Article Text

Abstract
Background Patients with ESRD comprise less than 1% of the Medicare population, however they are responsible for 7% of all Medicare spending. Hemodialysis (HD) and peritoneal dialysis (PD) have equivalent clinical outcomes; however, PD is more cost-effective. Undocumented immigrants, when given access to dialysis, are suspected to have lower PD utilization.
Objectives Establish baseline PD utilization rates amongst patients stratified by funding status, design an intervention to improve PD utilization, and assess impacts of interventions on utilization rates.
Methods The intervention was designed by using interview data to identify patient and provider barriers to selection of PD and stratifying the top failure causes through failure modes and effects analysis (figure 1). PD utilization rates before and after the intervention were determined through a retrospective chart review. The impact of the intervention on patient understanding was assessed with patient surveys.
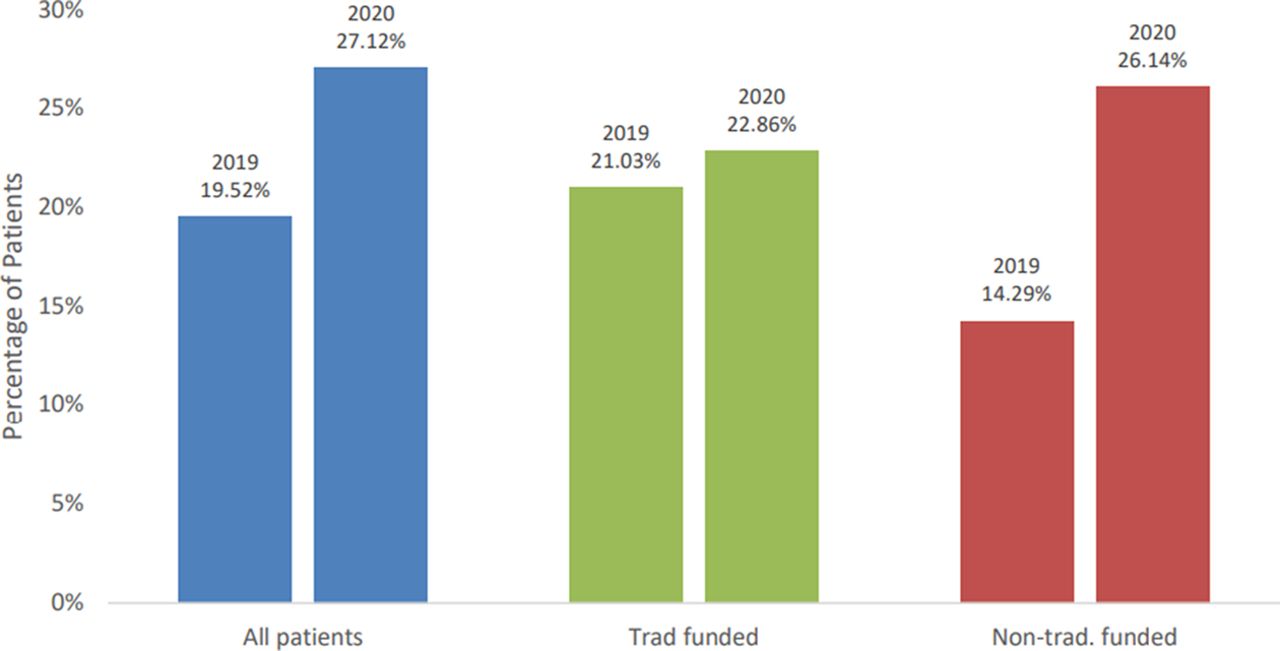
Results The chosen intervention was to revise educational materials to address common misconceptions. Prior to the class update, the utilization rate for PD was 14.3% in the non-traditionally funded group, primarily containing undocumented immigrants, compared to a 21.0% utilization rate in the traditionally funded group. After the updated class was implemented, PD utilization in increased to 26.1% and 22.9% in the non-traditionally and traditionally funded groups, respectively (figure 2–4). Preliminary data from post-class patient surveys suggests that patients with a better understanding of class material are more likely to make an earlier selection of a dialysis modality.

Fishbone diagram summarizing results from 17 patient interviews and 9 provider interviews (2 nephrologists, 3 NPs, 2 social workers, 2 nurse navigators). Interviews were conducted to understand patient perceptions of PD as a modality and characterize barriers to PD. The top failure modes are highlighted in red. These were utilized for a failure modes and effects analysis (FMEA) which was used to identify top failure causes

Dialysis modality preferences for all patients at the Advanced Stage CKD clinic compared to patients who may qualify for outside funding and those who utilize traditional funding, prior to interventions, from 03/14/19–07/14/19. n=251 for all patients, n=195 for traditionally funded. n=56 for non-traditionally funded

Dialysis modality preference for patients at the ASCKD clinic from 07/2020–10/2020, after the intervention. n=153 for all patients, n=118 for traditional funding, n=35 for non-traditional funding
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Peritoneal dialysis (PD) utilization rates at the ASCKD clinic at Parkland hospital from 2019–2020, stratified by funding status
Conclusions Addressing patient misconceptions about peritoneal dialysis by updating educational materials is an intervention that can increase the utilization rates of PD in patients with non-traditional funding. External factors could have played a role in increased PD utilization and additional data is needed to establish a more robust correlation.