Article Text

Abstract
Introduction Treatment escalation plans (TEPs) are important to ensure that every patient has their ceiling of care discussed and documented formally. At Medway Foundation Trust, we introduced TEP forms in September 2016 which are to be completed by the relevant consultant within 24 hours of admission.
Aims and methods To evaluate whether TEP forms had been effective at improving escalation planning and whether they had a subsequent impact in do not attempt cardiopulmonary resuscitation (DNACPR) decision-making. We carried out three plan-do-study-act cycles over a 2-year period across 100 patients in medicine and surgery.
Results TEP forms were initially found in 66% (66/100) of the patient notes and 34% (34/100) were completed appropriately. There was a 13% relative improvement in resuscitation decision-making, since the introduction of the TEP forms from November 2015 to January 2017. There was also a 12% reduction in inappropriate referrals to critical care during the same period. We decided to revise the TEP form through extensive collaboration and educate all staff members about the importance of escalation planning. This has led to an improvement in TEP discussion and documentation across the entire trust.
Conclusion TEPs can be an effective way of considering and communicating ceilings of care. They should encourage doctors to consider DNACPR decisions for patients who otherwise would not have been considered, and therefore may help reduce inappropriate referrals to critical care. The higher completion rates of the new form and increased clarity among staff regarding escalation planning should lead to an improvement in patient safety outcomes and communication between all patients and staff members. We believe it would be feasible to implement our user-friendly TEP form across other National Health Service organisations in order to develop a universal TEP form.
- communication
- critical care
- decision making
- patient-centred care
- quality improvement
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Appropriate escalation planning and resuscitation decision-making is essential to ensure effective patient management. These decisions should be made by experienced clinicians who fully understand the patient’s diagnosis and associated comorbidities, and can therefore make a balanced evaluation of what maximal level of treatment the patient would benefit from. The decision should be discussed with the patient and family.
At Medway Foundation Trust (MFT), an audit reviewing do not attempt cardiopulmonary resuscitation (DNACPR) decision-making in November 2015 and associated clinical incident reports, including recurrent inappropriate escalations to the intensive care unit (ICU), demonstrated a need to be more decisive with our DNACPR orders. We, thereby, introduced treatment escalation plan (TEP) forms for adult inpatients, located on the reverse side of DNACPR forms, in September 2016 as part of our Deteriorating Patient Programme (DPP) initiative.
TEPs aim to ensure that every patient has their ceiling of care considered early in their admission and documented formally. This gives the patient and members of staff confidence in the limits of treatment in the event of the patient deteriorating. They also help reduce unnecessary mobilisation of the cardiac arrest team and inappropriate referrals to the high-dependency unit or ICU. MFT guidelines require that TEP forms should be completed by the patient’s consultant within 24 hours of admission for all inpatients (except maternity, paediatrics and day-case surgeries) and attached to the front of the patient notes to allow for rapid identification in an emergency. As with many new changes, TEP forms at MFT did not come without reluctance to adopt this new initiative among staff members when they were first released. Criticisms included layout and wording of the form, along with poor staff engagement and communication.
Background
The National Confidential Enquiry into Patient Outcome and Death report ‘Time to Intervene’ (2012) highlighted that many patients are undergoing inappropriate resuscitation attempts, because DNACPR orders are not completed in a timely manner.1 In addition, a number of patients received attempted CPR in hospital despite having a recorded DNACPR decision, implying inadequate communication. There is also growing legal and ethical concern that decisions are often not discussed or communicated effectively to patients or relatives.2–4
Early decisions about DNACPR status and advanced planning on ceilings of care now form part of national recommendations by the UK Resuscitation Council (2016).5 There are currently national initiatives directed towards escalation planning, for example, Addendrooke’s Hospital in Cambridge developed the Universal Form of Treatment Options (2014) to focus on treatments to be given rather than withheld.6 The intention was to improve care for patients and address some of the problems associated with the DNACPR order. There is another national project called the Recommended Summary Plan for Emergency Care and Treatment campaign which hopes to ensure that dialogue between patient and clinicians is central to decision-making and that resuscitation decisions should be considered in the context of overall treatment plans.7 TEPs have generally been shown to be helpful in improving documentation on treatment escalation decisions and prompting discussion with patients and relatives.8 A universal escalation planning form is yet to be established.9 10
Aims
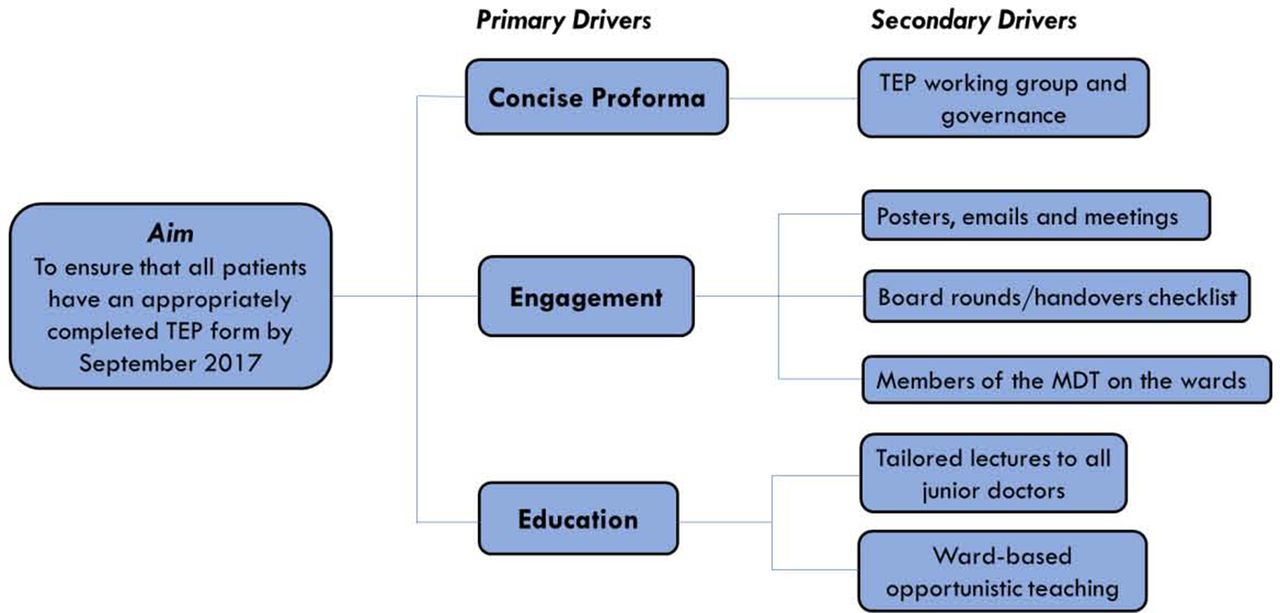
The aims of this project were to first introduce TEP forms trust-wide and measure their use and subsequent impact on DNACPR decision-making and referrals to critical care. We also measured adequacy of decisions, completeness of the forms, senior review, communication and patient demographics within each cycle. We carried out three plan-do-study-act (PDSA) cycles with the aim of achieving 100% TEP completion for all applicable patients by September 2017 (figure 1).

Driver diagram demonstrating the aim of the quality improvement project. This included developing a revised user-friendly TEP form as well as engaging and educating all staff members. MDT, multidisciplinary team; TEP, treatment escalation plan.
Strategy
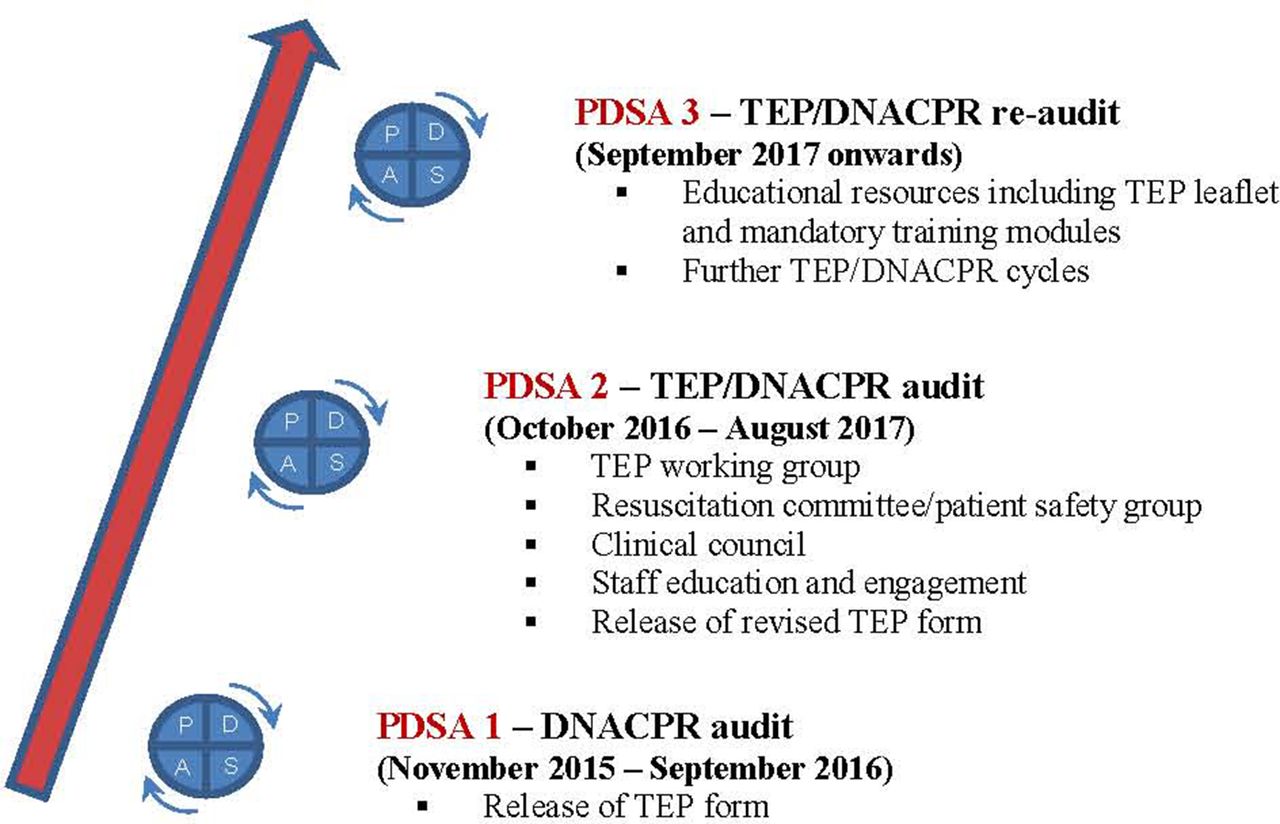
At MFT, we introduced the TEP form trust-wide using PDSA methodology. Three PDSA cycles carried out between November 2015 and September 2017 were used to develop and revise the TEP form (figure 2). The outcome measures of this project were the percentage of patients who had a correctly completed TEP form in their notes, percentage of appropriate DNACPR forms and the rate of inappropriate ICU referral. Our exclusion criteria for all three cycles were maternity, paediatrics, admissions less than 24 hours and day-case surgeries.

Plan-do-study-act (PDSA) cycle time course and highlights. DNACPR, do not attempt cardiopulmonary resuscitation; TEP, treatment escalation plan.
PDSA cycle 1
Consisted of a baseline audit of DNACPR decisions in the trust. In November 2015, we undertook a review of 100 inpatients (mean age 84.4 years; range 58–97 years) across two medical and surgical wards at MFT. Baseline demographics were obtained including assigning a performance status to each patient according to the World Health Organisation (WHO) classification (0=fully active, 4=severe comorbidities at risk of death).11 If there was a valid DNACPR decision in place, we asked the nurses if they were aware of the decision. We also identified which of the patients should have had a DNACPR decision but this had not been made. This was achieved through the help of senior clinicians (medical and surgical consultants) reviewing the patient notes, including comorbidities, performance status and any pre-existing documentation around escalation planning. The results of this cycle led to the development and release of the first TEP form across MFT in September 2016.
PDSA cycle 2
Studied whether introduction of TEPs had been effective at improving quantity and quality of escalation planning for patients and if this had led to a subsequent improvement in DNACPR decision-making, documentation and communication.
In January 2017, we analysed notes of 100 inpatients (mean age 71.9 years; range 18–97 years) across the same medical and surgical wards. Alongside demographics and performance status, we identified if there was a valid TEP or DNACPR decision in place, if it was clearly identifiable in the notes and signed by a consultant within 24 hours of admission. Of the patients who had a valid DNACPR, we checked that the staff nurses were aware. We determined which of the patients should have had a TEP±DNACPR decision and did not. In addition, review of clinical incident reports and ICU data facilitated identification of numbers of patients inappropriately escalated to critical care.
After extensive feedback from a spectrum of staff at MFT including the Resuscitation Committee, the TEP form was revised (figure 3A,B). Our intention was to develop a new more concise and user-friendly form that suits all specialties. We have simplified the escalation format. A list of potential indicators for poor prognosis has been added to act as a guide for doctors completing the form. In addition, a ‘specific discussions’ box has been included for discussions with patients and family or specific instructions on escalation plans for more complex cases. We hoped this will encourage doctors to hold conversations with patients and relatives in order to understand their wishes and concerns. The policy was changed to ensure that every patient undergoing trauma or emergency surgery at MFT must have a TEP in place.
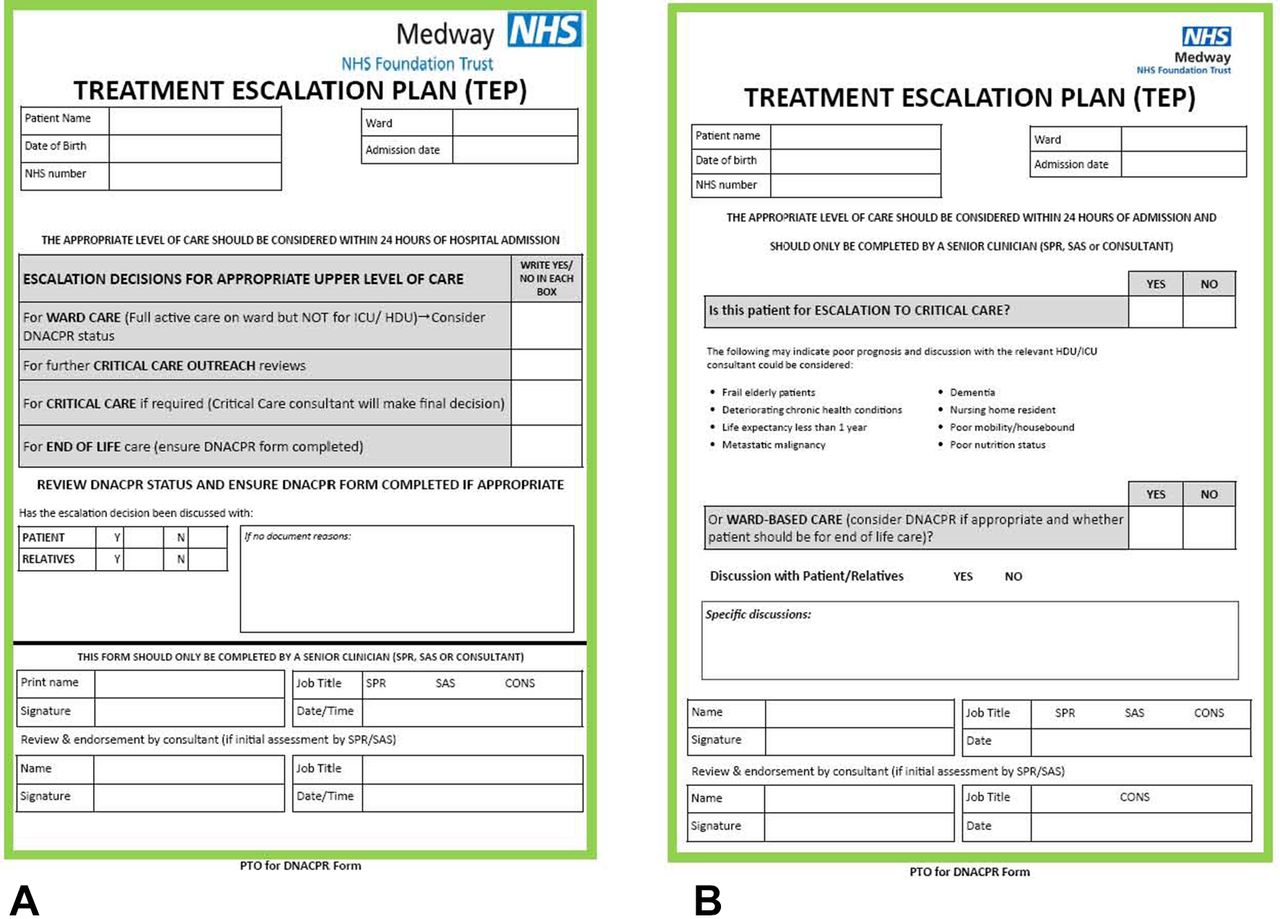
(A) The initial treatment escalation plan form and (B) the revised form developed with our group of critical care, medical and surgical consultants released in August 2017. CONS, consultant; DNACPR, do not attempt cardiopulmonary resuscitation; HDU, high-dependency unit; ICU, intensive care unit; NHS, National Health Service; SAS, specialty and associate specialist registrar; SPR, specialist registrar; PTO, page turn over.
The revised, more concise form was released in August 2017 through input from our multidisciplinary TEP working group. We improved engagement and education through TEP posters in clinical areas and a large communications campaign championed and cascaded by key consultants in the trust.
PDSA cycle 3
Commenced in September 2017 after introduction of the revised TEP form. We studied 100 inpatients (mean age 62.5 years; range 18–93 years) on the same surgical and medical wards as the previous two cycles in order to look for improvement in TEP and DNACPR decision-making, appropriateness, review and communication. This was accompanied by the new form being highlighted on the MFT intranet and a video demonstrating the importance of resuscitation decision-making, documentation and communication. This will be incorporated into resuscitation training at MFT. A mandatory training module for escalation planning for staff and an information leaflet on TEP for patients have also been made available.
Results
Table 1 summarises the patient demographics, WHO performance status, TEP form and DNACPR form completion rates across all three PDSA cycles. During PDSA cycle 1, 32% (11/34) of DNACPR decisions were made in the community, 62% (21/34) were made on admission (within 24 hours) and 6% (2/34) were made later following ward round review. Ninety-four per cent (30/32) of staff members were aware of the DNACPR decisions in place. We also highlighted 20% (20/100) of patients who should have had a DNACPR decision but did not have one in place. A review of the monthly ICU mortality group minutes revealed that 29% (31/101) of patients were retrospectively determined as inappropriately escalated to ICU. This has a major impact on ICU resources and we could improve our ability to care for patients who are more likely to benefit from critical care if there was a reduction in the number of inappropriate referrals.
The patient demographics, WHO performance status (0=fully active, 4=severe comorbidities at risk of death), TEP form and DNACPR form completion rates for each PDSA cycle
Over PDSA cycle 2, TEP forms were found in 66% (66/100) of the patient notes (43% located in front of the notes) and 34% (34/100) were completed. Of those completed, 68% (23/34) of the forms were done so within 24 hours and 50% (17/34) were signed by a consultant. Thirty-two per cent (11/34) of completed forms involved a discussion with patients or relatives.
Twenty-two per cent (4/18), 26% (5/19) and 30% (7/24) of patients had an appropriately completed TEP form with a performance status of 0, 1 and 2, respectively. Thirty-nine per cent (7/18) of patients with a performance status of 3 had a TEP form completed with 33% (6/18) of these patients having a completed DNACPR. Sixty per cent (9/15) of patients with a performance status of 4 had a TEP form completed with 73% (11/15) having a completed DNACPR form. Patients with a poorer performance status are generally seen to have higher TEP and DNACPR completion rates (table 2).
The number and percentage of patients with a completed TEP and DNACPR form according to their WHO performance status for each PDSA cycle
Seventeen per cent (3/18) of DNACPR decisions were made in the community, 77% (14/18) of DNACPR decisions were made on admission and 6% (1/18) were made later following review. We noted a greater percentage of DNACPR decisions made on admission following the introduction of TEP forms. We also identified 7% (7/100) of patients who should have had a DNACPR decision but did not have one in place. This was a 13% relative improvement compared with cycle 1. DNACPR documentation rates of the individual sections on the form scored higher in all areas, other than communication with patients (79% in cycle 1 vs 50% in cycle 2) and relatives (94% in cycle 1 vs 67% in cycle 2). One hundred per cent (32/32) of staff members asked were aware of DNACPR decisions.
The main errors found associated with the TEP forms included incorrect escalation plans, conflicting TEP forms found in the notes, difficulty in finding the form in the notes, lack of discussion with patients/relatives and no consultant sign-off. An example of an incorrectly filled in TEP form included one patient who was for both escalation to critical care and ward-based care with no discussion with the patient or family members.
Six clinical incident reports were found, over cycle 2, demonstrating a lack of TEP or DNACPR documentation. Inappropriate escalation of care in dying patients can result in significant stress on the patient, staff and family. They also highlighted unnecessary mobilisation of the cardiac arrest team due to poor TEP and DNACPR documentation. Another review of the monthly ICU mortality group minutes indicated 17% (16/95) of patients were retrospectively deemed as inappropriately escalated to ICU. We believe the introduction of TEP forms may have helped decrease the number of inappropriate referrals to ICU in cycle 2.
During PDSA cycle 3, the revised TEP form was found in 83% (83/100) of the patient notes (51% located in the front of the notes) and 56% (56/100) were completed. Of those completed, 70% (39/56) of the forms were done so within 24 hours and 45% (25/56) were signed by a consultant. 50% (28/56) of completed forms involved a discussion with patients or relatives. Table 2 generally shows that there was a greater percentage of TEP forms being completed across all performance statuses during this cycle. Overall, there was an increase in the revised TEP forms being found in the notes and being completed. Fewer errors were being made and there was a rise in patient/relatives discussion that were taking place and being documented (figure 4A,B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) The percentage of initial and revised TEP forms found in the patient notes and completed. (B) The percentage of initial and revised TEP forms, of those completed, signed by a consultant in 24 hours with documentation of patient/relative discussion. TEP, treatment escalation plan.
Lessons and limitations
This project demonstrated that improving resuscitation decisions is a trust-wide initiative and requires extensive engagement at every level. Revision and release of the new TEP form was an intensive process that involved excellent communication, feedback and review.
Limitations of this project included the communication we had at the outset was reduced somewhat after the DPP which championed this project was dismantled. For PDSA cycle 2 and 3, we no longer had a project manager which made it more labour-intensive. We also attempted to identify patients who should have had a DNACPR decision made but did not have one in place. However, DNACPR decision-making can clearly be affected by differing clinician views and perspectives, as well as the number of unwell patients there were present in each cycle at that particular time. We tried to overcome this by assessing and recording the performance status of each patient for all three cycles. In addition, despite trying to gain full engagement of clinicians, some continued to be reluctant to make these key decisions and we feel that this is representative of what occurs nationally.
Conclusion
TEPs can be an effective way of formalising timely clinician decision-making and communicating ceilings of care for patients and have now become a national initiative. A correctly documented TEP form is an important resource for both the medical and surgical team, particularly in the case of a deteriorating patient in the acute setting. This quality improvement project has increased the use of TEP forms. We believe this had a positive impact on appropriate DNACPR decision-making and documentation, as they helped to remind doctors to consider the escalation plans for their patients. In particular, there was also a noticeable increase in the proportion of escalation plans that had been discussed with patients or relatives. Although, TEPs have improved awareness and decision-making in our trust regarding ceilings of care, we still have not yet achieved our goal of 100% TEP completion.
Engagement and education of our senior decision-makers is key. Some of our senior staff continue to be reluctant to make these important decisions and we have focused on education and communication in order to improve this. We are targeting junior doctors’ teaching and induction to emphasise the importance of resuscitation decisions and to escalate to their seniors. Increasingly, hospitals are looking to the community and general practitioners to hold these conversations with their patients prior to being admitted to hospital and this is what we plan as the next cycle of this project. We need to ensure decisions made in the community are adequately communicated to the hospital staff if patients are admitted and electronic databases that are accessible from within the hospital would facilitate this. We also plan on training our senior nurses to be able to identify patients at risk and highlight them to the team.
Acknowledgments
The team would like to thank our TEP working group of consultants which included
Brian Andrews, Sandip Banerjee, Kolera Chengappa, Gihan Hettiarachchi, William Ogburn and Graeme Sanders. We would also like to thank a group of medical students who helped with data collection following the release of the revised TEP form.
Footnotes
Contributors MGF designed and led the audit cycles, collected and analysed and the data, and performed the write-up. KP took part in the audit cycles and helped with collecting and analysing the data. PH supported the data analysis and reviewing of the manuscript. PK supervised the audit cycles, helped with analysing and presenting the work and writing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.