Article Text

Abstract
Smoking tobacco is a major public health issue and a significant cause of increased mortality. People with a first episode of psychosis are more likely to smoke and the subgroup that goes on to have schizophrenia will have a significantly reduced life expectancy to the general population. The City & Hackney Early and Quick Intervention in Psychosis Team is a community mental health team at East London NHS Foundation Trust, providing outpatient care for adults presenting with first episode psychosis. This project aimed to increase the number of smoking cessation referrals from EQUIP to national smoking cessation services to 15% of the total team caseload over 6 months initially. A secondary measure was to complete an assessment of the smoking status for 90% of the caseload at all times. Change ideas were tested using plan-do-study-act cycles. A smoking cessation referral pathway was created and disseminated to the outpatient and inpatient services. The project was discussed at least monthly at the clinical team meeting. An education and skills building session was organised and took place at the team away day and an education drop-in session for patients was organised. The project was slow to take-off and patient participation was essential in driving progress. The aim was achieved at 23 months. A collateral benefit indicated that 25.7% of the total number of smokers had been recorded as having stopped smoking during the course of this project. This project demonstrates the effectiveness of quality improvement methodology facilitated by efficient leadership, collaborative teamwork, patient participation and persistence to address a complex problem that has significant consequences to patient health.
- quality improvement
- attitude of health personnel
- community mental health services
- coronary disease
- health promotion
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- quality improvement
- attitude of health personnel
- community mental health services
- coronary disease
- health promotion
Problem
Smoking disproportionately affects people suffering with mental illnesses with rates being 3–4 times higher for those with schizophrenia or bipolar disorder.1 First episode psychosis is associated with decreased life expectancy2 due to cardiovascular risk factors and for the schizophrenia subgroup there is an increased morbidity and mortality.3 Alongside the illness, treatment with antipsychotics and other psychotropic medication can lead to metabolic syndrome which increases the risk.
The first episode of psychosis is typically preceded by subtle signs and prodromal symptoms. Early assessment and treatment are critical to maximise longer-term outcomes for the mental health and physical health of these patients. Early and Quick Intervention in Psychosis (EQUIP) is a community mental health team in City and Hackney; the latter is one of the most deprived boroughs of England until 2015.4 It provides care for adults (18–65 years old) in the first 3 years of illness.
There is a significant focus on improving quality of physical healthcare in order to bridge the gap between physical and mental health services and it is a strategic priority for East London NHS Foundation Trust (ELFT). Smoking cessation is associated with significant positive outcomes for both mental health and physical health5 6 in the longer term. Smoke-free policies have been implemented across services in the National Health Service (NHS), including mental health settings7 despite difficulties in implementation.8 9 The ELFT Smokefree Vision strategy is in line with recommendations from the National Institute for Health and Care Excellence (NICE), Public Health England and the Department of Health.
Background
The incidence of smoking is higher in groups of people with serious mental illness (SMI).10 Tobacco is a leading cause of death and a key modifiable factor for several physical health morbidities. Vulnerable groups such as people with low socioeconomic background, co-morbid alcohol and substance misuse, homeless and minority populations are over-represented among those with SMI. Given the overwhelming benefits of smoking cessation for physical11 and mental health12 this is a major potential area for intervention and improvement.
Historically patients with SMI engage poorly with smoking cessation services. Pragmatic approaches are required to address this13 and teams are faced with multiple barriers along the way.14 Patients report smoking to gain autonomy, relieve boredom, manage stress, gain pleasure and enjoyment, to develop social relations and as a form of social pastime, as a form of self-medicating, to manage or counteract the unwanted effects of some antipsychotic medications. Nicotine and co-morbid cannabis addiction, lack of motivation, stress, peer pressure and the severity of mental health symptoms are perceived barriers to cessation despite the patients’ concerns about the adverse physical health effects, the peer pressures to quit, the concerns about the economic cost. Nicotine replacement therapy, smoking cessation, pharmacological interventions, behavioural interventions, smoking cessation advisors and monetary incentives may be effective interventions.15
Members of staff hold mixed perceptions about smoking. Some consider it a patient right and hold misconceptions about patient inability to quit or even actively discourage patients from quitting.9 16 Staff may also feel that smoking is an important issue, ascribing variable urgency to this matter with other health complaints taking precedence.
The smoking status of staff is a known barrier to smoking cessation especially in inpatient settings.17 Other barriers include lack of formal training in offering smoking cessation and motivational interviewing, increased workload and other competing treatment priorities and lack of set targets for offering support and treatment.18 Given the complexity of systemic factors, barriers and facilitators relating to smoking and smoking cessation, the task of promoting smoking cessation is complex. A pragmatic approach is required when implementing strategies of change on a local level.
All EQUIP staff undertake level 1 smoking cessation training.19 Two members have completed level 2 smoking cessation training and are leads for the in-house smoking cessation programme. They provide concurrent supportive interventions for four patients at any time. Patients seeking smoking cessation are also referred to national smoking cessation (NSC) services including the Hackney Stop Smoking Service, Stop Smoking London, Stop Smoking clinics and pharmacies in the borough.
Baseline measurement
Baseline data in April 2017 indicated that out of 89 smokers on a caseload of 240 patients, only one had a smoking cessation assessment completed. The low completion rate was suggestive of a need to promote awareness of smoking cessation to staff and we used the percentage of completed smoking status assessments as a process measure.
We set the overall aim of the project at increasing the number of smoking cessation referrals through the national pathway, as recorded in the Trust’s patient electronic records (RIO), to a total of 15% of the number of smokers in the team caseload in 6 months. The target was decided as a ‘realistic’ but ambitious goal compared with the Clinical Commissioning Group’s expectation for 7% reduction in the number of smokers. Accounting for the insufficient baseline data, we safeguarded against the risk of an overinflated cumulative result: those who relapsed into smoking after successful cessation or transitioned from the service were removed from the outcome numbers.
All patients on the caseload were required to have a smoking assessment as part of the Trust’s physical health-related Commissioning for Quality and Innovation (CQUIN) target: lifestyle assessment. This assessment classifies patients as current smokers, ex-smokers and non-smokers and if in the former category eligibility for interventions and consent for referral to NSC services is recorded. Staff ought to undertake a paper, email or over the phone referral for any interested patients. An automatic electronic national referral option was introduced in electronic records in September 2018, however, full functionality was established in another couple of months.
For measurement, smoking cessation referrals were counted by feedback through various sources: Trust’s performance data, confirmation from smoking cessation providers of referrals received and immediate feedback from the care coordinators.
Design
We formed a local quality improvement (QI) team including doctors, care-coordinators and frontline staff. ELFT is partnered with the Institute for Healthcare Improvement (IHI), the project design followed the IHI model, and all project leads had received prior QI training.20 Service user involvement was sought and achieved from August 2018 onwards. Links with the inpatient service were created by the shared appointment of the senior trainee psychiatrist across inpatient and outpatient pathways. The initial step included the creation of a driver diagram (figure 1) with obstacles and facilitators to change, hypothesising a major role for staff attitudes and education. Consistently with this hypothesis, we set our project measures aimed at staff performance: our target was to increase smoking cessation referrals to 15% out of the total number of smokers and we aimed to achieve this in 6 months. Smoking status assessments, another performance indicator, were used as a process measure.
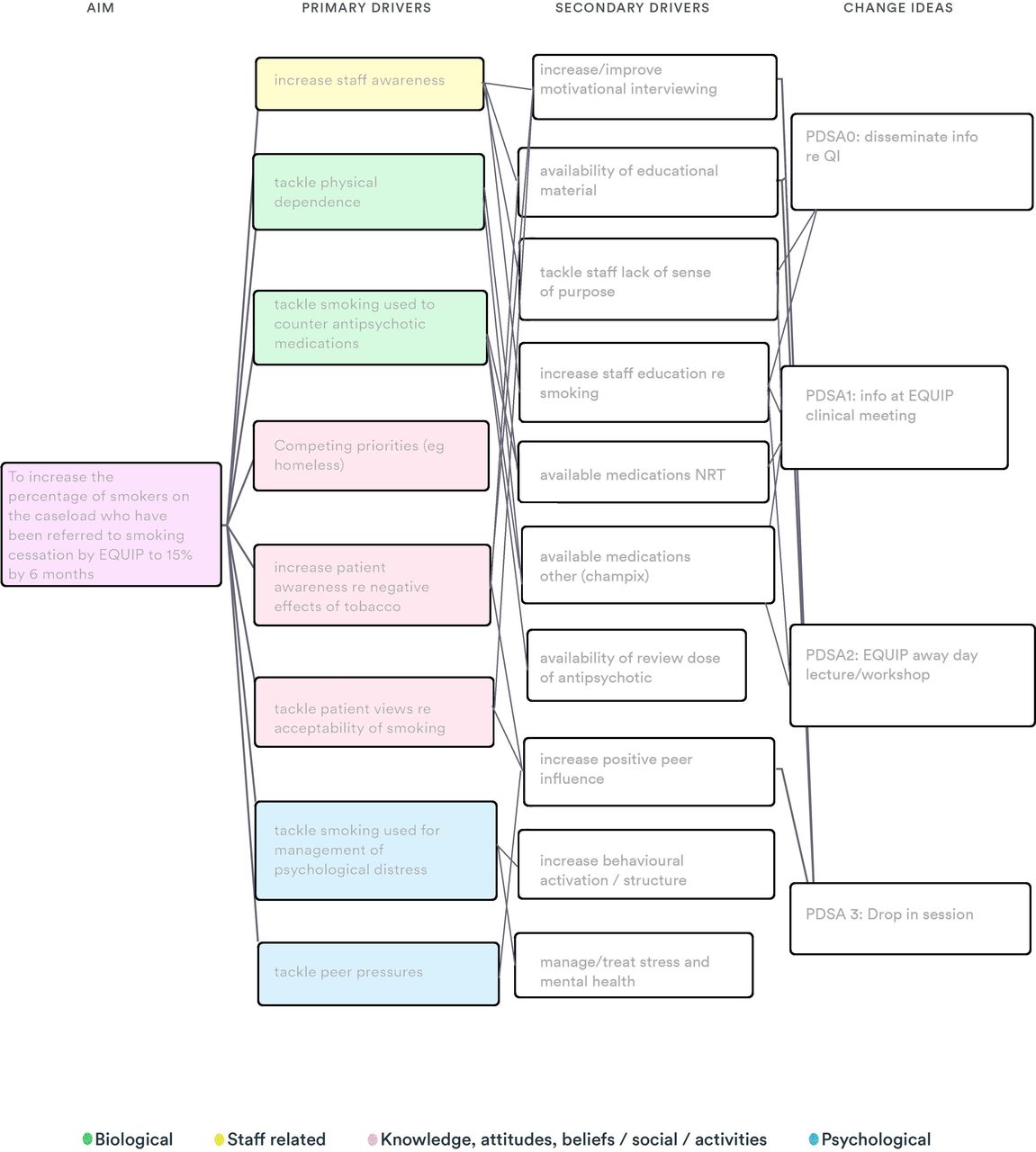
Driver diagram. EQUIP, Early and Quick Intervention in Psychosis; PDSA, plan-do-study-act; QI, quality improvement.
Strategy: plan-do-study-act (PDSA) cycles
Devising a smoking cessation referral pathway
This change idea included the creation of a structured smoking referral pathway. This was communicated to all team members in the outpatient and inpatient services. It was also exhibited for reference in EQUIP offices. Smoking cessation information leaflets for patients and motivational interviewing tools were collated and regularly updated to form a smoking cessation package. This cycle was completed at baseline and adjusted to a smaller clinical meeting update that formed the second PDSA. The visual representation of the referral pathway and information dissemination proved to be successful as evidenced by shifts to both the process and outcome measures.
Regular updates in clinical meetings
This update consisted of a reminder of basic principles and standards as set in the first PDSA cycle during the weekly EQUIP team meeting. Discussion took between 5 and 10 min and included an update on available data, obstacles and facilitators to change, and collection of feedback and recommendations from EQUIP staff. In addition, the QI team provided a monthly email update of compliance and performance records serving as a prompt for the members of staff tasked with completing smoking status assessments and smoking cessation referrals. Multiple trials of this PDSA cycle took place as it was considered a primary driver and allowed visual representation of progress.
Training sessions in the team away days and the team’s Continuous Professional Development sessions
Training sessions for smoking cessation were designed and delivered across two away-day team meetings. The educational sessions focused on learning about smoking and mental health. They included workshops to practice practical skills on motivational interviewing (role play, scenarios) and the ethical implications of smoking cessation in mental health were discussed. These were co-produced with an expert by experience patient and their personal story was used to support the team’s learning.
A medical update on access to in-house prescribing of varenicline was completed. Staff gave overwhelmingly positive feedback about this intervention and the impact was evidenced by a further improvement in the performance data following implementation during the first away day in September 2018.
A second trial of this cycle was implemented in June 2019 and sessions are planned to continue after completion of the project with a view to sustaining change over time.
In-house drop in sessions
A week of regular drop-in sessions for patients under EQUIP and Heads UP (early detection service) considering smoking cessation was trialled in January 2019. This cycle was not repeated due to low attendance rates.
Results
The project was characterised by a slow take-off period characteristic of the complexity of the problem, the challenges of designing the project and bringing together different members of a working group.
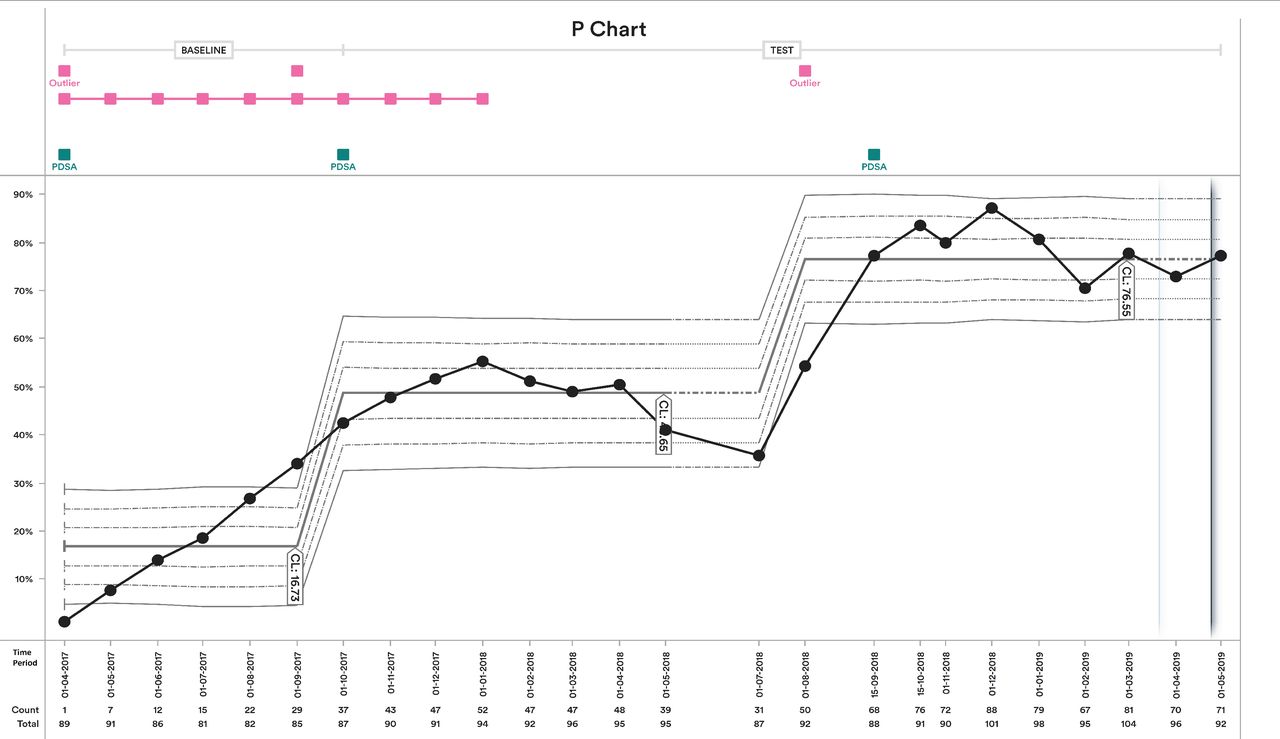
As a result the aim was not met at the initial timeframe of 6 months. However, given the progress, the project was continued and evidence of a clear shift in both the process measure (figure 2) and outcome measure (figure 3) is evidenced in the first year.
Process measure—caseload percentage of completed smoking status assessments.

{kind=link}
{kind=link}
{kind=link}
Outcome measure—caseload percentage of completed smoking cessation referrals.
This was followed by a plateau and a period of stagnation in the following months also evidenced in the gaps in data collection. This may be due to reshaping of the team with change-over of senior trainee psychiatrists in August 2018.
The project influenced a parallel change that was not planned, by which patients seeking smoking cessation could be directly referred to NSC services via the RIO lifestyle form, rather than through phone calls or sign-posting.
In August 2018, patient participation was enrolled and a third PDSA was trialled which renewed the team’s commitment to achieving the project goal. We recruited an expert by experience service user who had successfully quit smoking. They attended regular meetings, co-produced interventions and PDSAs and provided motivational speeches to the team. They also led the in-house smoking cessation drop-in sessions.
The outcome measure p-chart evidences the completion of the set target by March 2019 and this was sustained in the following month. The process measure indicated high levels of completed smoking cessation assessments, averaging at more than 70% but falling short of the set target of 90%.
A plan for embedding the procedures of PDSA cycle 2 into the team’s practice based on the learning achieved through cycle 1 and periodic reinforcement of achieved practice through educational sessions and workshops was made. Encouraging preliminary data indicate that referrals by EQUIP lead to a positive outcome (9 out of 11 referrals between 1 January 2019 and 11 March 2020 led to successful intervention) and that this compares favourably to other ELFT services.
Lessons and limitations
This project aimed to address a significant population health problem at a local team level in the challenging area of mental health. We used a rigorous QI PDSA methodology, in one site, with sequential staggered introduction of interventions some of which run concurrently. We adopted a pragmatic approach and chose outcome measures aiming primarily at staff attitudes, as directed by our driver diagram. Slow initial progress is indicative of the complexity of the issue and a long latency period for the first two PDSAs. Effective leadership and collaborative team work, persistence in the data collection despite shortcomings and commitment in the face of difficulty in progression was vital for the project’s progress.
Patient participation was particularly important and the third and fourth PDSAs were co-produced. The service user was an expert by experience, knowledgeable in the smoking cessation interventions and with a gift of passion and commitment to smoking cessation that was inspiring. This created a stimulating dialogue with QI members who had personal experience of smoking cessation.
The project team were able to manage with the impact of staff change-over although this affected data collection in June and September 2018. It can be hypothesised that such a change may have otherwise led to an early closure of the incomplete project. Effective leadership and patient participation was essential in regaining momentum.
The drop-in session change idea proved unsuccessful compared with the implementation of staff education measures. This indicated that the major driver in change is the day-to-day relationship between front-line staff and their patients, consistently with our primary hypothesis. We also neglected to collect measurable feedback on the perceived quality of the educational intervention (third PDSA) which makes the evaluation vulnerable to bias.
The Trust had established QI processes and methodologies in place and technical support from the QI team was invaluable. An improvement in the electronic lifestyle assessment form and referral pathway, leading to transition from manual and paper referral methods to e-referral processes was important but may also be a confounding factor.
Positive reinforcement of progress was given to staff on a regular basis by the project lead in the form of the QI project update email and healthy mutual support between staff to improve practice developed over time.
The cost effectiveness of this project was not studied. It is likely that this was a low cost intervention that made good use of already existing processes. However, the longer time required for implementation of change may be a limitation to future replication.
The target for 90% completion rate for smoking status assessments at all times was not achieved. This relates to (1) a lag between new referrals and first assessment completion and (2) expiring 6 monthly assessments that were not renewed in a timely manner. Challenges in this area were not overcome with the PDSAs used, and are suggestive of limitations related to time-commitments and suboptimal attitudinal change through interventions used (eg, in the inpatient site and primary source of many new referrals).
A hypothesis of the project that was not articulated from the outset was that access to smoking cessation pathways may lead to a reduction in the number of smokers. The initial design of the project did not aim to evaluate the true effectiveness of the interventions offered, by measuring dynamic variations in smoking rates. We consider this a limitation. However, we retrospectively identified that 25.7% of the total number of smokers had been recorded as having stopped smoking during the course of this project, which is important in the context of the complexity of the task.21 Sustainability of outcomes was studied in the short team and there is a possibility that results may diminish with time. We aim to repeat measurements after 6 months from the completion and closure of the project to revisit the sustainability of positive outcomes. The aim is also to extend this project by measuring actual changes in smoking status rather than completed referrals.
The findings of this project were developed into an intervention package and this was disseminated to other teams within the Trust wishing to carry out smoking cessation work. There are some limitations to the generalisability of interventions from results in one site, as EQUIP have specific structures and processes that differ from other community mental health teams (eg, a reduced caseload, quick access to psychology). Contextual factors that may facilitate replicability are the patient participation and the focus on staff education and performance. Gaps in data collection may be addressed in future trials by anticipating staff changeover and absences.
It is possible that change took place in ways that were not readily observable or measured, which is an identified risk for the pragmatic QI approach we chose.22 In keeping with the nature of the methodology, causality was not established, but an effective approach was developed and embedded to the team’s practice.
The collateral benefit of an increased number of smokers who did actually quit smoking is encouraging. Increasing awareness of research evidence on smoking and SMI, developing a wide range of interventions and developing a culture to challenge misconceptions about the intractable nature of smoking patterns in the mental health population contributed to change that may have been indirectly associated with the implemented change ideas.
Conclusion
Tobacco dependence and smoking is a known problem among people with SMI, including those with first episode psychosis. Smoking cessation can lead to significant benefits to the physical health of this population through dramatic reductions in morbidity and mortality.
This project met its aim of increasing the rate of referral of smokers within EQUIP. Although the aim was not met within the initial period of 6 months, the project was extended due to evidence of progress, the complexity of the problem and the significance of the project’s aim to improve patient health. Stagnation was overcome through effective leadership, patient participation and persistence.
This project provides an example for the effectiveness of QI in managing a notoriously complex problem and may serve as a starting ground for expansion of such initiatives to other mental health teams and NHS services.
Acknowledgments
We would like to thank the staff at EQUIP and the QI team, Sam Evans and Megan Pugh, in-house smoking cessation leads and QI members, the General Adult Mental Health Care Directorate ELFT for their contribution to this work, Francisco Frasquilho (ELFT senior QI advisor), Miranda Eeles (Smokefree Hackney) and the Smoking Cessation Service Team at Whittington Health NHS Trust, and the librarians at Homerton Newcomb Library and Basildon Healthcare Library for their help with access to the literature.
Footnotes
Contributors SG conceived and sponsored the project. NH initially formularised and led the project with help from QI members. OKB took over as the lead and prepared the initial draft for the paper. TS coached the QI team and MJ with DP participated as members. OKB, NH, MJ, DP, TS and SG jointly reviewed the initial draft, worked on revisions and corrections and agreed the final manuscript contributing equally to this process.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement One service user was involved as a full member of the QI project team and independent expert by experience advisor. Her insights drawn from her lived experience and successful smoking cessation were essential in giving this project its final form. Her personal details have been withheld for confidentiality.
Patient consent for publication Not required.
Ethics approval This work was considered exempt from ethical approval as it was deemed an improvement study and not a study on human subjects.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement East London NHS Foundation Trust is the owner of the data relevant to this study, which are available upon reasonable request.