Article Text

Abstract
Background The implementation and continuous improvement of patient safety learning systems (PSLS) is a principal strategy for mitigating preventable harm to patients. Although substantial efforts have sought to improve these systems, there is a need to more comprehensively understand critical success factors. This study aims to summarise the barriers and facilitators perceived by hospital staff and physicians to influence the reporting, analysis, learning and feedback within PSLS in hospitals.
Methods We performed a systematic review and meta-synthesis by searching MEDLINE (Ovid), EMBASE (Ovid), CINAHL, Scopus and Web of Science. We included English-language manuscripts of qualitative studies evaluating effectiveness of the PSLS and excluded studies evaluating specific individual adverse events, such as systems for tracking only medication side effects, for example. We followed the Joanna Briggs Institute methodology for qualitative systematic reviews.
Results We extracted data from 22 studies, after screening 2475 for inclusion/exclusion criteria. The included studies focused on reporting aspects of the PSLS, however, there were important barriers and facilitators across the analysis, learning and feedback phases. We identified the following barriers for effective use of PSLS: inadequate organisational support with shortage of resources, lack of training, weak safety culture, lack of accountability, defective policies, blame and a punitive environment, complex system, lack of experience and lack of feedback. We identified the following enabling factors: continuous training, a balance between accountability and responsibility, leaders as role models, anonymous reporting, user-friendly systems, well-structured analysis teams, tangible improvement.
Conclusion Multiple barriers and facilitators to uptake of PSLS exist. These factors should be considered by decision makers seeking to enhance the impact of PSLS.
Ethics and dissemination No formal ethical approval or consent were required as no primary data were collected.
- Healthcare quality improvement
- Incident reporting
- Medication safety
- Near miss
- Patient safety
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patient safety learning systems (PSLSs) are viewed as an important tool for improving the quality and outcomes of hospital-based care.
WHAT THIS STUDY ADDS
This review identifies barriers and facilitators for different stages of system implementation.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our findings can inform decision makers in establishing or improving their PSLS. Further research can build on these results.
Background
Patient safety learning systems (PSLSs) support healthcare staff in documenting patient safety events and concerns, facilitate immediate corrective actions including communication, and promote the learning and improvement required to prevent future similar occurrences.1 Use of PSLS involves four related and sequential efforts2: (1) structured reporting, (2) collation of data, (3) analysis and (4) learning from the reported incident.3 In their 1999 report, the Institute of Medicine strongly recommended the use of incident reporting as a means to improve patient safety.
The success of PSLS in improving patient safety is debatable,4 as errors and adverse events continue to occur in all healthcare settings. It is also important to note that using percentage of reported incidents as a measure of improvement after implementing PSLS might be unreliable as the true number of incidents (the denominator) is unknown because of under-reporting.4 Although there are no published reports demonstrating a reduction in adverse events, many studies have evaluated the adoption of PSLS.5 These studies identified factors associated with improving the use of PSLS, but tended to focus on the reporting of events rather than the factors improving the downstream actions of analysis and learning. As these later steps are the actions that will lead to improved safety, it is important that they are addressed in efforts to improve PSLS.1 To address this potential gap, we conducted a systematic review to identify the perceived barriers and facilitators for effective PSLS adoption in hospital settings. We assessed factors related to all phases of PSLS, not just the reporting of events. A fulsome description of all aspects of PSLS will help design future studies, support our understanding of ways to improve the effectiveness of PSLS, and enable hospitals and health systems to assess their own efforts. To guide our qualitative evaluation, we meta-characterised factors based on the Patient Safety Toolkit developed by the Canadian Patient Safety Institute (CPSI) (figure 1).6

Shows the different steps in the patient safety management toolkit developed by the CPSI (5). CPSI, Canadian Patient Safety Institute.
Methods
To synthesise the large array of qualitative findings in the literature, we first identified an overarching conceptual framework for safety reporting and response; then we mapped the factors related to the barriers and facilitators to this framework. This inductive approach resulted in the development of emerging themes. A protocol was registered a priori (CRD42021220504).7
Search strategy
An experienced medical librarian (LS) was consulted to develop a search strategy. The strategy was piloted in MEDLINE (Ovid), and then translated to include EMBASE (Ovid), CINAHL, Scopus and Web of Science. We manually searched Google Scholar, Grey Literature Reports, the CPSI and the WHO for unpublished studies. The multifield search query we used in our study is shown in online supplemental appendix 1.
Supplemental material
We used the PICO approach (suited to qualitative systematic reviews and meta-synthesis) for selecting our primary studies.8 The participants in these studies were healthcare professionals, quality and safety experts. According to the criteria discussed below, we included qualitative studies that investigated the problem of the continuous occurrence of patient safety incidents and the factors perceived to be responsible for ineffective PSLS.
Inclusion criteria
Studies published in English and discussing the perceived barriers and/or facilitators to the use of PSLS in hospitals were included. No restrictions on the type of incidents, demographic or geographical areas, sampling, or type of participant were applied.
Exclusion criteria
We excluded studies that evaluated the effectiveness of PSLS, those focused on a single incident and those examining the effect of a specific factor on PSLS. Studies investigating the criteria for reporting incidents and the trends in doing so were also excluded.
Study screening and selection
Two reviewers (HAM and MAA) independently screened the titles, abstracts and full text (in that sequence) of citations using Covidence software.9 Any disagreement between the two reviewers was resolved through discussion with a third reviewer (AAM).
Data extraction
Data were extracted into an Excel spreadsheet for analysis, including the following data points: study characteristics (authors, year of publication, journal); methodology (design, research purpose and/or questions, method of analysis); participant characteristics; country in which the study took place; setting; population descriptors; sample size; barriers, facilitators and conclusions reported. We used the qualitative assessment and review instrument for qualitative data extraction tool from the Joanna Briggs Institute (see online supplemental appendix 2).10 Data were extracted by one reviewer (HAM), and the second (MAA) verified the extracted data. Disagreements were resolved through discussion with a third reviewer (AAM).
Assessment of methodological quality
The purpose of assessing methodological quality for qualitative research is to describe the overall robustness and validity of the findings. It is not to be used to weight results or support the exclusion of studies as it is possible to find important themes from research with relatively weak designs. We; therefore, assessed quality using the Critical Appraisal Skills Programme (CASP) Qualitative Checklist (see online supplemental appendix 3: CASP Qualitative Checklist) by two independent reviewers (HAM and MAA), and any disagreement was resolved through discussion with a third researcher (AAM). However, this process did not lead to any studies being excluded from the analysis.
Guiding framework
The Patient Safety Toolkit6 is derived from the best available evidence and expert advice, and can be tailored for any healthcare setting. As such, we thought it might help us identify barriers to the success of PSLS, and used it as a framework for summarising our findings. This framework is comprehensive in that as well as including the four steps of PSLS, it describes other aspects expected to influence the effectiveness of such systems, for example, those ‘before the incident’, which include the organisational culture that encourages reporting and the support from the leadership. The incident management domain within the tool was used to develop our themes and subthemes.
Data synthesis
Two reviewers (HAM and MAA) reviewed all articles to retrieve data describing the participants, study characteristics, and perceived barriers and facilitators. Directed analysis was done, including identification and classification of extracted factors (barriers and/or facilitators), and assigning factors to themes and subthemes according to the CPSI Patient Safety Toolkit. These data were entered into separate spreadsheets. The results from the two reviewers were compared and differences were resolved by consensus with a third reviewer (AAM). We then counted the number of factors identified within each subtheme to inform our narrative synthesis. After removing duplicates, these factors were analysed, merged and new definitions were developed. In the present report, the resulting synthesised factors are narrated and tabulated as a set of main findings.11
Results
Study inclusion
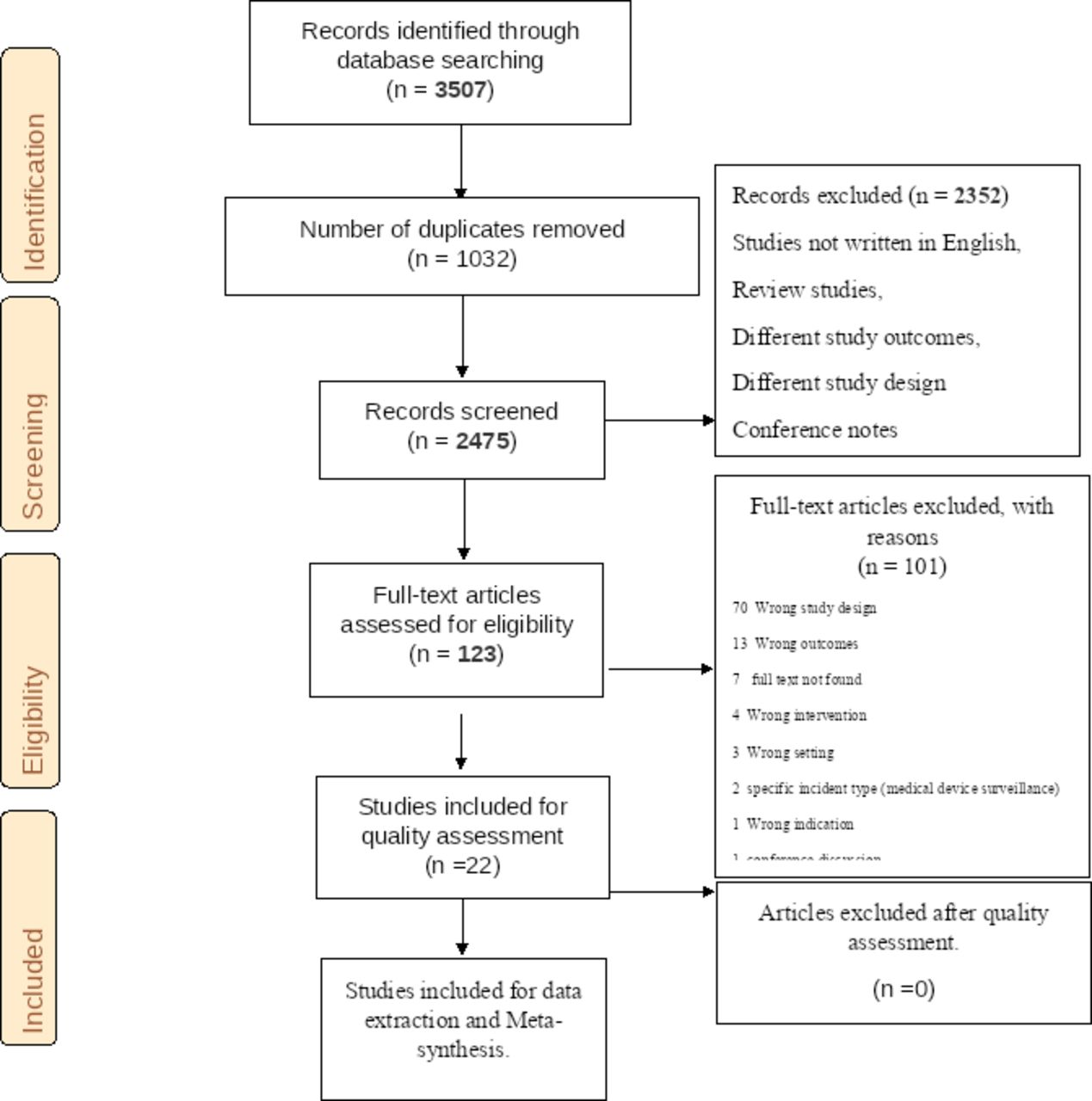
A total of 3507 studies were identified from searched databases on 1 February 2021, leaving 2475 studies for title and abstract screening after removal of 1032 duplicates (figure 2). Of these, 2352 studies were excluded according to the following criteria: the language was not English, review articles or having different study designs or outcomes. After assessment of the full texts, a further 101 articles were excluded: different study design (70 articles), different outcome (13 articles), full text was not found (7), different intervention (4) or setting (3), specific incident type (2), different indication (1) and conference report (1). After this exclusion process, we included 22 full-text articles.

{kind=link}
{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2009 flow diagram.
Study characteristics
All studies included were published in 2010–2021, except for three.12–14 Five were conducted in England,13 15–18 two in Australia,12 14 Canada,19 20 the USA,21 22 Brazil,23 24 and Iran,25 26 and one in the Netherlands,27 UAE,28 Sweden,29 Turkey,30 Qatar,31 and South Korea.32 One included study was multinational.33
No data were provided regarding the sex, age or work experience of any of the participants. Participants in the 22 included studies were 781 healthcare professionals including 359 nurses from different medical, intensive care and surgical departments, 190 physicians, 49 pharmacists, 42 quality and safety managers, and 5 allied health professionals. The profession of the remaining 136 participants were not mentioned in three of the studies.17 23 24 Studies were conducted in intensive care units,12 teaching hospitals,15 20 23 27 30 university hospitals,25 tertiary hospitals,22 31 32 large general public or community hospitals13 14 17–19 24 29 31 and children’s hospitals21; 1 of the studies involved participants from 111 hospitals.26
In relation to sampling, eight studies used a purposive sampling technique14 15 18 21 28–30 33; two studies used purposive sampling and snowball sampling20 31; four studies used invitation letters22 24 25 27; the researchers of one study sought out their acquaintances by posting advertisements and using snowball sampling techniques32; one study used posters and nurse leader appeal in selecting their participants12; one study involved all nurses until saturation occurred23; four studies did not clearly describe their sampling methods.16 17 19 26
Assessment of methodological quality
All of the included studies clearly described how they were conducted, but eight articles failed to clarify the researchers’ relationships to the participants (table 1).12 13 19 20 22 23 29 31 In relation to sampling, 11 of the 22 studies carried a risk of selection bias (the researchers selected their participants) and/or a risk of non-representative sampling.12 16 18 19 21–23 25 26 31 32 One study included only less-experienced residents.22 Two studies did not report how data saturation was defined or achieved.16 22 There was no weight to specific questions nor a scoring system for the CASP Qualitative Checklist. As qualitative studies, we included all primary studies regardless of the quality of their methodology, as even methodologically sound studies can be poorly interpreted thereby offering insufficient insight in a particular topic; conversely, studies of lower quality may provide new insights. This heterogeneity contributed to the interpretation of the overall findings.34
A summary of the overall methodological quality of the included studies
Summary of study findings
We extracted 375 reported factors from the 22 studies, all of which were either unequivocal or credible based on the participants’ verbatim transcripts and researcher experience.
Six themes and 16 subthemes were developed based on the Patient Safety Toolkit and are outlined below and in table 2. Factors under the theme ‘immediate response’ were the most cited as perceived barriers to improving PSLS, cited 170 times out of 375 reported factors (45.3%). Its subthemes ‘reporting the incident’, ‘secure items for confidentiality’ and ‘care for reporter’ were cited 98, 41 and 31 times, respectively. The theme ‘factors before the incident’ was cited 134 times (35.7%) and included subthemes ‘training’ (46 times), ‘organisational and leadership support’ (39 times), ‘cultivate just and safe culture’ (28 times), and ‘availability of resources’ (21 times). Other factors were reported less frequently, however, this does not necessarily reflect lesser importance, as all of the included studies were more focused on reporting procedures of the PSLS and less on the subsequent steps.
Identified themes and subthemes based on the CPSI safety tool kit and their proportions
Theme 1: before the incident (n=134)
Subtheme 1.1: training
Training was examined by 16 studies,13–15 19–28 30 32 33 which identified a ‘lack of training’—for both reporters and managers—as a major barrier (46 of 134 responses, 34.3%). Facilitators included planning for and implementation of continuous training, which should be effectively communicated to staff and managers.
Subtheme 1.2: organisational and leadership support
Factors related to organisational and leadership support were mentioned 39 times (29.1%) and included: lack of accountability that would make staff feel more responsible; ineffective reporting systems19 20 24 25 33; lack of definitions, policies or standards14 18 19 21 26 32; poor communication19 26; negative responses to reporting by leaders13 18 22 26 27 30–32; lack of authority25 and role models.32 Related facilitators included: incentives and initiatives to report more31; professional accountability and supportive atmospheres19 20 25 28 29 33; writing and dissemination of a guiding manual; increased confidentiality and security of the reporting process14; motivate staff to report through the display of posters27; eliminating blame by seniors or doctors.29 30
Subtheme 1.3: cultivate a just and safe culture
This subtheme was cited 28 times (20.9%). Barriers included a blaming and punitive culture14 18 21–23 25 32; an attitude of the administration for personalising errors27 30; a lack of awareness about safety culture, which subsequently fostered a lack of responsibility and undervaluing the reporting system14 30; a defective culture unwilling to accept responsibility for errors25; a culture of low expectations, for example, ‘Well they’re in a hospital and things happen’.22 Facilitators included balancing the need for responsibility and accountability15; building trust in a non-punitive system attained by supporting the reporters, promoting peer reporting, anonymous reporting to an independent body20 29 31; belief that this promotes patient protection19; stimulating role of superiors.27
Subtheme 1.4: availability of resources
Reported 21 times (15.7%), this subtheme comprised the following barriers: manual reporting systems or defective electronic systems can be time-consuming18; shortage of time and equipment for reporting.14–16 18 19 21 22 25 26 29 32 Facilitators included carrying a pocket-size plasticised card that outlines the reporting process27; electronic systems together with human and financial resources18 28 29; the option of faster reporting processes (eg, telephone reporting).14
Theme 2: immediate response to the incident (n=170)
Subtheme 2.1: reporting the incident
Factors in this subtheme were reported 98 times (57.6%) and were classified further into three categories: ‘user friendly’ (reported 37 times, 37.8%), ‘external and internal reporter influencers’ (32 times, 32.7%) and ‘incident related factors’ (29 times, 29.6%).
Under the ‘user friendly’ category, participants reported the following barriers: complex systems and forms asking for unnecessary data13 14 16 18 19 22 24 27–30 33; poor quality of the incident report15; reporting is time-consuming12 16 19 25 27 29 32; limited access to forms29; the extra work burden on the reporter19 27 32; duplication of work being registered in patient files and in the PSLS or rereporting by other staff.18 22 24 Facilitators included profession-specific forms14 18; forms that balance the amount of information requested with time.18 19 27 29
A second category is ‘internal and external influencers to report’, which included the following barriers: juniors are afraid to report seniors’ errors; seniors preventing juniors from reporting; the norm that doctors never report but nurses should12 18 20 28; avoiding reports that might cause internal disputes12 18 19 22 25 28 32; negative attitudes to reporting (eg, it is ‘a waste of time’)27 29 32; reporting yields a feeling of failure12; the perception that reporting brings no personal benefit12 19 25; non-mandatory reporting19 20 25; a lack of perceived ability to report or that staff simply do not think of reporting27 or consider errors a normal part of daily events.30 Facilitators included a belief in learning from errors,20 that this benefits patients19 25 and showing commitment to adhering to policies.19
A third category, ‘incident related factors’, includes ‘seriousness of incidents regarding impact, consequences, severity and frequency’, that is, the more serious incidents are more likely to be reported, whereas near misses are perceived to have less chance of being reported12 18–25 27 29 30 32 33; no clear cause for the error.24 The facilitators included: focusing on reporting serious prioritised incidents, which allows better analysis and management18 29; errors with serious consequences and high frequency of occurrence influence reporting.25 32
Subtheme 2.2: care for and support for reporter
This subtheme was mentioned 31 times (18.2%) in the primary studies, 25 of which described barriers, including: ‘reporters feel worse, guilt, shame, uncertainty, disloyal to colleagues and emotionally charged’; a lack of a supporting manager12 13 18 21 22 24 27 30 32; the feeling that reporting the error might cause loss of honour, respect, reputation and dignity along with perceived incompetence19–21 25; inappropriate responses by managers.21 25 Six facilitators included protecting reporters against legal and non-legal actions.14 19
Subtheme 2.3: confidentiality
This subtheme was reported 41 times (24.1%) and some barriers were directly related to ‘breach of confidentiality that might cause loss of reputation, career, relationships, friendships and respect’12 13 15 16 19 20 28 30; ‘fear of blame or punishment or legal action’12 13 16 19 20 22 25–27 29 30; ‘lack of anonymity and lack of trust in system confidentiality’18–20 22 25 32; ‘fear of economic losses’.25 Confidentiality and anonymous reporting to independent bodies have been repeatedly reported as positive system influencer.18 21 27 31
Theme 3: prepare for analysis
Subtheme 3.1: preliminary investigation
Factors related to preliminary investigations were mentioned five times and were all barriers such as lack of time and resources15 and poor communication.18 Furthermore, anonymity was cited as making information about the incident more difficult to obtain.17 32
Subtheme 3.2: identify team
Factors related to ‘identify team’ were cited six times, and included the following barriers: lack of front-line engagement15; complex organisations, in which it is difficult to assemble the appropriate team15 17; lack of cooperation between units related to the incident.29 Building fully representative teams was reported as an aspect that might improve PSLS.31
Subtheme 3.3: plan for interview
In thinking about planning for incident-related interviews, participants only reported fearing loss of reputation as a barrier for participation.17
Theme 4: analysis process
Subtheme 4.1: investigate what happened
One barrier and four facilitators were related to investigation: mass reporting might interfere with accurate analysis and capacity for learning33; ‘multidisciplinary meetings ensure equal and fair participation’17; applying tools and analytical approaches, avoiding analytical myopia,15 17 and to have open communication.31
Subtheme 4.2: understand why and how it happened
This subtheme was represented only by one facilitator of PSLS: use of proper analysis tools.18
Subtheme 4.3: develop and manage recommendations
Factors in this subtheme were reported six times, including poor-quality recommendations such as ‘too much details or too simple’,15 contradictions with other change agendas and initiatives.17 ‘Avoid giving undue attention to the report’17 was reported as a facilitator.
Theme 5: follow through
Subtheme 5.1: implement
Reported 11 times, this subtheme includes a lack of effective measures that make tangible changes22 24 27 29 and also time-consuming recommendations,29 difficult to implement recommendations,32 existence of plans that contradict recommendations.26 Visible change was reported as a facilitator.18
Subtheme 5.2: follow and assess
Factors in this subtheme were reported five times, four of which were facilitators. Two of these were the use of risk-assessment tools to prioritise actions for follow-up14 and formal (eg, targets, audits and score cards) and informal (keeping on meeting agenda, management oversight, risk officer spot-checks) performance management for evaluating changes.15 Only one barrier was reported under this subtheme: data processing does not reflect the real number of reports due to under-reporting.23
Theme 6: close the loop
This theme was reported 31 times (8.3%) and includes only one subtheme ‘share learning internally and externally’. The barriers are lack or defective feedback resulting in loss of trust in the system.12–14 16 22 24 26–28 32 Facilitators include: feedback mechanisms that motivate reporting15 18 19 29; improving error-related communication from senior management to healthcare professionals19; to ‘definitely collect less data of better quality of learning and feedback’; to ‘share learning horizontally (with peers), and also for vertical accountability’33; transparency in sharing data21; the type and timing of feedback depend on the severity of the incident or the degree of risk to the organisation; individual and group feedback about action taken will increase trust in the system.14
Discussion
In this systematic review, we identified all barriers and facilitators reported in the literature for PSLS. In those studies, recommendations were reported by participants encountering such barriers. The results also revealed the participants’ perceptions of how these barriers might prevent improvement of the system. By including all the aforementioned factors and recommendations, managers and other decision makers have a wide range of options for taking innovative actions to improve their safety systems.
We included 22 primary studies. We sorted the reported factors (barriers and facilitators) into themes based on a framework derived from the CPSI Patient Safety Toolkit. Facilitators and barriers related to ‘before the incident’ included the preparedness of a hospital to implement PSLS through planning, training, assignment of resources, a well-established safety culture that focuses on systems not people and ensures top-level commitment and support, and well-developed policies and procedures. Related to ‘the immediate response’, some studies recommended that hospitals support reporters emotionally and against legal action. Factors related to ‘analysis process’ and ‘follow through’ included having a well-trained multidisciplinary team to ensure high-quality investigations of safety incidents. Analysis should start with the selection of the most appropriate analytical approaches, followed by investigating the incident and development and implementation of smart recommendations that make tangible system changes. Factors related to ‘closing the loop’ included providing timely feedback to reporters and sharing results of the analysis internally with other departments as well as externally with other hospitals to facilitate learning on a wider scale.
Our results are consistent with other systematic review studies; however, we identified a gap in the research—the predominant focus is the reporting stage, leaving the subsequent stages of the learning system neglected. Vrbnjak et al35, stated that ‘a non-blaming, non-punitive and non-fearful learning culture’ is needed to encourage incident reporting. They grouped most of the system barriers into three main areas: the efficiency of the reporting system, management behaviour and staff education.35 In 2015, Health Quality Ontario identified the barriers and facilitators of PSLS, all of which are consistent with our results, including a non-accusatory environment, improving safety culture, training, enhanced transparency and effective feedback, role models (such as managers), protecting reporters, anonymous reporting, and clear operational policies. Barriers identified for other steps of PSLS have been derived from the WHO guidelines and not primary studies.36 Similar findings by other studies include a blame-free culture, clear guidelines on how and what to report, user-friendly systems, organisational support for data analysis to generate meaningful learning outcomes and multiple mechanisms to provide feedback through routes to reporters and the wider community.6 36 37
Gaps in the research
It is important to note that identified barriers to the reporting stage are also pertinent to the three themes not addressed in 19 of our included studies12–14 16 18–25 27 28 30–33 38: ‘prepare for analysis’, ‘analysis process’ and ‘follow-up’. These include a lack of time, resources and training for analysis, and a lack of direct communication between responsible departments. Under these circumstances, developing analysis teams is difficult, especially in complex organisations. Also, staff are unwilling to participate in these teams because they are afraid of losing reputation. The corresponding facilitator to these barriers is to bridge the gap in communication through holding regular meetings and structuring well representative teams with front-line engagement and top-level commitment. A newly reported barrier was related to the anonymity of the system, making it difficult to clarify incidents for which data is missing. Modifying an electronic system to not accept incomplete reports was suggested to overcome this barrier.39 It is also important to mention the problem of under-reporting and its effect on the accuracy of data processing with subsequent failure of follow-up. This can be improved through audits, use of performance scorecards and spot checks.
Participants did not reveal any barriers or facilitators under the ‘select appropriate analysis method’ subtheme. This can be attributed to being outside the scope of the included studies.
Strengths and limitations
Our study is unique as it included a variety of safety incidents including medication-related and device-related incidents. As it is more comprehensive than prior published studies, its results are more applicable to the common setting of a general hospital with a need to track all patient safety events. Our review included 22 primary studies with 781 participants, making it the largest published review on this topic, increasing the likelihood we have not omitted important published information. In addition, the participants represent different departments in hospitals, further increasing the general applicability of our findings. Furthermore, the included studies were done in geographically and economically diverse countries, representing both the developed and the developing world. We included only qualitative studies that gave more chance for participants to express their concerns about the system, which was reflected in the number of perceived system barriers and facilitators. We ensured valid results by including studies of high-quality methodology. Although 9 of the 22 studies involved relationships between the researchers and the participants with a risk of selection bias, no potential bias in their studies was reported.25
One limitation of our study related to the selection methods of the included studies. More than half of the included studies selected participants non-representative of the healthcare worker population, that is, either only doctors13 16 27 or only nurses,12 21 25 or residents. This potentially limits the generality of each study’s conclusions. However, taking the totality of findings across all studies and the consistency of the findings, we are confident our results are valid. Another limitation was an inability to perform subgroup analyses based on healthcare worker characteristics (eg, age, sex, occupation and years of experience of the participants) as studies did not consistently provide that information. Given our findings, we do not feel this limits our conclusions.
Finally, this study is based on what hospital staff perceive as factors affecting PSLS as opposed to actual quantifiable effects. This is a limitation of the existing knowledgebase that needs to be addressed in future studies.
Conclusion
Our review found that most studies on the effectiveness of PSLS relate to aspects ‘before the incident’ and the ‘immediate response’. Themes related to investigations, follow through, and ‘closing the loop’ have received less attention, and it is likely that health systems have spent less time considering them. As it is these stages that lead to improvements in safety, it is not surprising that PSLS have not achieved desired success. We recommend that researchers, safety leaders and health system policy makers focus more of their attention on these aspects of PSLS.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
All studies were granted ethical approval.
Acknowledgments
We would like to thank everyone who directly or indirectly participated in this research with special thanks to Lindsey Sikora (Health Sciences Research Librarian) for her endless support to develop the Data bases search strategy.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Corresponding author (HAM) was the guarantor responsible for the whole research at its different stages (protocol development, planning, screening of primary studies, extraction and analysis of data, writing, editing and decision of publication. AJF is the research supervisor responsible for planning, supervision and revision of the final manuscript. SM, KT and DM, they all participated in development of the protocol, revision and approval of the analysis, writing the manuscript and revision of the different edits of the manuscript. AAM and MAM they both participated in the screening of primary studies and data extraction and analysis and finally in revisions of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.