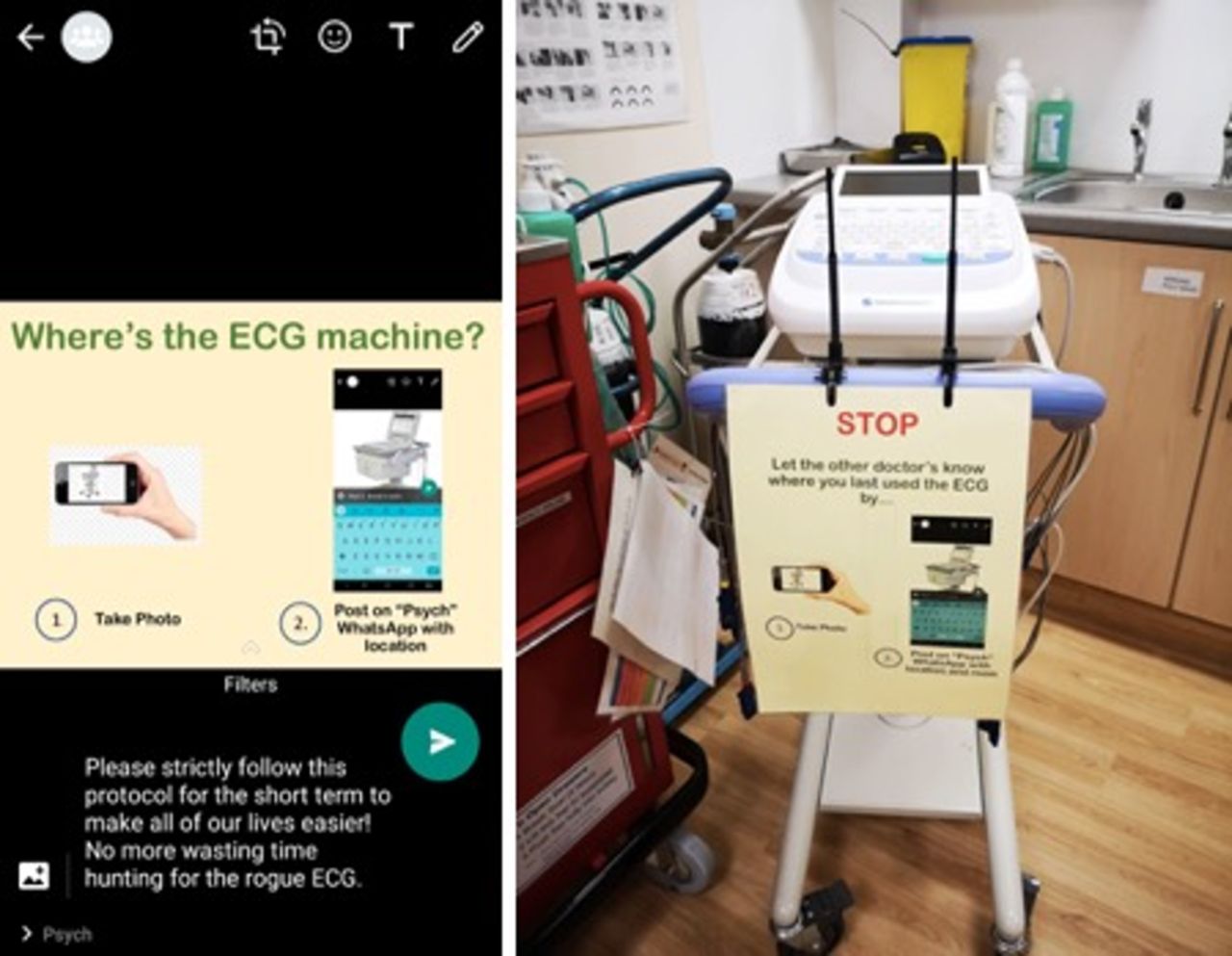
Intervention for PDSA 1 (left) and PDSA 2 (right). PDSA, plan, do, study, act.
The intervention for PDSA 2 involved printing a physical copy of the memorandum and attaching it to the ECG machine to act as an aide-memoir, complementary to the WhatsApp post (figure 1). The memorandum was also re-posted in the group to ensure continued engagement with the project. The aim for PDSA 2 was to monitor continuing engagement with the protocol and encourage its use. From the start of PDSA 2 improvements were hampered as engagement with the memo dropped. This was mainly due to a concern raised by one of the senior doctor’s regarding potential for confidential information leaks, when users were posting photos of the ECG machine location. Despite no actual occurrence of data leaks, it was proposed to only post the location of the machine in words. This was ineffective as shown by continued stagnation of the OEM being <1 through PDSA 2. It was evident that posting a photo with surrounding context of the machine led to better engagement and was of more help to locate the machine within the psychiatry unit.
Learning from PDSA 2, in PDSA 3, we aimed to allay the concerns raised by the senior doctor in order to improve engagement with the memorandum. Concise photo posting guidelines were established to limit any potential for data breaches. The succinct 3-step guideline was as follows: (1) Check your surroundings for confidentiality, (2) Capture photo with sufficient context and (3) Caption location of the machine and post. Furthermore, local trust guidelines were consulted, which had no objections to taking photos of medical devices in the workplace, given no patient identifiable data or person was in the frame. This intervention improved the OEM marginally, from 0.4 to 0.7, yet the OEM remained <1 till the end of the project. It was realised that senior buy-in towards the start of the project could have facilitated better engagement.
Results
Outcome measures compared with baseline
The average weekly event count dropped from 2.3 at baseline to 1.7 in PDSA 1. This improvement is also reflected with a maximal OEM of 3.5 during PDSA 1, where OEM ≥1 indicates QI. The weekly average event count increased to baseline levels during PDSA 2, followed by a rise above baseline to 2.7 in PDSA 3. This is reflected in the stagnant OEM of 0.5 through PDSA 2, followed by a slight increase to 0.7 at the start of PDSA 3 with the introduction of the photo posting guidelines. Yet the OEM remained below threshold for improvement for the remainder of the project which ended on an OEM of 0.4 (figure 2).

The overall effectiveness metric (OEM), shows the effectiveness of our interventions solely from monitoring the WhatsApp chat activity on a prospective basis. OEM = event count/engagement count. Every occurrence of a member posting, “Where is the ECG machine?”, “Has anyone seen the ECG machine?” or a statement of similar effect was recorded as an event count. An engagement count is every time a user engaged with the WhatsApp protocol detailed in the strategy section and figure 1. An OEM ≥1 indicated engagement with the intervention and improvement, whereby <1 indicates no change compared to baseline. Bar-chart showing event counts through study period (left). Run chart for PDSA 1 to 3 outlining each intervention with resultant OEM (right). PDSA, plan, do, study, act.
End of project survey
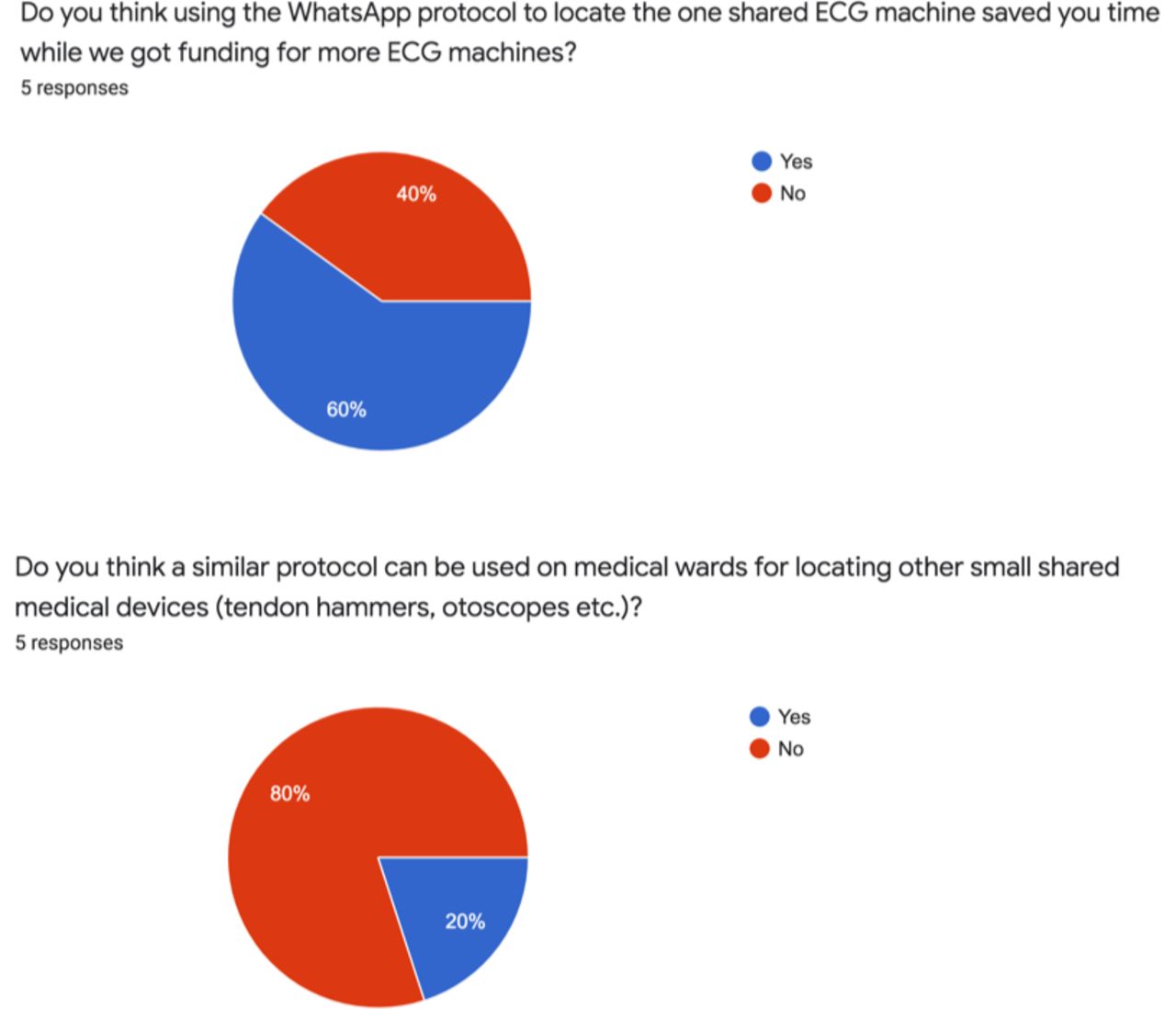
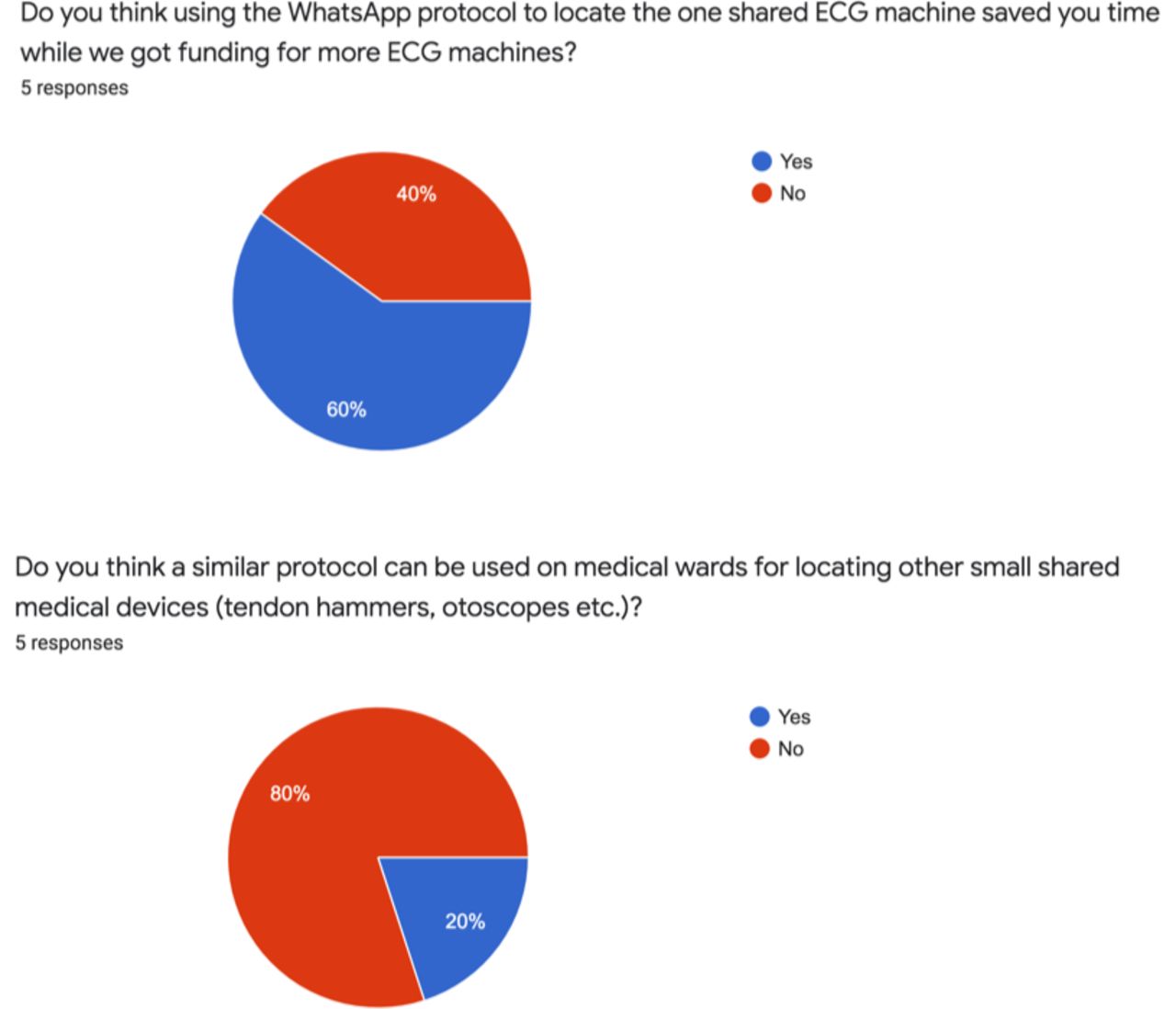
Sixty per cent reported that the WhatsApp protocol saved them time to locate the one ECG machine in the unit, while we awaited funding and delivery of more machines (figure 3). Only 20% felt that a similar protocol can be successfully implemented in other surgical or medical wards. The reasons for this included; such a protocol worked well in a small self-contained unit like Carseview Centre but might be less successful in more complex ward setups, with frequent staff changes and addition of locum staff. One respondent suggested an alternative strategy, that has worked well for an out-of-hours swipe card for the unit. This strategy involves agreeing to a central location among the doctors for the ECG machine to be held, with a sign-out diary, when a doctor takes the machine away from the central location, they list their name, ward and time in the diary for accountability. The machine needs to be returned back to the central location by the user. Another respondent recognised that senior buy-in prior to starting the project could have sustained engagement.
{kind=link}
{kind=link}
{kind=link}
Pie-charts summarising junior doctor participants feedback following completion of the QI project. QI, quality improvement.
Discussion: lessons and limitations
Our outcome measure could have been influenced by variability in admissions on certain weeks compared with others. Furthermore, during busy periods staff may not fully engage with the intervention, reverting back to old habits. Looking at our data this is unlikely as the event count remained stable between 2 and 3, throughout most of the 12 weeks.
Second a concern was raised regarding the potential for the leak of confidential information, when users were posting photos of the location of the ECG machine. No nationwide guideline exists at present for clinical staff using WhatsApp for work communication, despite its routine use, henceforth we established local guidance for posting of photos taken in clinical environments as one of our PDSA interventions.14 Moving forwards, we can encourage clinical teams to start using WhatsApp like apps (WLAs), such as Hospify. These apps are approved by the NHS apps library and meet the General Data Protection Regulation, but current uptake of WLAs within clinical environments is variable.13 17 The barrier to uptake maybe explained in the context of the technology acceptance model, where the perceived usefulness of WLAs are likely to be high but their perceived ease of use is likely rated low.7 Therefore, we recommend hospital trusts/health boards to encourage staff uptake of WLAs through an addendum in their local e-communication policies.
Future tech-based QI projects can look at creating their own in-house communication apps, tailored to local infrastructure setups, to enable a more intuitive experience. A successful local example of such in the electronic patient records arena is Ekora, by clinical IT, a tech-based QI solution to move away from paper notes, especially at the advent of COVID-19.18 Ekora was initially trialled within NHS Tayside cardiology units, with subsequent roll out to other departments in the health board. One of the reasons for Ekora’s success and sustainability can be attributed to it being led by senior clinicians, with a long-established reputation within NHS Tayside.
Third, the response rate for the end of project survey was 42%. We accept that this is on the low side, yet it is above the average response rate for web surveys (33% in 2021).19 Although the project concept may not be transferrable to all centres facing an equipment shortfall, a limitation eluded to by one of the survey respondents, it remains a prototype to address the stated problem.
Ultimately, it was realised that senior staff buy-in, prior to rolling out the project may have sustained engagement at the later stages. This was also mentioned in the end of project survey. Thus, in future projects, we will hold an initial focus group with key stakeholders to seek their opinion, concerns and backing. Furthermore, this would give us an early opportunity to answer any questions, in order to mitigate future barriers and maximise sustainability.
Conclusion
Prompt access to shared medical devices for clinicians is vital, in order to deliver a safe standard of care and prevent avoidable delays. Inpatient units within the NHS often face equipment shortages. At our centre an innovative solution was required to meet the immediate shortfall of ECG machines. Therefore, we proposed the use of our work group WhatsApp chat, for staff to post a photo captioned with a concise location of the machine, as a promising solution to reduce the search and retrieval time of the one shared machine. Furthermore, local photo-posting guidelines were established, which the staff were prompted to follow, to mitigate any incidental confidential data breaches.
It was evident from this project that individual factors, such as access to the work WhatsApp chat and frustration among junior doctors with the current situation, was a primary driver for the initial engagement with the intervention. It seems that organisational factors, such as senior doctor buy-in, may play a greater role with regard to sustainability of an innovative QI solution.
Data availability statement
Data are available upon request.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Footnotes
Contributors AA and HK are both junior doctors who have faced the stated problem in their day to day clinical work. The inception and ground level implementation of the project was done by AA. AA and HK jointly analysed the data prospectively, conceived updates to the interventions and prepared the manuscript. Advise on QI methods and local QI protocols was offered by VT who is the teaching lead for patient safety at the University of Dundee. AA is the guarantor for this project and accepts full responsibility for the work from conception to publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.