Article Text

Abstract
Introduction CT use for renal colic has increased costs, radiation exposure and frequently does not alter management. Consequently, choosing wisely (CW) recommends avoiding CT imaging of otherwise healthy patients younger than 50 years presenting with symptoms of recurrent, uncomplicated renal colic. We evaluated the utilisation of CT imaging for this subgroup of patients and subsequently implemented a quality improvement initiative with an aim to reduce unnecessary radiation exposure.
Methods A retrospective chart review was performed for all patients younger than 50 years who visited Sunnybrook Health Sciences Centre emergency department (ED) between December 2015 and May 2016 with a discharge diagnosis of renal colic. After the audit period, emergency physicians were engaged to perform a root cause analysis and a driver diagram was developed. In December 2016, a clinical decision tool was introduced to standardise the imaging for patients with presumed renal colic. In May 2017, a separate electronic order was created for low-dose CT for renal colic, including a prompt to remind clinicians of the CW recommendation. The impact of these changes was measured over 15 months.
Results Over the initial audit period, 17/63 (27%) of our target population received a CT to rule out renal colic. Many patients received multiple CT scans for renal colic during past ED visits, while one received a total of 13 CTs. At the time of our interventions, the baseline rate of CT scans in our target population was 37%, which reduced to 29% after our project began.
Conclusion CT is often used as an initial diagnostic modality for suspected recurrent renal colic despite current guidelines. While this initiative caused only a modest change in management, it led to the introduction of a new low-dose CT scan order specifically to reduce radiation exposure in patients at risk for repeat scans.
- quality improvement
- compliance
- decision making
- emergency department
- acute Kidney Injury
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Urolithiasis is the process of forming stones along the urinary tracts, including the kidney, bladder and urethra. Acute flank pain due to suspected urolithiasis is a common reason for emergency department (ED) visits, accounting for more than 1 million visits in the USA annually.1 The estimated lifetime incidence of these urinary stones is 12%, they most commonly presents in patients between 30 and 60 years of age, and they are three times more common in men.2
Non-contrast abdominopelvic CT has become the most common initial imaging study for suspected urolithiasis due to its high sensitivity for urinary stone disease, which ranges from 91% to 100%.3 Unlike other imaging modalities such as ultrasonography (US), CT exposes patients to high levels of ionising radiation with consequent long-term cancer risk.4–7 It has been estimated that 14 000 additional cancers in the USA may be attributable to unnecessary abdominal and pelvic CT scans.8 These avoidable scans can also lead to increased false positives and incidental findings, resulting in unnecessary patient anxiety and inappropriate follow-up interventions, further exacerbating the cycle of unnecessary and potentially harmful care.9 These interventions additionally contribute to increased system-level costs of acute renal colic, which currently amount to over $5 billion annually in the USA.10 Furthermore, there is no evidence to show that increased CT use, despite its higher sensitivity, is associated with improved patient outcomes.11
While ultrasound has lower sensitivities to visualise urinary stones, it is an alternative imaging modality which may be used to investigate renal colic without exposing patients to ionising radiation.12 Furthermore, ultrasound can accurately detect hydronephrosis, perinephric fluid and abnormal ureteric jets, which increases the sensitivity for detecting kidney stones when they are too small to be visualised directly.13 As such, the importance of reducing unnecessary CT imaging for presentations of renal colic is recognised at an international level. In support of choosing wisely (CW), the growing international movement to reduce the overuse of unnecessary medical interventions, the American College of Emergency Physicians (ACEP) released 10 recommendations specifically targeting ED interventions.14 One of these recommendations was to ‘avoid ordering CT of the abdomen and pelvis in young, otherwise healthy emergency department patients (age <50) with known histories of kidney stones, or ureterolithiasis, presenting with symptoms consistent with uncomplicated renal colic’.14
Thus, the first objective of this study was to perform an audit assessing the degree of utilisation of CT imaging for this subgroup of patients at a tertiary care centre ED. Subsequently, a quality improvement (QI) study was designed and implemented with an aim to reduce unnecessary radiation exposure. A subaim was to achieve over 90% of patients under the age of 50 years presenting with recurrent, uncomplicated renal colic to be managed without a CT abdomen.
Methods
Audit setting and population
A retrospective chart review was performed for all patients younger than 50 years who visited the ED of a large tertiary care centre in Toronto, Canada for 6 months between December 2015 and May 2016 with an ED diagnosis of renal colic. Patients who received a discharge diagnosis of renal colic during this period were identified through use of ED information system (EDIS). Using electronic medical records (EMRs), patients from this group were identified whose management did not comply with this CW recommendation. These patients were under the age of 50 years, had a history of renal colic, presented with uncomplicated renal colic and received a CT scan. Uncomplicated renal colic was defined based on presentation to the ED: (1) temperature < 37.8°C on presentation, (2) absence of refractory vomiting requiring >3 doses of Ondansetron, (3) absence of refractory pain requiring >15 mg of morphine equivalents, (4) absence of a history of underlying urological or nephrological problems and (5) absence of significant renal impairment evidenced by serum creatinine <120 µmol/L. All patients meeting these criteria were considered to have uncomplicated renal colic and were included in the study. Patients were excluded from the study group if they received CT imaging to rule out other conditions in addition to renal colic (eg, rule out renal colic and appendicitis).
CT was available 24 hours, but US was available from 07:00 to 16:00 each day. For ultrasound ordered after 16:00, patients were either instructed to return the following day to receive their scan or kept in the ED until the morning.
Audit data collection
For each patient, their demographic data, relevant prior medical history, clinical presentation, lab values, ED medications administered, diagnostic imaging ordered (including time of order entry, indications and findings) and dispositions were recorded. All data were abstracted from the EMRs of patients. Laboratory results collected included serum creatinine and serum white blood cell count, as well as urinalysis for red blood cells and white blood cells. Key clinical features assessed included presence of flank pain, gross haematuria, nausea and vomiting, and signs of infection.
Interventions
A team of healthcare professionals was established including an emergency physician, a radiologist, a urologist, a clinical nurse educator and an information technology specialist. In consultation with emergency physicians, a root cause analysis was performed, and a driver diagram was developed to identify change ideas, displayed in figure 1. The first intervention was to standardise the decision-making to order CT scans for renal colic. To achieve this, in December 2016, an educational campaign was initiated for emergency physicians. Physicians were surveyed regarding their reasons for ordering CTs in the target population and a root cause analysis was performed. They were subsequently educated about the CW recommendation and the rationale behind it. Physicians were then introduced to a validated decision tool based on sex, time course of symptoms, ethnic origin, nausea, and erythrocytes in the urine (STONE score) for the assessment of renal colic.15 An electronic version of the STONE score was created and made available to emergency physicians. Next, in May 2017, a separate electronic order was made for CT scans for renal colic. To adhere to recommended practice, the protocol for these scans was adjusted to use a lower dose of radiation. The CW recommendation was incorporated into this electronic order and emergency physicians were advised to order an ultrasound if patients met the CW criteria.
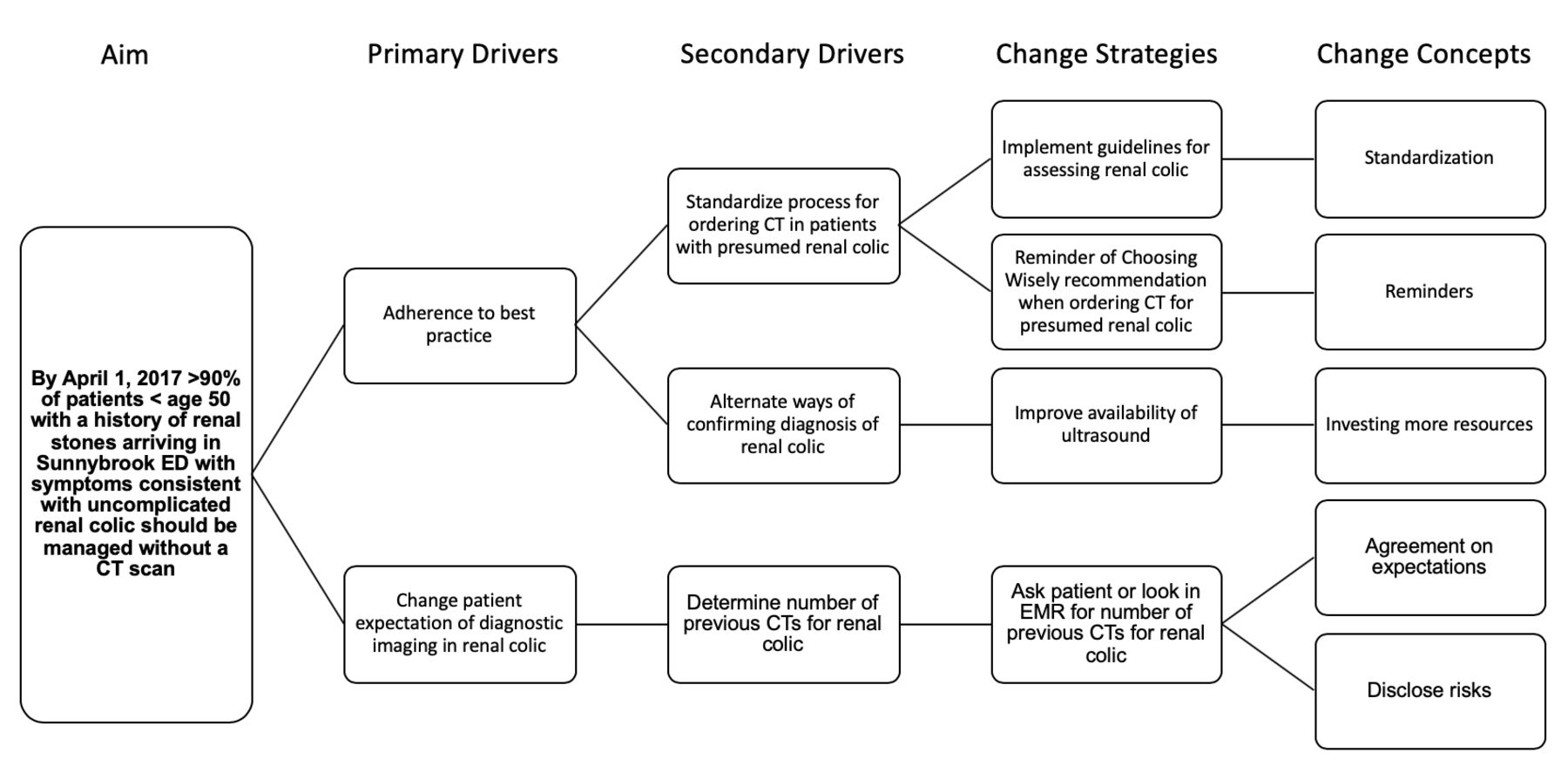
Key driver diagram. Generated with input from emergency physicians, a radiologist, a urologist and a clinical nurse educator. This diagram was used to provide a framework for the proposed aim, the critical factors needed to achieve change, and change strategies. ED, emergency department; EMR, electronic medical record.
Family of measures
The outcome measure was the number of CT scans ordered for those aged <50 years with a history of renal stones presenting with uncomplicated renal colic. The process measures were the number of ultrasounds ordered for the target population and the number of kidney-ureter-bladder X-rays ordered for the target population. The balancing measure was the number of patients diagnosed with renal colic that returned to the ED within 14 days with an alternate diagnosis.
Statistical analysis
Categorical data were reported as frequencies and proportions, whereas continuous variables were reported as medians with IQR. For comparison purposes, patients were divided by the type of imaging used to investigate their renal colic.
Results
Demographic features during audit period
Between 1 December 2015 and 31 May 2016, 130 patients under the age of 50 years visited our ED with a final diagnosis of renal colic. Of these, 63 had a history of renal colic and met our definition for uncomplicated renal colic on presentation. The number of files reviewed, the reasons for exclusion and the imaging modalities used for the study population are summarised in figure 2.

Flow diagram of included patients. KUB, abdominal X-ray to investigate the kidneys, ureters and bladder; US, ultrasonography.
The majority (47/63, 75%) of the patients were male and the median age was 36 years (IQR: 33–43). Nearly every patient presented with flank pain (62/63, 98%), often accompanied by nausea/vomiting (39/63, 62%), and sometimes gross haematuria (13/63, 21%). Many of the patients were returning to the ED for the second time within a month with ongoing symptoms of renal colic (22/63, 35%). There was no statistically significant difference in serum white blood cell count, creatinine, microhaematuria and pyuria for patients with and without CT imaging.
Management in the ED during audit period
Medications received by patients in the ED were documented as metrics for their expression of pain and nausea/vomiting. These findings show that a majority of patients received no medications for nausea or narcotic pain medications during their ED stay, however, most received ketorolac (44/69, 64%). Patients who received CT imaging received a median of 4 mEq of morphine (IQR: 0–10), while patients who did not undergo CT received a median of 0 mEq of morphine (IQR: 0–5).
Approximately 50% of the patients, both within the CT-imaged group and within the non-CT-imaged group, were referred to outpatient urology. None of the patients in either group were admitted to hospital.
Imaging appropriateness during the audit period
During the audit period, adherence in our ED for the CW recommendation to avoid CT imaging in patients under the age of 50 years presenting with uncomplicated, recurrent renal colic was 46/63 (73%). Many patients who met criteria for this recommendation had received multiple CT scans in the past for renal colic. 9.5% (6/63) of our patients had received a total of 3 or more CT scans specifically for renal colic. Notably, one patient had received 13 prior CT scans to investigate renal colic.
For patients who did not receive CT imaging, the alternative imaging modalities that were used are displayed in figure 2.
Imaging appropriateness during the QI period
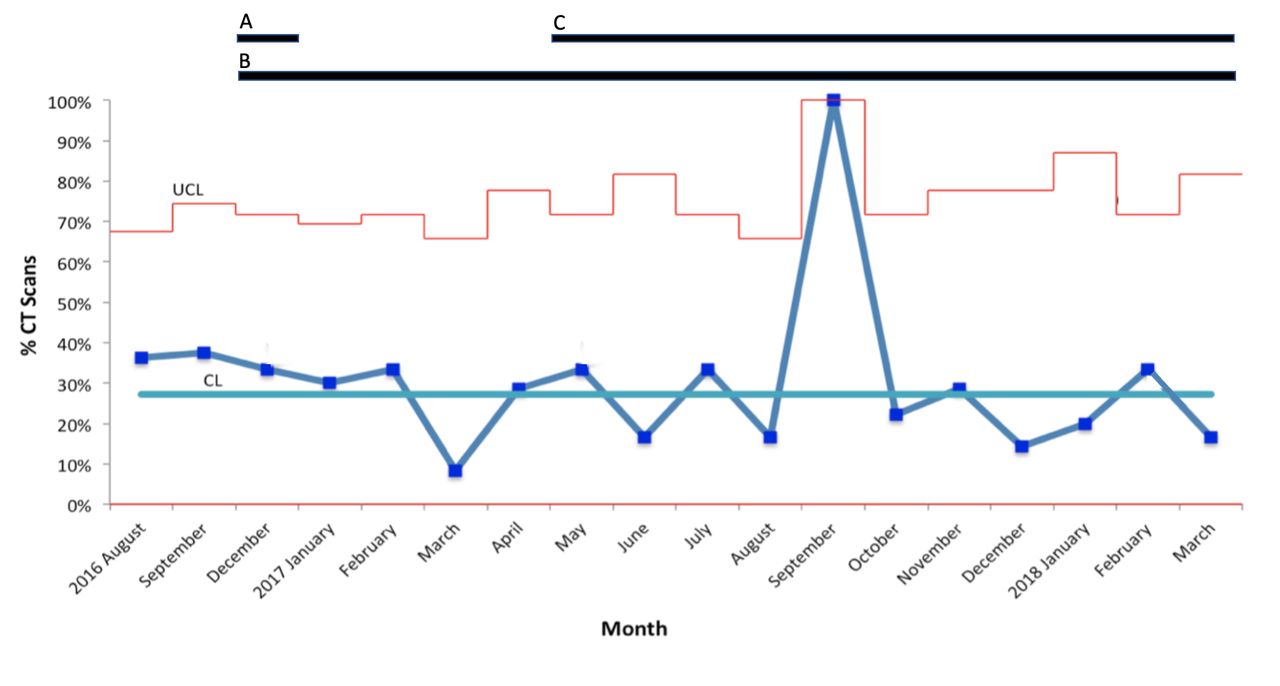
In the baseline audit from December 2015 to May 2016, 27% of individuals in our study population received unnecessary CT imaging. In the months before the QI project, however, the rates were higher at a baseline of 37%. Interventions were first implemented in December 2016 and then in May 2017. Over a 15-month period, utilisation of inappropriate CT imaging for these patients showed a modest decrease to 29%, displayed in figure 3. September 2017 was an aberrant month with 100% of patients in our study population receiving unnecessary CT imaging. This was due to a very low number of these patients presenting to the ED that month, and all had a CT scan. There was a corresponding increase in the utilisation of ultrasounds for patients with recurrent renal colic and no significant increase in the number of KUB X-rays performed. There were no patients diagnosed with renal colic that returned to the ED within 14 days with an alternate diagnosis.
{kind=link}
{kind=link}
{kind=link}
Percentage of cases of recurrent, uncomplicated renal colic inappropriately assessed by CT scan each month. The lettered black bars represent the various interventions throughout the quality improvement project and are described in further detail below. A: in December 2016, an educational campaign was conducted through individual interviews and a presentation at rounds informing about the choosing wisely recommendation; B: in December 2016, an electronic version of the STONE score was created and made available to emergency physicians to guide assessment of renal colic; C: in May 2017, a separate electronic order was created for low-dose CT scans for renal colic, including a prompt to remind clinicians of the CW recommendation. CL, control line; CW, choosing wisely; UCL, upper control limit.
Discussion
Our initial audit found that 27% of patients under the age of 50 years presenting with uncomplicated, recurrent renal colic received CT imaging, suggesting non-adherence with an ACEP CW recommendation. Importantly, none of the patients who received CT imaging during our audit period demonstrated significant findings warranting hospital admission or leading to identifiable changes in management plans in the ED. There was no significant difference in the proportion of patients referred to outpatient urology in either study group.
Our patient demographics and presenting complaints are similar to those reported in the literature, suggesting that our study population represented typical patients presenting to the ED with renal colic.2 16 Our audit did not have the statistical power to perform meaningful subgroup analyses, however, certain trends were noted. Patients who had presented to an ED with renal colic or flank pain in the last 30 days were less likely to undergo CT imaging during their second presentation. Presumably, on their initial visit, many of these patients had received imaging which was able to identify a stone, and were thus less likely to receive CT imaging at their return visit. It was also noted that the patient group that received CT imaging was given more narcotic analgesia, suggesting that the perceived severity of a patient’s pain may have also influenced the decision to order CT imaging.
The varied approach to diagnostic imaging of renal colic in our ED demonstrated by this audit is corroborated by other similar studies.11 Interestingly, a recent report released by the Canadian Institute for Health Information estimated that up to 30% of patients identified by CW Canada recommendations underwent unnecessary investigations.17 With 27% of our audit population receiving unnecessary imaging, we reached a similar figure.
Our QI initiative involved meeting with stakeholders, standardising a decision-making tool, implementing reminders on the electronic record, and creating a unique low-dose order for CT scans for renal colic. For the first intervention, a validated decision tool to guide treatment of suspected renal colic was introduced to clinicians and integrated into the EMR. This prediction tool, the STONE score, includes five factors which were found to be most predictive of urolithiasis: male sex, non-black race, short duration of pain (<6 hours), presence of nausea or vomiting, and microscopic haematuria.15 Moore et al recommend that CT imaging be avoided for patients who score high on this validated tool, and report it could help guide shared decision-making regarding imaging for renal colic.15 Unfortunately, during our study period, this decision-making tool was infrequently used by clinicians and therefore it was difficult to standardise CT ordering for presumed renal colic. Most physicians did not adopt regular use of this tool, preferring to rely on their own clinical judgement to determine the likelihood of renal colic. While use of this tool was available on an electronic platform that is regularly used during ED workflow, possible next steps could involve incorporating it into the EMR as a force function to encourage physicians to calculate a score and reconsider their imaging order as needed.
Our QI initiative faced several other challenges during implementation. A urologist was consulted as part of our team of stakeholders and had some concerns about the initiative, as it would result in more referrals to the urology service without CT imaging. These scans can be useful to urologists in clinic to help guide management decisions following an ED visit, and it required further discussions to get stakeholder buy-in. Through explanation of risks and benefits, and reviewing the literature around this specific presentation, our stakeholder team became more engaged with the goal of reducing the number of scans.
Although there was only a modest reduction in the number of CT scans ordered on young patients with recurrent renal colic, the greatest gain from this QI initiative was introduction of the ‘CT renal stone low dose’. It allowed a separate electronic order for a low-dose CT scan to be created, embedding the CW recommendation as a reminder and facilitated using the lowest dose of ionising radiation for patients with suspected renal colic. Usability testing was carried out on this new embedded order, and changes were made based on feedback. After integration into our EMR system, it took several weeks for physicians to consistently order the correct CT for presumed renal colic, instead of a full-dose CT scan of abdomen and pelvis. Adherence was monitored through audit and feedback was provided to clinicians. After this period, most physicians readily adapted to the new CT order for presumed renal colic, as it did not significantly alter their workflow. The data continue to show a modest decrease in the use of CT scans in patients aged <50 years with recurrent renal colic. Emergency physicians continue to consistently use the CT renal stone low-dose order when ordering a CT scan for suspected renal colic.
Across institutions, non-contrast abdominal and pelvic CT is currently used for ~80% of renal colic presentations due to its high sensitivity for urinary stone disease, as well as ease of availability in most EDs.18 However, even though CT imaging is often more sensitive than US, both modalities are effective in clinical practice. A prospective cohort study by Yan et al studying the use of ultrasound in the management of low-risk renal colic patients found that at 90-day follow-up, there were no significant intra-abdominal pathologies missed.19 In a multicentre study comparing US and CT imaging for suspected nephrolithiasis, Smith-Bindman et al found no significant differences in the risk of subsequent adverse events, pain scores, return ED visits or hospitalisations for the two groups.20 Furthermore, the use of US as the initial test resulted in no need for subsequent CT in most patients, thus resulting in lower cumulative radiation exposure for the US group. Other studies have also found that the use of US has similar patient outcomes as CT imaging, as the stones that are missed by US are usually small (<5 mm), and often pass spontaneously.12 18
Prior studies have shown that emergency physicians significantly underestimate the radiation exposure from CT and most physicians did not believe that CT increased the lifetime risk of cancer.21 This attitude can result in risks to patients, which is highlighted by one patient in our study who has undergone 13 CT scans for recurrent renal colic. Since urolithiasis is a recurrent disease and infrequently leads to long-term complications, emergency physicians should consider alternative diagnostic modalities to curb the amount of unnecessary radiation exposure. In particular, this should be considered in young patients with a history of renal colic with typical presentations.
Westphalen et al found that while there was a 10-fold increase in the utilisation of CT imaging for patients with renal colic from 1996 to 2007, there was no associated change in the proportion of diagnoses of kidney stones, significant alternate diagnoses or admissions to the hospital.11 These findings suggest that increased utilisation of CT imaging may not have a significant impact on the diagnosis and management of renal colic in the ED.
Despite low uptake during our initiative, the use of validated clinical decision-making tools and algorithms remain a useful resource in helping emergency physicians decide when to employ CT imaging for suspected urolithiasis. Dalziel et al proposed a prospectively validated algorithm for the use of point of care ultrasound (POCUS) for the management of renal colic in the ED.22 The algorithm uses hydronephrosis found on POCUS as the primary sign to guide the use of CT imaging. Kartal et al found that after using this algorithm, up to 50% of patients with renal colic in the ED could be discharged without further imaging other than US.23 The STONE score and POCUS are examples of evidence-based interventions to reduce CT use in patients with renal colic.
Our study has several limitations. First, given the nature of retrospective chart reviews, our initial audit is subject to documentation bias. We only included patients based on a discharge diagnosis of renal colic rather than a presenting complaint of flank pain. Emergency physicians may have considered a diagnosis of urolithiasis but an alternative discharge diagnosis may have been input into EDIS (eg, haematuria, back pain). Thus, it is possible that the study may have underestimated the number of patients receiving CT imaging for suspected renal colic. Nonetheless, we believe that our data abstraction methods were robust, as all study variables were defined a priori and a standardised data collection tool was developed. Finally, the generalisability of our study is limited given that this was a single centre audit with a small sample size. Further, practice will vary greatly at different centres based on local culture and awareness of CW initiatives. Despite this, our demographic results suggested a fairly representative patient population. Given previous studies, we expect that other jurisdictions would benefit from similar practice improvements.
Conclusion
In our large tertiary care centre ED, prior to a QI initiative, there was a 37% non-adherence to an evidence-based CW recommendation to decrease radiation exposure to young patients presenting with recurrent, uncomplicated renal colic. After implementation of conservative interventions, there was a modest reduction to 29% non-adherence. As a result of this QI initiative, there is less reflex in ordering CT scans on patients with renal colic. There is also awareness among emergency physicians of a patient population that is over imaged with CT scans, often with no change in management. Importantly, as a result of this project, there is a newly implemented low-dose CT order for renal colic patients.
Acknowledgments
Sunnybrook Health Sciences Centre Emergency Department and Emergency Physicians.
References
Footnotes
Contributors DS and JH designed the restrospective chart review. JH was responsible for data extraction and analysis of the chart review. DS designed and implemented the quality improvement initiative. DS was responsible for the data analysis of the quality improvement initiative. JH and AL were responsible for preparation of the manuscript. JH and DS are responsible for the overall content of the study.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.