Article Text

Abstract
Background The Vancouver Island Health Authority (VIHA) implemented a standard advance care planning (ACP) document called the medical order for scope of treatment (MOST) in February 2016 to improve end of life communication and documentation. This study aims to see if the MOST implementation improves inpatient ACP documentation when compared with the ‘do not resuscitate’ (DNR) order. Improvement is measured by: (1) proportion of inpatients with documented orders for life-sustaining treatment, (2) discordance between patient’s expressed wishes and chart documentation, (3) patient satisfaction and (4) days admitted to an acute care hospital within 90 days of study inclusion.
Methods We performed a single-centre quality improvement study tracking the effects of MOST implementation. 329 consecutive patients were enrolled at a 215-bed community hospital located in Comox, British Columbia, Canada.
Results The MOST integrated well into the process of care, significantly improving ACP documentation from 33% preimplementation to 100% over 8 months of implementation. MOST completion was associated with a significant decrease in discordance between patients’ wishes and documented goals of care. Patients with a MOST were significantly older and had a higher charlson comorbidity score than those without a MOST. Despite this, there was no difference in the number of days study patients were admitted to hospital within 90 days of study inclusion.
Conclusions MOST implementation improves the frequency and quality of inpatient ACP documentation with no effect on acute care utilisation.
- advance care planning
- quality improvement
- prospective study
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Despite advances in medical care, technology-laden end-of-life (EOL) care is associated with poorer quality of life, lower patient and family satisfaction, increased family anxiety and depression and increased cost.1 2 Conflicts regarding goals of care are usually due to poor communication between healthcare providers (HCP), patients and their families, leading to unwanted treatment, family distress, clinician burnout and higher costs.1 3–7 EOL communication and documentation has been identified by patients and families as the highest priority for improving the quality of EOL care.2 8 9
Research suggests that hospital-based HCPs infrequently engage patients and families in EOL planning conversations.2 Multiple barriers to improving communication and decision-making between patients, family members and HCPs have been identified: physicians have reported inadequate patient and family understanding of the risks and benefits of therapeutic options, personal discomfort addressing EOL issues and time restrictions.3 Patients, on the other hand, have reported a lack of knowledge, confusing paperwork and a lack of clarity as to who should initiate these discussions and which HCPs are qualified to engage in these discussions.3 5
In an attempt to improve inpatient EOL care, healthcare systems have introduced various communication and documentation strategies. Advanced care planning (ACP) is a frequently used term referring to a plan you make in advance, for your care at the end of your life. In 1991, Physician Orders for Life-Sustaining Treatment was developed in Oregon and included a standard order set that allowed physicians to document the level of intervention for a given patient using a prespecified set of options.6 In 2008, a similar framework was implemented in Alberta, Canada, called the Goals of Care Designation. In 2012, the Fraser Health Region of British Columbia (BC), Canada, implemented the medical order for scope of treatment (MOST). MOST is an order set with a range of options offering more detailed guidance on desired care than the pre-existing ‘do not resuscitate’ (DNR) order. No evidence to date shows that the MOST order improves the rate or quality of documentation about scope of treatment or patient care over the DNR. In 2016, the Vancouver Island Health Authority (VIHA) (BC) adapted and planned to implement the MOST, offering a unique opportunity to prospectively study its effect on the documentation of levels of intervention in EOL care and effects on patient care.
The primary aim of this single-centre quality improvement (QI) study was to increase the proportion of inpatients with a documented order for life-sustaining treatment by 50% over 8 months by implementing the MOST order. Secondary aims were to: (1) reduce discordance between patient preferences and prescribed orders for EOL care, (2) increase patient satisfaction with care and (3) have no effect on acute care resource use.
Methods
Setting
This study is set at St Joseph’s General Hospital (SJGH), a 215-bed VIHA affiliated community hospital located in Comox, BC, Canada. The hospital’s catchment population is approximately 70 000 with a mean age of 53.9 years. Prior to MOST implementation, physicians occasionally documented orders to limit the use of cardiopulmonary resuscitation with a DNR order. The low frequency use of this order, along with the fact that it only applies to a narrow circumstance, impaired its ability to guide the use or non-use of a broader range of treatments in emergencies. In June 2016, with local administrative support, and a month of staff engagement, SJGH replaced the DNR with the VIHA MOST. MOST is a medical order placed at the front of every patient’s chart outlining their consent for the use or non-use of life sustaining treatments if they are unable to communicate their wishes. The SJGH Research Institute Institutional Review Board approved this study.
MOST intervention outline
The intervention strategy was mapped to three phases spanning from June 2015 to January 2017. In the first phase, we adapted the MOST for regional use and planned the health authority wide roll out strategy. In the second, we planned and carried out hospital implementation of the MOST. In the third, we refined study operations and data collection.
Phase 1
Adapt MOST for local context and plan regional roll out strategy (June 2015–March 2016). In the first phase, the lead author (SK) worked with the VIHA MOST steering committee to review existing goals of care order forms in use in other regions and adapt them for use within VIHA. Drawing on available literature, expert opinion and implementation experience at other sites, the VIHA steering committee optimised the MOST document as shown in figure 1 for local use. The MOST steering committee simultaneously planned a health authority wide MOST roll out strategy, including a communication plan (e-mails and presentations), the development of supporting documents and materials (lanyards, cue cards, patient information sheets) and the development of an on online education module for allied HCPs using the hospitals learning management system.
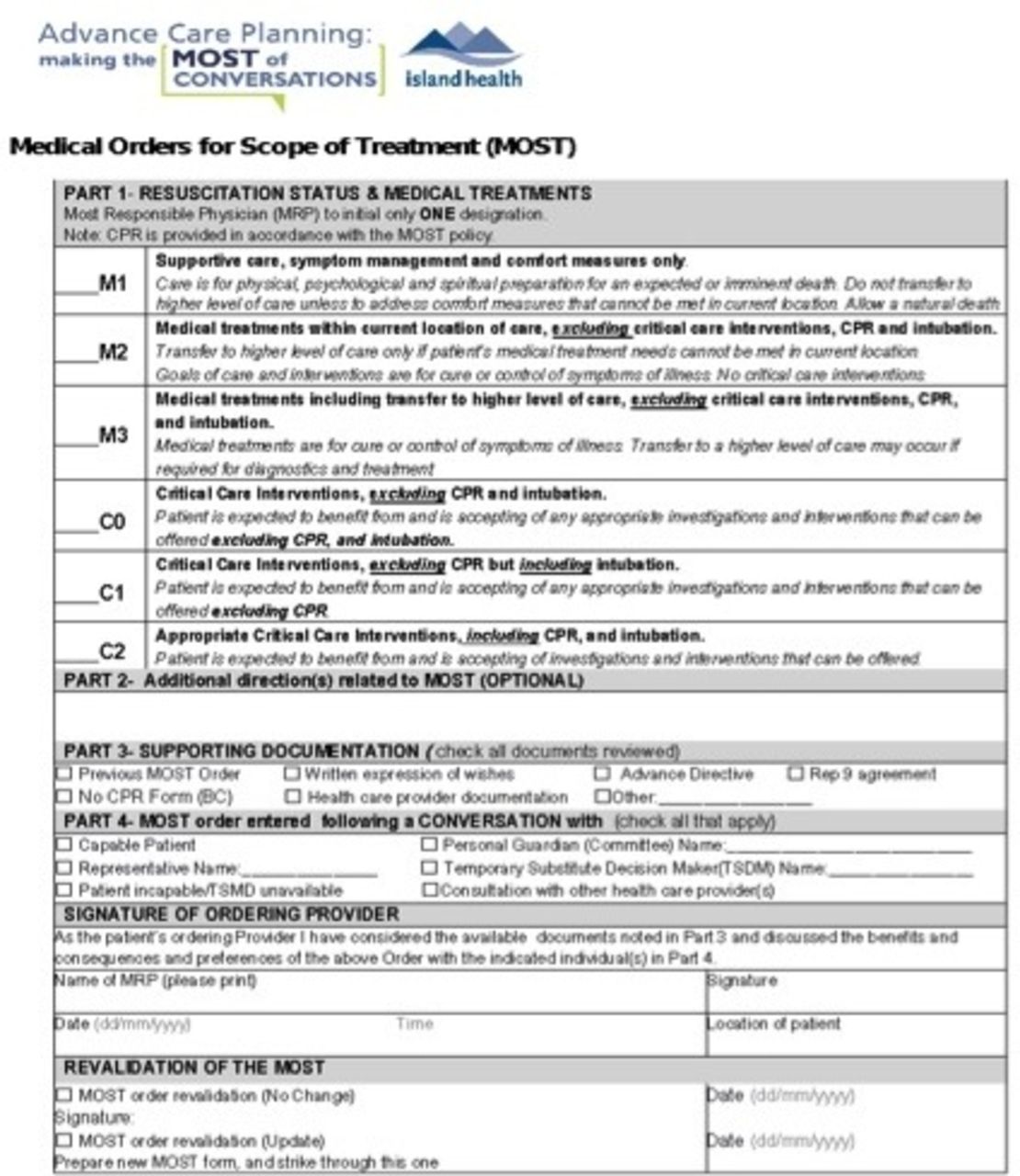
The medical order for scope of treatment (MOST) document.
Phase 2
Engage and educate hospital staff (February 2016–June 2016). Rolling out the MOST at SJGH required local hospital-based senior administrative support. To achieve this, the lead author (SK), with the support of a VIHA MOST steering committee and the health authority medical advisory council, presented the MOST and this QI project to the SJGH chief executive officer, operational and medical directors and the director of QI and patient safety. Once engaged (ie, getting buy-in), organisational implementation planning was assigned to the manager of patient flow and the clinical nurse educators. Working with the lead author (SK), the manager of patient flow and the clinical nurse educators forwarded health authority communications, arranged regular unit-based educational sessions and engaged unit managers who asked staff to complete the online education module and followed up with staff to see if they had any questions or concerns.
Simultaneously, the lead author (SK), presented the MOST to all hospital-based physician groups at their quarterly staff meetings. Provider responses were: initially, anaesthetists felt that all operative patients should be defaulted to ‘C2’ (ie, deemed that no conversation with patients was needed), but relented when considering the implications of performing interventions inconsistent with patients’ overall goals of care and the inappropriateness of resuscitation attempts for patients undergoing palliative procedures. Initially, surgeons did not feel it would be appropriate to discuss goals of care with inpatients in the absence of a long-term therapeutic relationship and suggested the patients would be better served completing the MOST order with their family doctor. The lead author explained that the surgeons were the most responsible physician intraoperatively and immediately postoperatively and that all surgical interventions should align with the patient’s goals of care and that no physician is better able to consent patients for a procedure or guide them through the management of perioperative complications than the surgeon. Finally, emphasising to specialists that they are well compensated for discussing and documenting patient goals of care reduced their resistance to engaging in such conversations.
Phase 3
Begin using MOST and refine outcomes data collection process (June 2016–January 2017). We quickly realised we could not afford to pay project technicians (PT) to collect outcome data full-time for the planned 8-month study period and therefore limited data collection to first 2 weeks of every month during the study period (doubling the length of time we could collect data). This allowed us to estimate monthly compliance over the planned 8-month period. Early in the study, we discovered that we were missing predischarge data for many patients recruited into the study. We identified that this was because of a hospital push to discharge patients before 09:00, which did not leave PTs with enough time to identify patients who were being discharged and approach them before leaving. We overcame this barrier by having PTs attend multidisciplinary discharge rounds, identify patients likely to be discharged the day before and approach them first thing in the morning on the day of discharge. This greatly decreased the number of patients who were discharged without being approached by the PT. We are anticipating the need to make additional modifications to address inadequate response or plateaus in MOST uptake; however, our data showed a continuous increase in documented orders throughout the study period.
Patients
During the first 2 weeks of every month during the study period (1 May 2016–31 January 2017), we approached consecutive patients admitted to hospital. This study included all competent adult (age 18 years or older) patients admitted to the intensive care unit, telemetry, medical or surgical wards. Patients were excluded if they did not consent to inclusion in the study, were being isolated for a communicable disease or were expected to die or be discharged within 48 hours. Patients were only approached on their first study admission and excluded from re-recruitment on subsequent hospital visits. A visual outline of our recruitment, inclusion and exclusion process is outlined in figure 2.
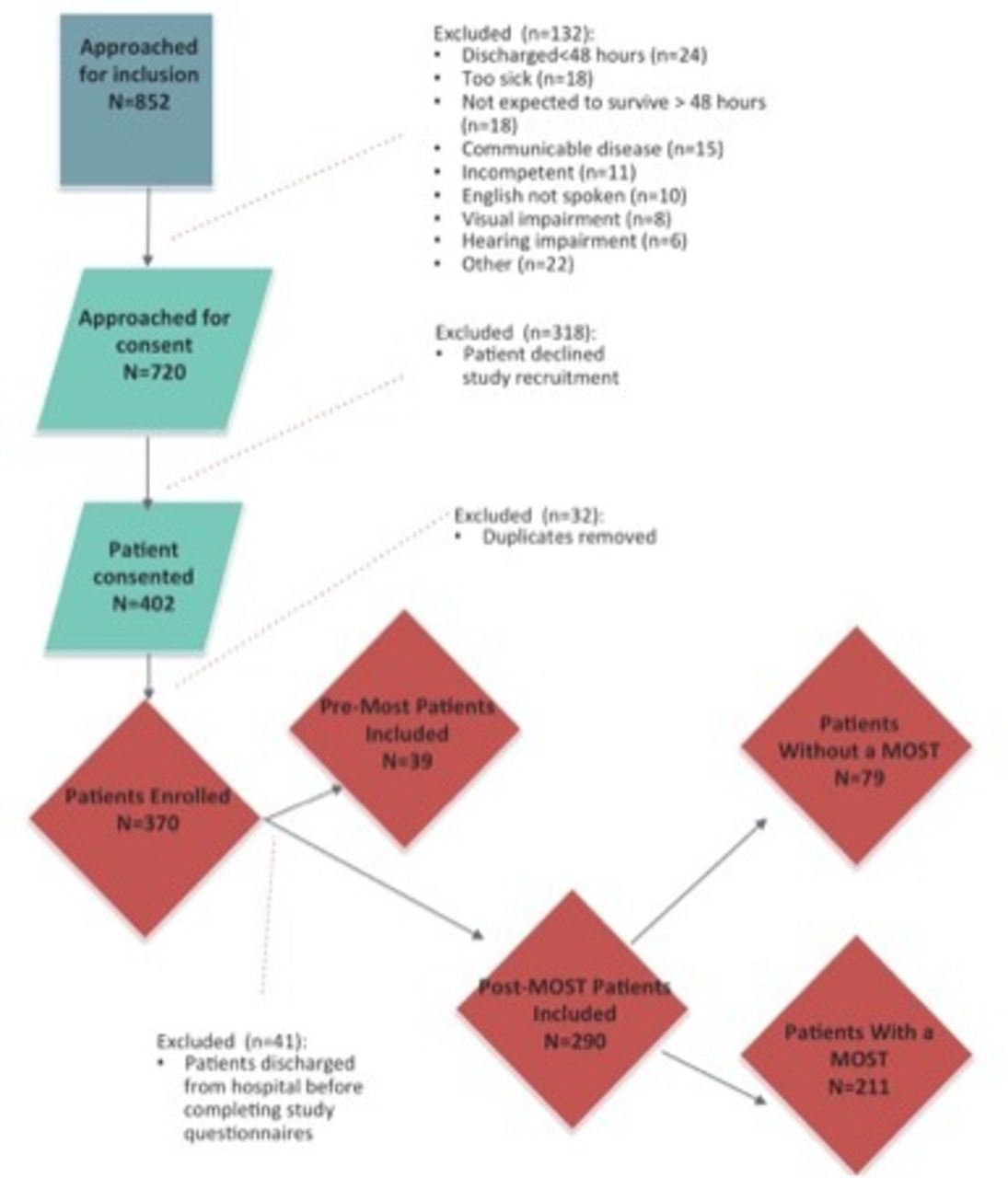
Study flow of participants.
Study design
We recorded pre-MOST implementation data in May 2016 and MOST implementation data from June 2016 to January 2017. Throughout the study, PTs approached potential study patients within 24 hours of hospitalisation for inclusion into the study. MOST order concepts were not explained to patients beyond those needed for consent. Once informed consent was obtained, patients were entered into a confidential, study-specific electronic database. On the day of discharge, a project technician interviewed study patients using a standard data collection package, including CANHELP Lite, and a patient completed MOST. Total completion time was approximately 15 min. Following the interview, each patient’s chart was reviewed by a project technician and/or the project manager to extract key demographics and the documented orders for life-sustaining treatment. Three months post-discharge, we used the VIHA electronic medical record to determine each patient’s total number of days admitted to a VIHA acute care facility.
The study minimised patient exposure to non-organisational MOST and ACP (EOL care) interventions by limiting initial project technician contact with patients to a standard consent document only. Study-related questionnaires were only presented to participants on the day of discharge, when exposure to these concepts could no longer affect patient’s knowledge or chart documentation.
Outcome measures
This study’s primary outcome was the proportion of inpatients with documented orders for life-sustaining treatment, measured at each patient’s first hospitalisation during the study period. Before MOST implementation at SJGH, some patients had a DNR order on the chart which, despite its limitations, was considered adequate documentation. A few patients had specific instructions such as ‘Would accept BiPAP but not intubation’ written as a medical order or in the progress notes, which was also deemed adequate. Once we implemented the MOST, in accordance with VIHA policy, only patients who had a completed MOST on their chart were determined to have adequate documented orders for life-sustaining treatment. Secondary outcome measures were: (1) discordance between patient preferences and prescribed orders for life-sustaining treatments, measured as the number of MOST categories between a patient-completed and chart-documented MOST. As the MOST order has six escalating levels of care, discordance can range from 0 (if the patient chose the same category as was documented on the chart) to 5 (if the patient wishes and chart documentation were opposite) (eg, ‘C2’ vs ‘M0’, see figure 1). Patients with no documented ‘code status’ were classified as ‘full code’ (MOST C2), in accordance with current practice standards.10–13 (2) Patient-reported satisfaction with care, measured using the CANHELP Lite, a 21-item satisfaction questionnaire validated for use with patients who have advanced, life-limiting illnesses.14 Scores on CANHELP Lite range from 1 to 5 points. (3) Acute care utilisation, defined as the total number of hospital days from the time of consent to 90 days after recruitment, extracted from the VIHA electronic medical record.
Data and statistical analysis
Baseline characteristics are summarised with mean (SD), count (%) or median (quartile 1 (Q1), quartile 2 (Q2),) as appropriate. Primary and secondary outcomes are summarised using run charts that display monthly mean values between May 2016 and January 2017, comparing participants who received the MOST intervention with those who did not. We made two comparions. First, we compared the pre-MOST and MOST implementation groups. For the latter, we included patients with and without a MOST, to evaluate MOST uptake over time. Second, after MOST implementation, we compared patients with and without a MOST to observe the effect of MOST implementation on patient outcomes. Cohort data was compared using t-tests when continuous data were normally distributed, the Mann-Whitney U test for skewed continuous data and χ2 tests for categorical data . In order to explore the effects of baseline covariates on the outcomes, we built generalised linear mixed regression models for each outcome adjusting for age (years), gender (male and female), Charlson Comorbidity Index (CCI) (1–10), study period (pre-MOST vs MOST implementation) and for MOST implementation period patients, whether a MOST was recorded. ORs, 95% CIs and p values are calculated. The level of significance was set at α=0.05.
Results
Participants
The patient recruitment process is outlined in figure 2. A total of 852 patients were considered for inclusion in the study. One hundred thirty-two patients were excluded by PTs using prespecified criteria and 318 patients declined involvement, most commonly due to a lack of interest. Another 32 patients were excluded because they had already been recruited into the study on a previous admission. This yields a recruitment rate of 54% (370 enrolled/688 eligible patient approached for consent). Our final sample included 39 patients pre-MOST implementation and 290 MOST implementation patients (79 patients with no MOST and 211 patients who had a MOST documented), for a total of 329. The demographic and clinical characteristics of study patients are listed in table 1. The mean (SD) age of our sample was 72.7 (12.9); 53.5% were female. Across groups, there were statistically significant differences in the distribution of age, CCI, admitting diagnosis and unit. Of note, MOST implementation patients without a documented MOST were on average: younger, had a lower CCI and were more likely to have been admitted via the surgical unit.
Patient characteristics
Primary outcome
Documented orders for life-sustaining treatment
Overall, MOST implementation was associated with a 41% increase in the documented orders for life-sustaining treatment (before implementation 33.3% (N=39), during implementation 74.5% (N=290); p<0.01) (table 2). Further, figure 3 shows how the percentage of patients with documented orders for life-sustaining treatment increased to 100% over 8 months of implementing the MOST, averaging an 8% increase per month. Among the 13 preimplementation patients with clear documentation, levels of care included ‘full code’ in 39% (n=5 patients), DNR in 31% (n=4 patients) and ‘other’ status (designating medical/supportive care) in 31% (n=4 patients).
Summary of study outcomes before and during MOST implementation periods

Per cent of patients with documented orders for life-sustaining treatment.
Secondary outcomes
Discordance
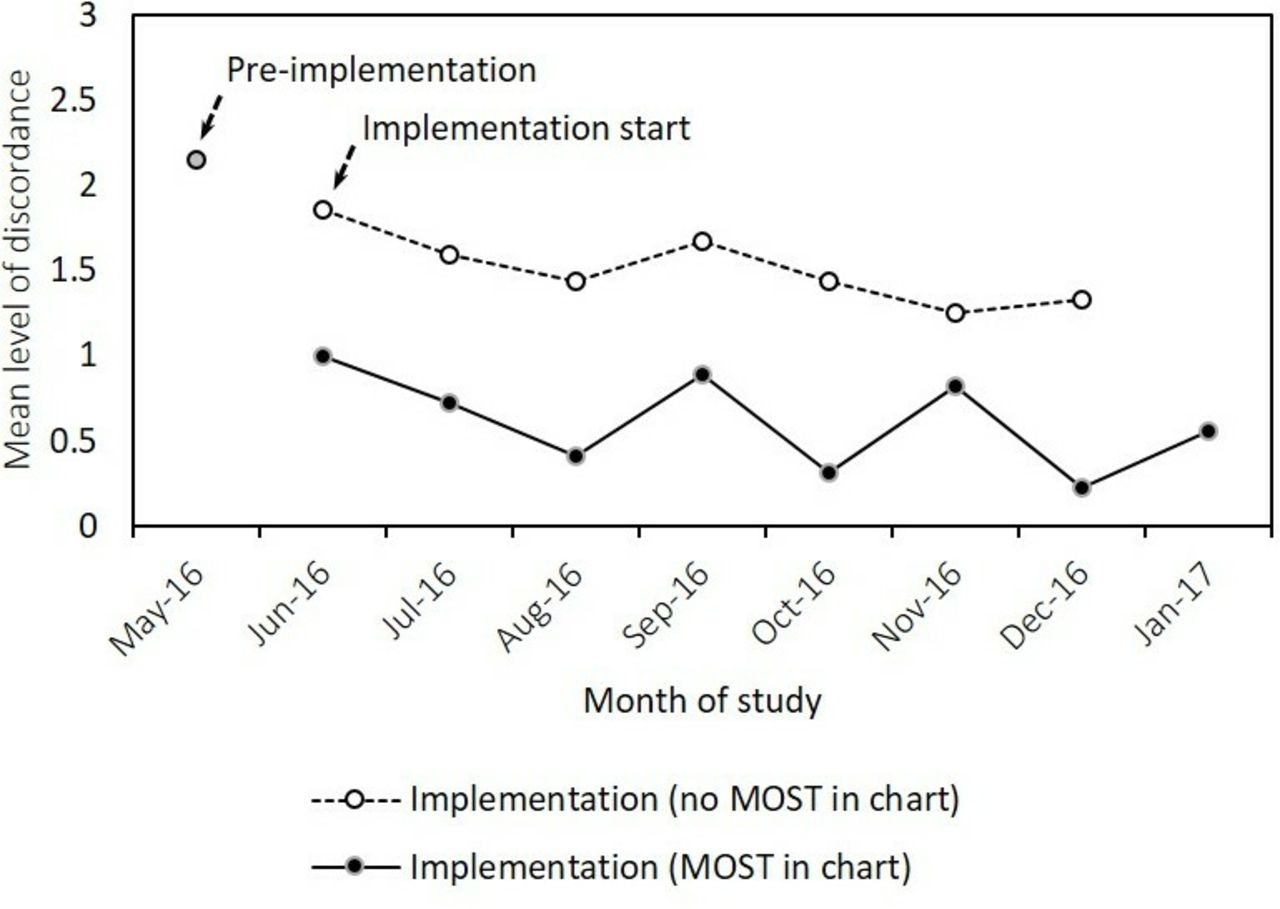
MOST implementation was associated with a significant decrease in the mean level of discordance. Preimplementation mean discordance was 2.2 (1.6); implementatation mean discordance was 0.85 (1.5), p<0.01 (table 2). A run chart showing mean discordance over time is shown in figure 4. In the MOST implementation phase, patients with a MOST had lower mean discordance than those without a MOST (1.6 (1.7) vs 0.5 (1.2), respectively; p<0.01) (table 3). Those patients with a chart documented MOST were fourfold less likely to experience any level of discordance in expressed preferences for care (level ‘0’ compared with levels ‘1–5’; OR 4.1, 95% CI 2.3 to 7.1, p<0.0001). We observed that 25% of patient with a chart-documented MOST still had some degree of discordance with their expressed wishes (online supplementary table 1). Of these, 40% has one degree of discordance, 24% had two degrees and 36% had ≥3 degrees of discordance.
Supplemental material
Summary of study outcomes during the implementation period, comparing patients with and without a chart-documented MOST

Mean level of discordance between patient expressed preferences for care and those documented in the patient chart (or in the absence of documentation, implied by hospital policy). MOST, medical order scope of treatment.
Patient-reported satisfaction with care
Based on mean CanHelp Lite scores, MOST implementation was not associated with a significant difference in ‘general’ satisfaction with care (table 2). Mean satisfaction with ‘decision-making’, however, improved from 3.9 (0.7) before implementation to 4.2 (0.4) during implementation, p=0.0002 (table 2). During the intervention period, mean general satisfaction with care was paradoxically higher in patients without a documented MOST (4.4 (0.59) vs 4.2 (0.60); p=0.01), but mean satisfaction with decision-making was not significantly different (table 3). This could be because patients without a MOST were on average younger, had a lower CCI and were more likely to have been admitted via the surgical unit (table 1). Trends over time in general satisfaction and satisfaction with decision-making are illustrated in figures 5 and 6. The before and during implementation patient cohorts also differed significantly for the CanHelp Lite dimension ‘satisfaction’ (p=0.0001), ‘illness management’ (p=0.0022), ‘communication’ (p=0.0001) and ‘feeling at peace’ (p=0.0009) (online supplementary table 2). In postintervention comparisons of patients with and without a MOST, only the CanHelp Lite dimension ‘general’ satisfaction with care was significantly different.
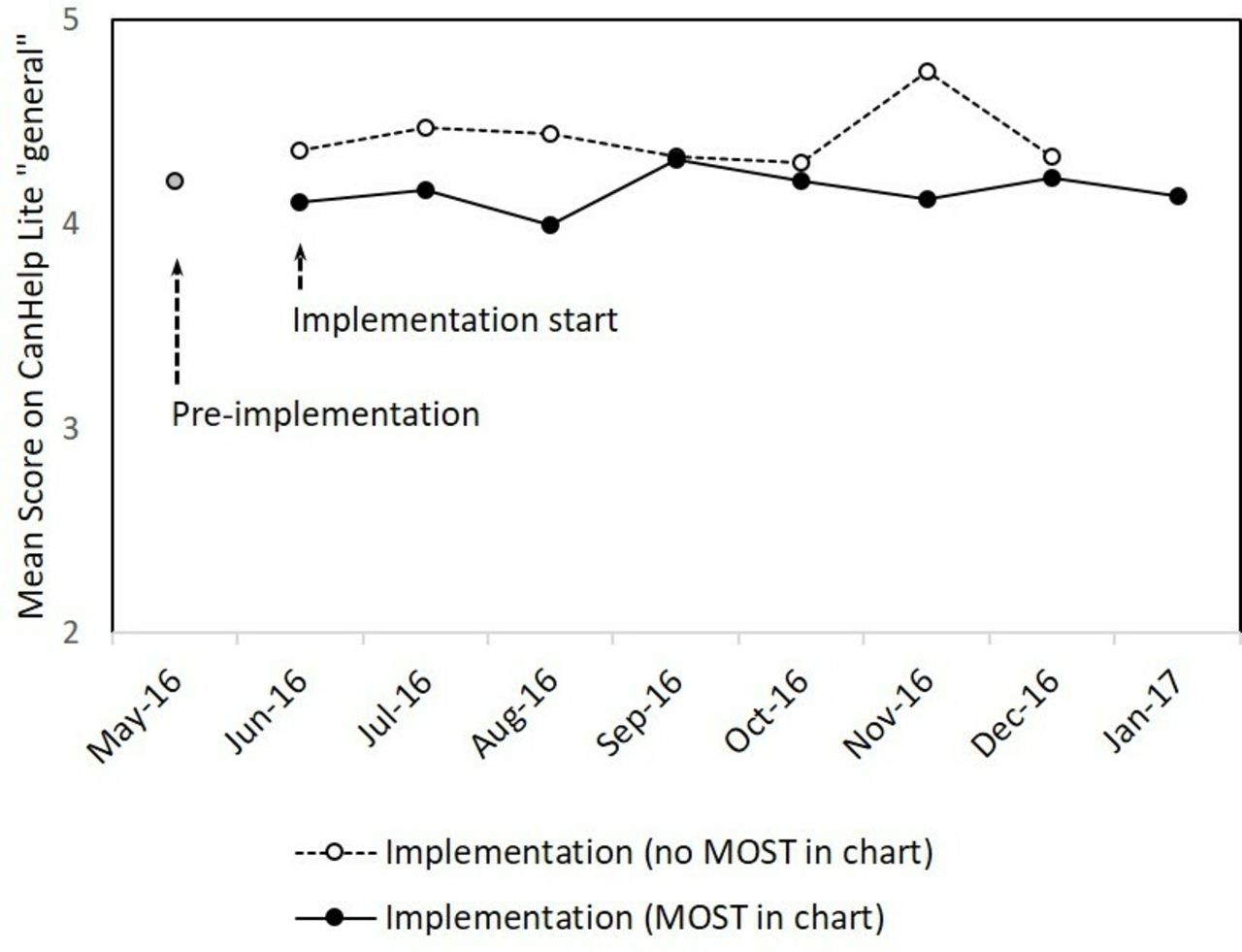
Mean score of ‘general satisfaction with care’ (CanHelp Lite). MOST, medical order scope of treatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean score of ‘satisfaction with decision-making’ (CanHelp Lite). MOST, medical order scope of treatment.
Acute care resource use, as measured by hospital length of stay
Patients median length of stay was 3 and 4 days, before and after implementation of MOST, respectively (p=0.29) (table 2). For the during implementation period, median length of stay was not different between patients with and without a MOST (table 3).
Exploratory analyses: baseline covariates, study outcomes
To control for potential confounding due to differences in patients baseline characteristics, we adjusted for age, gender and CCI, in separate generalised linear models for each of the primary and secondary outcomes. For the primary outcome, documented orders for life-sustaining treatment, patients in the implementation cohort were more likely to have documentation than the patients in the preimplementation cohort (OR 5.08, 95% CI 2.31 to 11.19; p<0.01). In this model, a higher CCI was also associated with documentation rates (OR 1.96, 95% CI 1.5 to 2.5; p<0.01). For the secondary outcome discordance, during implementation, participants with a charted MOST had a smaller mean discordance interval (OR 0.3, 95% CI 0.2 to 0.5; p<0.01). Additionally, in this model, increased age was associated with higher discordance (OR 1.02, 95% CI 1.01 to 1.03; p=0.01). For the secondary outcome general satisfaction with care, no difference between groups was observed (OR 1.02, 95% CI 0.82 to 1.26; p=0.85), and none of the covariates were significant predictor in the model. For satisfication with decision-making, patients in the implementation group were more likely to be satisfied with decision-making (OR 1.41, 95% CI 1.13 to 1.75; p<0.01). Further, a higher CCI was associated with less satisfaction with decision-making (OR 0.94, 95% CI 0.89 to 0.99; p=0.03). Finally, length of hospital stay did not differ between before and during implementation, despite including patients baseline covariates (p=0.23). No covariates were significant predictors of length of stay in this model.
Discussion
Our hospital-wide implementation of the MOST order significantly improved both the frequency and quality of documentation of orders for the use or non-use of life-sustaining treatments.
The rate of hospital-based documentation of decisions about life-sustaining treatment is highly variable and the quality frequently poor15 16 leading to unwanted treatment, family distress, clinician burnout and higher costs.1 3–7 For example, Fraser Health Region, one of BC’s most populous health authorities reports MOST completion ranging from 29% to 75% depending on the site.17 Similarly, Alberta Health Services, reports Goals of Care Directive completion ranging from 45% to 89%.18 While it is impossible to compare study data to audit data directly, the degree of improvement we observed in documented orders for life-sustaining treatment (from 33% to 100% over 8 months) shows that the MOST order can be quickly and effectively implemented in the clinical setting. Further, an audit of months 3–6 after the project concluded (as part of a planned follow-up study) showed that improvements in this primary outcome had been sustained with a rate of 92% being observed (average of month 3–6).
We also observed an improvement in the quality of documentation in terms of reducing discordance. Standardising documentation with the MOST is associated with a substantial decrease in discordance between patient’s preferences for life-sustaining treatment and prescribed orders. Though measured differently, previously published multicentre studies of seriously ill hospitalised patients report high levels of discordance.19–22 To our knowledge, this QI study is the first to observe that a standard documentation tool is associated with a reduction in discordance between patients’ preferences and their prescribed orders, suggesting that a standard order set (MOST) is better than usual care.
The dramatic improvement in the rate and quality of EOL care documentation observed with MOST implementation is associated with a small, statistically significant improvement in satisfaction with decision-making, previously identified by Heyland et al as the highest priority for improvement of end-of-life care.8 9 True informed consent, however, requires a reasonable understanding of the risks and benefits of available healthcare options, thus, highlighting an important remaining target to improve EOL communication.
This study did not observe any difference in the use of acute care resources between patients with or without a MOST, as defined by the number of days patients are admitted to an acute care facility within 90 days of study inclusion. There is no standard way to measure acute care utilisation, limiting comparisons between studies. Available studies, however, show an inconsistent effect of ACP on acute care utilisation. For example, the SUPPORT trial23 found that facilitated discussion had no effect on reducing length of hospital stay, while Zheng and Edes reported decreased length of stay with professionally facilitated discussions about future medical care.5 24
Implementation lessons
This project encountered a number of barriers that are frequently experienced in QI studies, such as competing organisational priorities, change fatigue, clinical and administrative resistance and financial limitations. With an upcoming hospital transition, hospital administration and staff were already experiencing change fatigue. It was therefore not surprising that SJGH administration was hesitant to take on another large-scale clinical change. While the timing of our MOST implementation was suboptimal, it was mandated by VIHA and already being rolled out throughout the health authority. Failure to implement the MOST locally would have led to conflicting goals of care documentation between co-dependent hospitals, clinical uncertainty and potentially conflict. With health authority wide administrative support and local appreciation of the resulting clinical risk, SJGH agreed to implement the MOST locally. Ideally, we would not recommend implementing multiple significant changes at the same time. It was important that allied HCP resistance was managed by local clinical nurse educators, while physician concerns were addressed by the lead author (SK), who was locally considered to have clinical expertise. The financial administration of this project took significant resources and would not have been possible without external funding and continuous study optimisation.
Limitations
There are several limitations to this study. First, allocation to the MOST intervention was not randomised, making it more difficult to make inferences about causation. A single-centre randomised controlled trial, however, would be almost impossible to execute because contamination would be unavoidable, and a cluster randomised controlled trial was not feasible with available resources. Nevertheless, the significant improvement in ACP documentation is most likely due to MOST implementation, as opposed to other contemporaneous factors. Second, due to timeline and resource limitations, we were only able to collect baseline data for 1 month, limiting reliability of preintervention data. Third, to evaluate the impact of our intervention, we only included patients who consented to data collection. As half the eligible patients we approached did not consent to participate in our study, there is a possibility of a selection bias, limiting the generalisability of our findings to centres using administrative data. Fourth, because the MOST form and education strategy were simutaneously implemented, this study cannot differentiate each component’s contribution to the observed improvement. Fifth, discordance was measured by comparing a self-reported MOST category with chart documentation. We assumed that competent patients would be able to understand the simplified MOST form. This study’s strengths, however, include its tangible clinical results, use of validated tools and rigorous data collection processes.
Conclusion
To our knowledge, this QI study is the first to support the hypothesis that multidisciplinary implementation of a standardised order set can improve both the frequency and quality of inpatient documentation of medical orders for life-sustaining treatments when compared with usual care. Further, this study outlines a simple implementation strategy that other hospitals can adapt and apply to their processes of care to see similar improvements.
Acknowledgments
The authors would like to thank the project technicians who delivered the MOST intervention at SJGH (M Hathway, B McDowell, M Heymann, K Collins and E Williams), the MOST implementation advisory committee including J You and I Benbasat, and the operational support of J Murphy and P McDonald. Thanks to M Earp for providing manuscript editorial support.
References
Footnotes
Contributors RN and SK lead the study. SK acquired funding, designed the study and aided in implementation. RN assisted in study design, oversaw implementation and managed the projects daily operations. RN and SK wrote and revised the manuscript.
Funding This study was funded by the Comox Valley Auxillary Society, Division of Family Practice, and Healthcare Foundation, and the Doctors of BC.
Competing interests None declared.
Ethics approval St. Joseph's General Hospital Ethics Committee AND The Vancouver Island Health Authority Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information