Article Text

Abstract
Background Frailty measurement is recommended when assessing older adults with cardiovascular disease to individualise prevention and treatment. We sought to address this by incorporating routine gait speed measurement by clinicians into an outpatient preventive cardiology clinic.
Methods Quality improvement (QI) project initiated at VA Boston in January 2015 to measure usual gait speed in m/s over a 4 m distance for patients aged 70 and older. The primary outcome was completion and documentation of 4 m usual gait speed. Data were manually extracted from the electronic health record. Frequency distributions and descriptive statistics are presented.
Interventions Several change interventions were implemented over a 5-year period (January 2015–December 2019) addressing (1) stakeholder engagement and project champions, (2) staff education, (3) assessment space, (4) electronic health record template update and (5) sustaining the initiative. Statistical process control charts were used to monitor proportion of gait speed measurement and to detect shifts resulting from 5 phase change interventions.
Results During this QI project, 178 patients aged 70 and older attended the clinic, accounting for 1042 individual clinic visits. Gait speed was measured at least once for 157 patients; 21 were never assessed. At the end of the first month (January 2015), gait speed was measured during 40% of clinic visits and rose to a median measurement rate of 78% at clinic visits during the 2018–2019 study period. An unanticipated result was the spread of the initiative to other cardiology clinics.
Conclusions Gait speed measurement was successfully embedded into clinic assessments for older adults at a cardiology clinic following targeted interventions. This project highlights the feasibility of incorporating a brief frailty assessment such as gait speed, into non-geriatric medicine clinics.
- ambulatory care
- quality improvement
- control charts/run charts
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Problem description
A core principle in cardiovascular disease (CVD) prevention and promoting healthy ageing is physical activity and exercise. Patients seen in primary care or a preventive clinic may have an activity history taken and be counselled on the value of increasing exercise, however, routine assessment of a functional measure such as gait speed is missing from both guidelines and usual care.
Available knowledge
Slow gait has emerged as a powerful predictor of CVD risk, mortality1 2 and poorer neurocognitive outcomes later in life.3 Furthermore, gait speed is considered a single marker of frailty,4 that can serve as the ‘sixth vital sign’ of functional capacity.5
Recognising frailty can identify older adults at increased risk of both cardiovascular (CV) events and potential treatment harms.6 7 For this reason, major CV guidelines have begun to include frailty, although with minimal guidance as to how it should be measured is provided.8 9
Gait speed is a rapid, easy, cost-neutral and sensitive tool, with excellent inter-rater and test–retest reliability, even for patients with cognitive impairment.10–12 Beyond its ability to predict risk and indicate pathology in the cardiopulmonary and musculoskeletal systems, gait speed can be considered an integrator of all body systems.
Rationale
Detection of slow gait speed in routine clinical care provides an opportunity to create person centred treatment goals and to seek modifiable signs of and contributors to frailty. However, to date, there has been limited incorporation of gait speed or other frailty assessments into the routine CV care of older adults.
Specific aim
We aimed to introduce gait speed measurement into the routine clinical evaluation of all patients age 70 and older seen in a Cardiology clinic over a 5-year period. Prior to initiation of this project, there was no formal assessment of frailty in any subspecialty clinics at the Veterans Administration (VA) Boston Healthcare System. We hypothesised that identifying frail patients using gait speed in a busy outpatient cardiology clinic would be (1) feasible, (2) sustainable over a 5-year period and (3) effective in identifying patients at risk of decline and prompting investigation and management of frailty syndromes in an at-risk population.
Methods
Context
We initiated a quality improvement (QI) project in a single Preventive Cardiology Clinic at VA Boston Healthcare System in January 2015 aimed at incorporating gait speed into the assessment of all patients aged 70 and older. A geriatrician was embedded into the clinic from the start of the project. Change interventions were implemented on a phased basis over a 5-year period.
Gait speed measurement
Usual gait speed was measured by the clinician seeing the patient in metres per second over a 4 m distance. This included both preventive cardiology fellows and attending physicians. The assessment was performed as the patient was escorted from the clinic waiting room to the assessment room (figure 1). Patients were asked to walk at their normal pace and were permitted to use their prescribed adaptive device (such as cane or walker) and eyeglasses, if applicable. The patient was observed walking over a 2 m acceleration zone, followed by a 4 m assessment zone and then a 2 m deceleration zone. The observing clinician stood slightly behind the patient while they were walking and avoided talking during the measurement to reduce distraction. The time taken to walk the 4 m assessment zone was measured in seconds (sec) with a stopwatch to the nearest 0.01 s. A gait speed of less than 0.8 m/s was considered slow.5

Gait speed assessment zone embedded into the existing clinic space.
Interventions
During the project, five change interventions were implemented to improve rates of gait speed measurement; (1) stakeholder engagement and project champions, (2) staff education, (3) assessment space, (4) electronic health record (EHR) template update and (5) sustaining the initiative.
Study of the interventions
Each clinic assessment note was manually reviewed for documentation of gait speed measurement. Data regarding demographic and comorbidities, including hypertension, diabetes, hyperlipidaemia, coronary artery disease, arthritis, atrial fibrillation, congestive heart failure were collected from the EHR. The project implementation team reviewed number of gait speed measurements completed at clinic visits on a monthly basis and following each change intervention.
Measures
Data were collected for up to 5 years following the initial clinic visit. The primary outcome measure was completion and documentation of 4 m usual gait speed during the patient’s preventive cardiology clinic assessment. Data on those missing gait speed measurement were collected. Secondary outcomes were referrals to physical therapy (PT), occupational therapy (OT) and geriatric medicine. Mortality and hospital admission rates were also collected.
Analysis
Demographic and baseline disease characteristic data were summarised for the study population by presenting frequency distributions and descriptive statistics. Means and SD were calculated for normally distributed data. Median and IQR were calculated for non-normally distributed data.
Statistical process control (SPC) charts were used to monitor proportion of gait speed measurement and to detect any shifts resulting from change interventions.13 SPC charts were constructed using QIMacros SPC Software for Excel V.2018.10 (KnowWare International, Denver, Colorado, USA).
The findings of this study were reported in keeping with Standards for Quality Improvement Reporting Excellence V.2.0 publication guidelines.14
Implementation and strategies
The five-phase change interventions implemented are described in detail below along with improvements in gait speed measurement at clinic visits in response to these interventions.
Intervention 1: stakeholder engagement and identification of project champions
Relevant stakeholders were identified by stakeholder mapping and consulting with the clinic team prior to initiation of the project. These included other preventive cardiology attendings, fellows, nurses and clinic administrative staff. We engaged with stakeholders through one to one and small group meetings. A key one to one meeting was held with the director of the preventive cardiology clinic. The importance of identifying frailty in older patients with CVD was described and buy in was secured. An important element of this was highlighting that the addition of gait speed measurement, which takes only 5–10 s to complete, would not significantly increase clinicians’ time with a patient. Finally, the proposal for this QI project was presented at the local department of cardiology grand rounds in early 2015 which enhanced stakeholder engagement. The project team leader, a geriatrician with training in preventive cardiology, was a key champion embedded in the clinic. This physician was present at the clinic weekly and maintained stakeholder commitment to the project. Rotating geriatric medicine fellows at the clinic also acted as champions in sustaining the measurement of gait speed measurements.
Intervention 2: staff education
To further ensure buy in of all clinical staff, as part of regular didactic sessions, all preventive cardiology fellows and attending physicians were educated on the value and method of usual gait speed measurement.1 Differential diagnosis for slow gait speed was reviewed, including those which should be immediately addressed such as symptoms of acute coronary syndrome, orthostatic hypotension, hypoglycaemic and use of sedating medications. These sessions were led by a physician board certified in geriatric medicine, and began in December 2014 in anticipation of project launch. Preventive cardiology fellows were prompted to report the gait speed result during precepting with the clinic attending physician. Brief educational sessions and reminders were repeated throughout the project. Fellows were encouraged to educate new and rotating clinic staff on gait speed measurement technique. Gait speed measurement during the first 4 months of the project improved following this intervention (highest recorded proportion 57%). However, variability in measurement remained high (range 29%–57%).
Intervention 3: creation of an assessment space
To make it easy for clinicians to measure gait speed a dedicated area for gait speed measurement in the cardiology clinic was identified early in the project. A corridor which all patients must walk through to reach the clinic rooms was chosen. A 4 m distance was measured with a 2 m distance on either end and brightly coloured tape was applied first to the floor and then to the wall at eye level marking the distance. This ensured that the assessment space was easily identifiable to all team members. It also allowed for easy incorporation of gait speed measurement into the clinic visit, as all patients would walk this 4 m distance on their way from the waiting room to the consultation room. Clinic staff reported that this dedicated assessment zone facilitated ease of gait speed measurement served as a reminder to perform the assessment.
Intervention 4: EHR template update
In July 2015, after 6 months of fellow education and gait speed measurement, it became clear that even if gait speed was being measured it was not always documented as there was no dedicated place in the chart to record it. Permissions from the department of cardiology were obtained to modify the EHR note template for all cardiology clinics. The physical examination portion of the template was expanded to include ‘gait speed assessment’ along with a brief explanation of how to interpret the results (‘not frail if able to walk four metres in <5 s’). This change resulted in a shift in proportion of gait speed measurements and the median proportion increased to 69% of all clinic visits for older patients.
Intervention 5: minimise variation in gait speed measurement and sustain improvements
Regular educational updates were held with the preventive cardiology clinic staff to sustain rates of gait speed measurement. Whenever a change in clinic personnel occurred, it became clear that education on gait speed measurement was needed. This was repeated by a board-certified physician in geriatric medicine. This was particularly important at the start of a new training cycle (July). Trainees were regularly reminded during precepting to measure gait speed. The educational component of this project was published in January 2018 as an online continuing medical education article at the Cleveland Clinic Journal of Medicine.15 This article was given to all new trainees.
Results
Baseline data
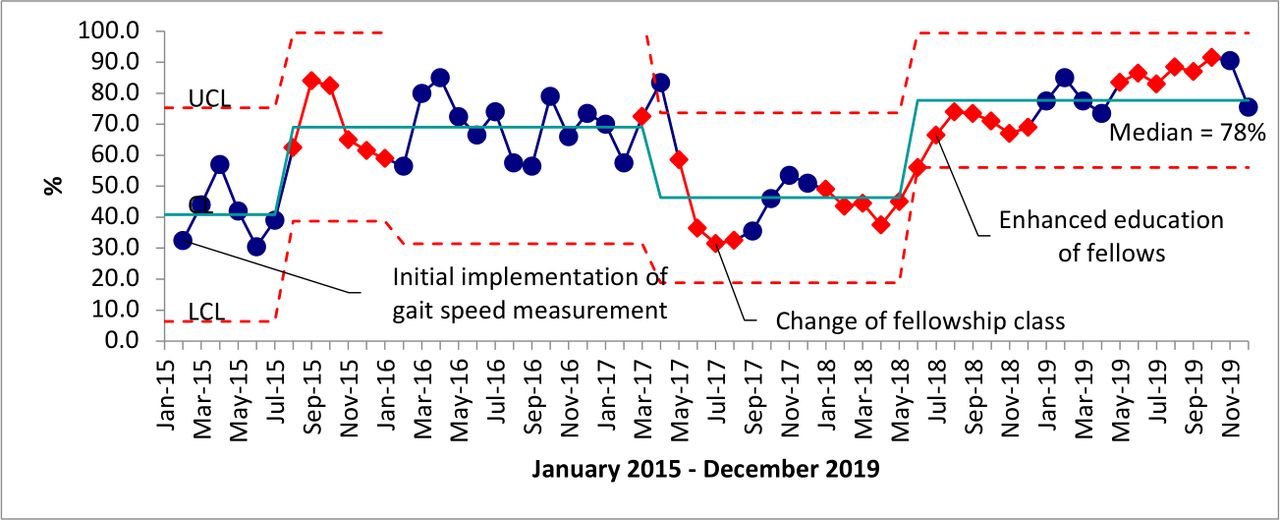
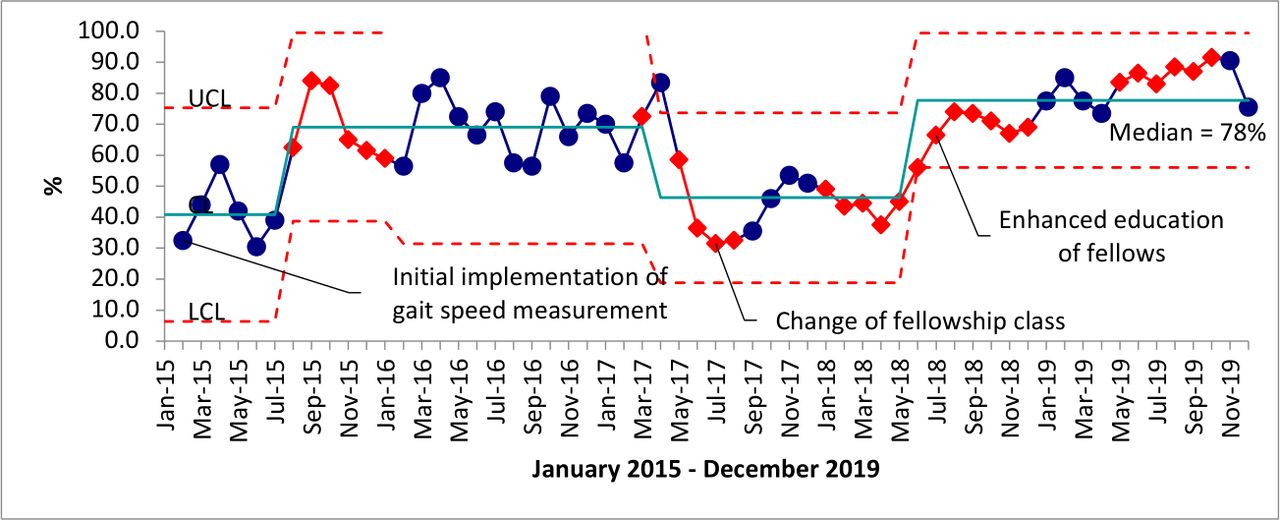
Prior to initiation of this project, gait speed measurement was not routinely performed in any of our organisation’s cardiology clinics. Over a 5-year period (January 2015–December 2019), 178 patients aged 70 and older attended the preventive cardiology clinic, accounting for 1042 individual clinic visits. At the end of the first month (January 2015), gait speed was measured during 40% of clinic visits. The trends for gait speed measurement throughout the duration of the project are shown in figure 2. Over 5 years, gait speed was measured at least once for 157 patients. In total, 21 patients attending the clinic never had a gait speed assessment. The baseline characteristics for these patients are described in table 1.
Baseline characteristics for 178 patients according to gait speed
{kind=link}
{kind=link}
Bimonthly statistical process control of rates of gait speed measurement (%) during preventive cardiology clinics (January 2015–December 2019) for patients aged over 70. LCL, lower control limit; UCL, upper control limit.
Those who had slow walking speed were older (79 vs 75 years), had a higher mean systolic blood pressure (133 vs 128 mm Hg), and higher prevalence of hyperlipidaemia, coronary artery disease and arthritis.
Overcoming barriers
In total, 21 patients who attended the clinic over the 5-year period did not have gait speed measured. We assessed the reasons why gait speed was missing or not measured (online supplemental appendix figure 1). The most common reason for not measuring gait speed was inability to walk 4 m due to cardiorespiratory limitations or immobility with wheelchair use (n=12). One patient was not assessed due to time constraints.
Supplemental material
From April 2017 to April 2018, a decrease in rates of gait speed measurement were observed. We believe this occurred as the cohort of fellows may not have been as engaged as at other times. This was addressed by repeating small group stakeholder engagement meetings and brief educational sessions with clinic staff. Targeted reminders to preventive cardiology fellows by senior clinicians to measure gait speed were also provided. Following these renewed interventions, we observed a further shift in proportion of gait speed measurements at clinic visits to 78% (figure 2).
Secondary outcomes
Table 2 details rates of referrals to other services (eg, therapy and geriatrics), hospitalisation and mortality rates. Slow walkers had higher rates of referral to PT (14% vs 2%) and geriatrics clinic (8% vs 1%). Slow walkers were also more likely to be admitted in 1 year (38% vs 26%) and more likely to die during 4 years of follow-up (32% vs 9%).
There were no additional costs incurred in implementing this project.
Outcomes according to gait speed
Additional outcomes
Although not initially planned, the success of this project in a single cardiology clinic led to the natural expansion to other Cardiology clinics, including electrophysiology, heart failure and valvular disease. In July 2019, a geriatrics consult clinic was formally embedded into the VA Boston cardiology service.
Discussion
Summary
Gait speed is a well-recognised measure of frailty in patients with CVD either as a single measure or used as a component of a frailty assessment score.4 Through this QI project, we were able to successfully establish and maintain gait speed measurement as part of routine care in a preventive cardiology clinic. A particular strength was the sustained improvements in measuring gait speed at a single site over a 5-year period. Secondarily we found an increase in referrals to PT and geriatrics, as well as increased mortality among slow walkers.
Gait speed measurement rates went from not assessed at all to 40% of clinic assessments at the early stages of the project, to a median measurement rate of 78% at clinic visits during the 2018–2019 study period. Embedding a tool to assess frailty in a non-geriatric medicine clinic with a high prevalence of older adults is a feasible initiative.
Interpretation
We identified several interventions that contributed to our results. These included: ease of documentation and the need for strategic and ongoing education particularly at vulnerable transitions such as change in trainee cohorts.
This project required clinicians performing CV assessments to incorporate a clinical measure more typically performed in geriatrics clinics. Stakeholder meetings describing the potential benefits to patients, the minimal increase in workload for team members and the cost neutrality of implementing this measure were all key in obtaining support from members of the clinical leadership team. In turn, leadership support of the project was influential in acquiring buy in from clinic staff.
Securing buy in from patients did not pose a challenge as gait speed assessment was performed as part of their routine clinic visit, did not prolong their visit or require them to move to a different location, and did not replace any other aspect of their assessments. In reviewing reasons for why gait speed was not measured, only in one case was time constraint the cause suggesting that time limitations should not be a barrier for others looking for a simple way to measure frailty in a busy clinic. Furthermore, sustainability was also maintained by the routine review of gait speed during precepting by attending physicians in the clinic.
Existing services such as cardiac rehabilitation are beneficial to older patients with CVD and focus predominantly on aerobic exercise. However, patients with physical frailty and slow gait speed may need additional interventions to address balance, lower limb strength and postural stability.16 Once slow gait speed is recorded, there is an opportunity to refer the patient to services which may not be classically considered in a cardiology clinic such as PT and OT, both of which can be targeted to focus on frailty specific goals.16 Formal referral for comprehensive geriatric assessment may also be considered where resources are available. In this study a geriatrician was embedded in the clinic and the natural extension of this project has been the incorporation of an embedded geriatrics clinic within cardiology, bringing care directly to the patients who need it most.
The improvements seen in this single site project have had positive impacts at the departmental level. We have observed spread of gait speed measurement to other cardiology clinics. While not formally studied, our impression is that this occurred because gait speed measurement is simple and can quickly give insights into a patient’s functional and frailty status. Furthermore, over the time period of this project, several CV guidelines called for frailty assessment,8 9 and gait speed presents one way to do this, without incurring additional costs or personnel. Following brief training on gait speed measurement, any clinician or qualified member of an interprofessional team can complete this assessment in approximately 30 s during a clinic visit (10 s to instruct patient on gait speed assessment method, 10–20 s to complete assessment). Future directions are to expand this model of focused assessments of frailty to other medical specialty and primary care clinics.
Although there is growing consensus on the importance of measuring frailty in older patients seen in cardiology clinics,6 there is little published literature to date specifically describing a clinical model of embedding geriatric assessments in cardiology clinics and related outcomes. A study of 131 older adults assessing the relationship between gait speed and outcomes following cardiac surgery found that slow gait speed was associated with increased postoperative morbidity and mortality (OR 3.05; 95% CI 1.23 to 7.54) and longer hospital stays.17 A study of 309 older adults with coronary artery disease found that slow gait speed was an indicator of frailty and was more predictive of mortality than the composite score on a more comprehensive frailty index (OR 3.8, 95% CI 1.1 to 13.1).18 Our study takes the existing literature about the value of gait speed for risk prediction and as a modifiable vital sign and demonstrates the feasibility of integrating gait speed assessment into regular care.
The importance of identifying frailty in patients with CV disease has been recognised by the European Association of Preventive Cardiology, particularly with regard to patient suitability to partake in Cardiac Rehabilitation. Their 2017 position paper recommends collaboration between cardiologists and geriatricians in assessing frailty in cardiology patients.19 While there may not be enough geriatricians to see all CV patients, all Cardiologists can learn to measure gait speed.
Completion of a comprehensive geriatric or frailty assessment in a non-geriatric medicine clinic can be a challenge. The skillsets of the clinicians, time allotted for consultations and the clinic workspace and equipment may not be conducive to performing these assessments. Choosing brief and easy assessments to perform which are reliable indicators of frailty is an alternative to screen for frailty in a cardiology clinic and identify patients who require more in-depth geriatric assessment. Gait speed can be used as a single measure of physical performance and has been shown to identify patients at risk for hospitalisation.10
Limitations
All clinic staff were aware that a QI project was taking place and that the clinic leadership team were committed to the success of the project. This may have influenced staff adherence to gait speed measurement. It is possible that this influence enhanced the improvements seen with other interventions. Additionally, gait speed assessment was largely done by the fellows in clinic and was not delegated to support staff which may limit generalisability to other clinics. However, if gait speed is routinely measured along with vital signs by clinic support staff, it may be easier to implement.
This project was conducted in a cardiology clinic where one attending physician on the team is a board-certified geriatrician. This may have influenced the positive response to the project from clinic leadership and the sustainability of the project. Future work will examine the implementation of gait speed measurement in other cardiology clinics where this physician does not attend.
We found variability in rates of gait speed measurement with the annual change in clinical fellows and trainees. Including permanent staff such as nurses or medical assistants to measure gait speed as part of usual vital sign assessment could be considered. This was particularly evident during 1 year when median rate of gait speed measurement decreased to 46%. This decrease highlighted the importance of focusing on regular fellow education and strong leadership from the attending physicians in the clinic.
While we completed regular focused educational sessions with clinic staff members, we did not formally measure the effect of each of these sessions with individual Plan, Do, Study, Act (PDSA) cycles.
Conclusions
Gait speed measurement was successfully embedded into clinic assessments for older adults at a cardiology clinic during this project. Gait speed measurement improved following several targeted interventions. These improvements were sustained and gait speed measurement is now spreading to additional cardiology clinics within our institution due to its ability to quickly identify frailty. This project highlights the feasibility of incorporating brief assessments of mobility and frailty such as gait speed into non-geriatric medicine clinics.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrAROrkaby
Contributors ARO initiated the project and acted as project sponsor, contributed to project design, data collection and analysis and drafted and revised the paper. ARO is guarantor. KJ contributed to project design, data collection and analysis, and drafted and revised the paper. JL and ES collected and analysed qualitative data, and drafted and revised the paper. JMG was colead and clinic champion. He contributed to project design and critically revising the paper. JAD acted as project lead, contributed to project design, data collection and analysis, and drafted and revised the paper.
Funding ARO is supported by VA CSR&D CDA-2 award IK2-CX001800.
Disclaimer The funding source had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This project was reviewed by the local VA Boston R&D Committee and determined to be non-research.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.