Article Text

Abstract
Background Acute kidney injury (AKI) is a common postoperative complication which increases morbidity and mortality. This quality improvement project aimed to implement measures targeting known risk factors to decrease the incidence of postoperative AKI in trauma and orthopaedics (T&O) patients.
Methods Data were collected across three six-month to 7-month cycles between 2017 and 2020, analysing all elective and emergency T&O operated patients within a single NHS Trust (n=714, 1008 and 928, respectively). Patients who developed a postoperative AKI were identified using biochemical criteria and data were collected on known AKI risk factors, including use of nephrotoxic medications, and patient outcomes. In the final cycle, the same variables were collected for patients without AKI. Between cycles, measures implemented included: preoperative and postoperative medication reconciliation aiming to stop nephrotoxic medications, orthogeriatrician review of high-risk patients and junior doctor teaching on fluid therapy. Statistical analysis was undertaken to determine the incidence of postoperative AKI across cycles, prevalence of risk factors and impact on length of hospital stay and postoperative mortality.
Results There was a statistically significant decrease in postoperative AKI incidence from 4.27% (43 of 1008 patients) in cycle 2 to 2.05% (19 of 928) in cycle 3 (p=0.006), with a notable decrease in use of nephrotoxic medications. Significant predictors for the development of postoperative AKI included use of diuretics and receiving multiple nephrotoxic drug classes. Development of postoperative AKI significantly increased length of hospital stay by 7.11 days on average (95% CI: 4.84 to 9.38 days, p<0.001) and risk of 1-year postoperative mortality (OR 3.22, 95% CI: 1.03 to 10.55, p=0.046).
Conclusion This project demonstrates that a multifaceted approach targeting modifiable risk factors can reduce incidence of postoperative AKI in T&O patients, which may lead to reduced length of hospital stay and postoperative mortality.
- acute kidney injury
- quality improvement
- postoperative care
Data availability statement
Data are available on reasonable request. Anonymised data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Postoperative acute kidney injury (AKI) is an increasingly common complication in trauma and orthopaedics (T&O) patients, which has been shown to worsen patient outcomes and increase hospital and staff burden.
We sought to reduce the incidence of postoperative AKI in our department through targeting known risk factors, which has not previously been done in both emergency and elective T&O patients.
WHAT THIS STUDY ADDS
Implementing targeted perioperative interventions, such as withholding nephrotoxic medications, can significantly reduce incidence of postoperative AKI in T&O patients.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Simple, relatively cost-free, interventions such as medication reviews and focused junior doctor teaching can reduce the incidence of postoperative AKI across T&O departments, which may lead to improved patient outcomes.
Problem
Acute kidney injury (AKI) is a common postoperative complication in trauma and orthopaedic (T&O) patients, which leads to increased length of hospital stay, risk of other postoperative complications, morbidity and mortality.1–5 A large-scale cohort study estimated the incidence of AKI for postoperative T&O patients at 10.8%.6 Studies focusing on AKI following elective procedures found rates of 6.8%5 and 8.2%1 compared with 17% of patients following emergency surgery.3 7 Importantly, while undergoing an operation is in itself a risk factor for developing an AKI, emergency T&O patients in particular are often at greater risk, given their frailty and comorbidities.3
We conducted a quality improvement project (QIP) due to concerns regarding high rates of postoperative AKI within our department, and the impact of this on patient outcomes. This project was conducted within a single NHS Trust which performs over 2000 T&O operations a year, including day case, elective and emergency procedures, and has a dedicated orthogeriatrics service to assist with inpatient management. Postoperatively, patients are managed by junior doctors (often at foundation year 1 or 2 level) with senior support. These junior doctors are responsible for fluid prescribing and work alongside ward pharmacists in medicine reconciliation and review of nephrotoxic medications.
Postoperative AKI is a potentially preventable complication; the mainstay of preventative measures involve addressing modifiable risk factors including avoidance of nephrotoxic medications and appropriate fluid management.8
Our QIP therefore aimed to achieve the following:
To determine the incidence of postoperative AKI within our T&O department.
To ascertain the prevalence of known modifiable AKI risk factors for patients developing a postoperative AKI.
Through targeting of these identified risk factors, to reduce the incidence of postoperative AKI across both emergency and elective procedures by at least 1% over the planned 2-year study period.
To determine the impact of postoperative AKI on length of hospital stay and 1-year postoperative mortality.
Background
AKI is a significant problem within the National Health Service (NHS) across all specialties with a standardised prevalence of 14.7% and an associated mortality of 28.1%.9 This in turn translates to costs of over £1 billion per year for the NHS.9 The National Institute for Health and Care Excellence guideline on AKI highlights key risk factors in surgical patients, namely: age, comorbidities including heart and kidney disease, emergency surgery and the use of nephrotoxic medications. With regard to prevention, they recommend routinely assessing the risk of AKI preoperatively based on the above factors, discussing these risks with the patient and formulating a clinical management plan based on this, presumably through optimisation of modifiable risk factors.10
There is a notable body of literature investigating risk factors for the development of AKI, specifically in postoperative orthopaedic patients. A meta-analysis and cohort study found that male gender, age, American Society of Anaesthesiologists (ASA) grade of 3 or more and use of ACE inhibitors (ACEi) were significantly associated with postoperative AKI.6 11 The latter study also suggested that the number of prescribed medications was an independent risk factor.6 Furthermore, use of angiotensin receptor blockers (ARBs) increased the risk of postoperative AKI following colorectal surgery.12 A large-scale cohort study conducted in non-orthopaedic patients found a significant association between the use of diuretics and the development of AKI following major surgery.13 In addition, the impact of perioperative non-steroidal anti-inflammatory drug (NSAID) use on the development of postoperative AKI remains under question with unequivocal findings from a recent systematic review.14 Hypotension, both intraoperatively and postoperatively, has been shown to increase risk of postoperative AKI.8
The potential impact of gentamicin, a known nephrotoxic and commonly used surgical antibiotic prophylaxis, on development of postoperative AKI has also been considered. Three studies investigating postoperative AKI rates following a change in antibiotic prophylaxis for primary arthroplasty from gentamicin and flucloxacillin to either co-amoxiclav or cefuroxime found increased rates of AKI in those receiving gentamicin. Notably, there was no significant change in rates of Clostridium difficile or surgical site infections.15–17 Our Trust guidelines throughout our study period recommended the use of single-dose 160 mg intravenous gentamicin with weight-based teicoplanin and antibiotic-loaded cement (where applicable) for all T&O procedures with the exception of open fracture surgery and emergency surgery not including hip fractures.
In summary, the key modifiable risk factors for postoperative AKI development include hypotension and use of nephrotoxic medications including: ACEi/ARB, diuretics, gentamicin and possible NSAIDs.
There is now evidence that targeting the aforementioned risk factors may act as a means of AKI prevention. A recent study by Malinge et al has demonstrated a decreased incidence of postoperative AKI in elective T&O patients following the introduction of targeted peri-operative interventions. These measures included optimisation of fluid status and withholding nephrotoxic medications such as ACEi/ARB and NSAIDs prior to and following their operation.18 This peri-operative protocol involved intensive measures including outpatient nephrology review for high-risk patients or those with chronic kidney disease stage 3b or higher. A further QIP demonstrated that suspending nephrotoxic medications, optimal peri-operative fluid management and educational measures reduced incidence of postoperative AKI in elective patients, although this was not statistically significant.19 However, these studies do not include emergency T&O patients who are inherently at higher risk of AKI and pose a greater challenge in prevention, due to the unplanned nature of admission.
Measurement
We conducted a single-centre QIP with three Plan-Do-Study-Act (PDSA) cycles aiming to reduce incidence of postoperative AKI across both elective and emergency T&O operations. Our study population included all T&O admissions to our Trust who underwent an operation across the three cycles of data collection. Our first data collection period took place between 1 December 2017 and 31 May 2018, with the second taking place across the same 6-month period the following year. The final period was delayed and extended to 7 months between 1 June 2020 and 31 December 2020 due to the impact of the COVID-19 pandemic, and to allow for a more comparable number of operations between cycles. Patients who underwent a day case procedure were excluded as most would not have a postoperative assessment of renal function. Those with pre-existing AKI at the time of their operation were also excluded.
Patients developing an AKI following their operation and during the same admission were identified automatically on our online pathology results system using the Acute Kidney Injury Network (AKIN) criteria, based on a rise in serum creatinine of >26.4 µmol/L over 48 hours or a rise >1.5 times the baseline serum creatinine.20 Urine output was not used as this information was not readily available and there were concerns over accuracy of documentation.
For patients identified as developing a postoperative AKI, data were collected on known AKI risk factors. Patients’ sex, age on admission, whether the operation was elective or emergency, the ASA grade of patients, length of hospital stay and 1-year postoperative mortality is routinely coded and was provided to us by the Trust Informatics team. From patient observation charts, we recorded whether patients had an episode of hypotension (defined as systolic blood pressure <90 mm Hg) during their admission as a proxy marker of hypovolaemia. From computerised patient drug charts, it was recorded whether they were prescribed different nephrotoxic drug classes prior to the development of AKI including NSAIDs, ACEi or ARB, gentamicin or diuretics. The full list of medications included in these categories can be found in online supplemental appendix 1. A composite variable of the number of risk factor drug classes prescribed was calculated. The stage of AKI (as per the AKIN criteria) and the number of days postoperatively the AKI developed were calculated.
Supplemental material
For the final period of data collection, the same relevant variables were collected for patients who underwent an elective or emergency T&O operation and did not develop an AKI to control for potential confounders. This was done by the Trust Informatics team using clinical coding from electronic patient notes. This was not feasible for our first PDSA cycles as the Trust switched to computer-based documentation mid-way through the second period of data collection.
Statistical analysis was conducted using R (V.3.6.3) and p values of <0.05 were considered statistically significant. Descriptive statistics of the demographic characteristics and prevalence of AKI risk factors across the three cycles and between patients with AKI and patients without AKI in the final cycle were reported. Visual inspection of histograms and the Shapiro-Wilk test were used to determine whether data were normally distributed. The Kruskal-Wallis test, χ2 test and Fisher’s exact test were conducted as appropriate to determine significant differences between the groups with regard to demographic characteristics and AKI risk factors.
To control for confounders and using all eligible patients from the final cycle of data collection, additional binary logistic regression models were constructed with development of postoperative AKI as the outcome and demographic variables, potential risk factors and use of multiple risk factor drug classes as covariates. Further multiple linear regression and binary logistic regression models were constructed for the outcomes of length of stay and 1-year postoperative mortality, respectively, using demographic variables and occurrence of postoperative AKI as covariates.
Design
Our QIP team consisted of T&O junior doctors, medical students, T&O consultants and colleagues of the orthogeriatrics team. We arranged team meetings following each data collection cycle to discuss the results and potential interventions we could implement. Additional key groups involved in the project included the Trust Informatics and Clinical Effectiveness teams. There was no patient or public involvement at any stage in the project.
Based on previous literature, we sought to implement simple, relatively cost-free interventions with the aim of reducing the prevalence of known AKI risk factors within our study population. Our assumption was that by targeting modifiable risk factors we can minimise the risk of postoperative AKI, thereby driving down incidence within the department.
We adopted a multifaceted approach to AKI prevention through education, review of guidelines and medication reviews. These interventions involved key stakeholders including junior doctors, anaesthetic, orthogeriatric and T&O consultants.
Our initial measures implemented following the first cycle included a review of our Enhanced Recovery After Surgery (ERAS) protocol. A teaching session for junior doctors on fluid management and optimising fluid status in the peri-operative period was conducted and further developed over the PDSA cycles.
More intensive interventions were implemented following the second cycle, targeting different aspects of the peri-operative period. First, we recommended a preoperative medication review to be undertaken by the anaesthetics team and T&O junior doctors for elective patients, and the clerking junior doctor for emergency admissions, with a focus on stopping known nephrotoxic medications. All high-risk patients such as those undergoing hip or knee arthroplasty, elderly patients and those undergoing emergency large-joint surgery are reviewed by a junior doctor 2−3 hours postoperatively. We recommended undertaking a medications re-review at this stage to ensure nephrotoxic medications were withheld. We further ensured that very high-risk patients such as those who are clinically frail or suffered a fractured neck of femur, had a day 1 postoperative review by an orthogeriatrician. Given concerns over risk of secondary joint infections and to remain in line with national guidance, gentamicin continued to be recommended for surgical prophylaxis. However, we sought to increase awareness of its nephrotoxicity within the department and for operating teams to consider alternatives in high-risk patients.
Strategy
Following data collection and analysis of our first PDSA cycle, the results and recommendations were presented at the T&O Quality Improvement Day which was attended by departmental leads, T&O consultants, the orthogeriatrics team, junior doctors, nursing staff and other allied healthcare professionals within the department. The initial interventions implemented included a change to our ERAS protocol so NSAIDs were no longer routinely prescribed for postoperative analgesia for patients aged over 65 years. Further to this, a teaching session for current and new T&O junior doctors on fluid management was conducted.
However, given the rising postoperative AKI rates and NSAID use following the second PDSA cycle, it was apparent that these initial measures had not been successful. It is likely that a simple change in guideline and one-off education session had not led to a meaningful change in practice and therefore outcomes. Consequently, we implemented more intensive measures and again presented our findings and proposed changes at the T&O Quality Improvement Day. We further developed the education aspect for junior doctors by delivering a 4-month course on postoperative complications, including prevention of AKI, which was repeated for each rotation of newly starting doctors from August 2019. This included a session on peri-operative fluid management led by a consultant anaesthetist, a session on AKI prevention led by a consultant orthogeriatrician and further bedside teaching. A short course booklet was provided to all current and new T&O junior doctors with a printout and posters placed in the doctors’ office on the ward. To evaluate the effectiveness of the educational programme, pre-programme and post-programme surveys, using Likert scales from 1 (not at all confident) to 5 (extremely confident), were administered to identify any changes in junior doctors’ confidence in managing peri-operative complications. Combining data from the three rotations in 2019/20, junior doctor confidence in the prevention and management of AKI increased significantly from before to after the teaching programme (median confidence rating before=3.5 (n=34), median confidence rating after=4 (n=21), p=0.023). Although not a direct marker of knowledge, improvements in confidence likely relate to better understanding of AKI prevention, coupled with practical experience.
To facilitate medication reviews, we wrote and disseminated proformas within our electronic documentation system for both emergency admission clerking and postoperative reviews, which included a reminder to withhold nephrotoxic medications where appropriate. These proformas were well received and are now widely used by junior doctors (online supplemental appendix 2). We continued to liaise with the orthogeriatrics team and reiterated the nephrotoxic risks of gentamicin.
To ensure the sustainability of our interventions, we will continue to deliver the postoperative complications teaching programme and encourage use of our proformas for new starting junior doctors. Further to this, we aim to engage other members of the healthcare team including the ward nursing staff and pharmacists, who rotate around wards less frequently than junior doctors and can play an important role through monitoring of fluid balance and medication reviews.
Results
The demographic characteristics, incidence of postoperative AKI and prevalence of AKI risk factors in each of the PDSA cycles are outlined in table 1. There were no significant differences in sex, age or ASA grade between cycles, although there was a significantly greater proportion of emergency operations in the final cycle, as was expected given the ongoing COVID-19 pandemic. Despite an initial increase between cycles 1 and 2, there was a statistically significant decrease in postoperative AKI incidence from 4.27% (43 from 1008 patients) in cycle 2 to 2.05% (19 from 928 patients) in cycle 3 (p=0.006). A significantly reduced proportion of patients with AKI received gentamicin in cycle 3 compared with the first two cycles. However, a significantly greater proportion of patients with AKI received diuretics prior to development of AKI in cycle 3 as compared with cycle 2, reasons for which are unclear. Furthermore, there was no improvement in the proportion of patients with AKI who were hypovolaemic during admission. It should be noted that there was a reduction in the proportion of patients with AKI receiving ACEi/ARB, NSAIDs and multiple risk factor drug classes prior to AKI onset between cycles 2 and 3, although this did not reach statistical significance. The majority of postoperative AKI was mild (stage 1) and occurred in the first 2 days postoperatively.
Demographic characteristics of the study population and prevalence of AKI risk factors in patients with postoperative AKI, stratified by PDSA cycles 1, 2 and 3
Our key finding from cycle 1 was the high proportion of patients with postoperative AKI receiving nephrotoxic medications; notably, all received at least one class of nephrotoxic. In cycle 2 as compared with cycle 1, there was an increase in the number of patients with postoperative AKI who were hypotensive and received NSAIDs or gentamicin, although we cannot conclude whether this explains the rise in postoperative AKI incidence between the first cycles.
Table 2 outlines the demographic characteristics and prevalence of AKI risk factors in all eligible T&O patients in the final cycle of data collection, stratified by whether or not they developed an AKI (n=928). Our univariate analysis shows that patients with AKI were significantly more likely to be older, female, ASA grade 3 or 4, received gentamicin, an ACEi/ARB or a diuretic. While a significantly greater proportion of patients receiving multiple risk factor drugs developed an AKI, there was notably no significant difference in proportions of patients with AKI and patients without AKI who received NSAIDs or were hypotensive during admission. Patients with postoperative AKI had a significantly greater length of stay and 1-year postoperative mortality. However, our multivariate analysis, when adjusting for demographic characteristics, found that only age and diuretic use (adjusted OR 3.31, 95% CI: 1.10 to 10.22, p=0.003) were significant predictors for the development of AKI. This multivariate analysis can be found in online supplemental appendix 3. A further binary logistic regression model was constructed with postoperative AKI as the outcome and receiving multiple risk factor drugs classes as a covariate, adjusted for age, sex, type of operation and ASA grade and can be found in online supplemental appendix 4. It shows that receiving more than one nephrotoxic drug class is a significant predictor for the development of AKI (OR 5.00, 95% CI: 1.87 to 13.95, p=0.001).
Demographic characteristics and AKI risk factors of the all T&O patients undergoing an elective or emergency operation between 1 June 2020 and 31 December 2020 (inclusive) in terms of those who had a postoperative AKI and those who did not
The results of the multivariate analysis of the effect of postoperative AKI on patient outcomes is shown in table 3. Adjusted for age, sex, type of operation and ASA grade, development of postoperative AKI significantly increases length of hospital stay by 7.11 days on average (95% CI: 4.84 to 9.38 days, p<0.001) and risk of 1-year postoperative mortality (OR 3.22, 95% CI: 1.03 to 10.55, p=0.046).
Multiple linear regression model (second column) with length of stay (days) as the outcome and demographic variables and occurrence of postoperative AKI as covariates using data from all T&O admissions between 1 June 2020 and 31 December 2020
Lessons and limitations
Our results demonstrate a significant reduction in postoperative AKI incidence following the introduction of our more intensive interventions. We have shown that patients with AKI were significantly more likely to have received ACEi/ARB and gentamicin, and that use of multiple risk factor drug classes is a significant, independent predictor of postoperative AKI development. Further to this, we have demonstrated a notable reduction in the proportion of patients with AKI who received these medications (and multiple risk factor drug classes) between the final two cycles, suggesting a degree of success in our interventions. Despite this, there was minimal change across the three cycles in the proportion of patients with AKI who were hypovolaemic or received diuretics indicating there remains room for improvement in future cycles. Finally, we have demonstrated that postoperative AKI significantly prolongs length of hospital stay and increases risk of 1-year postoperative mortality.
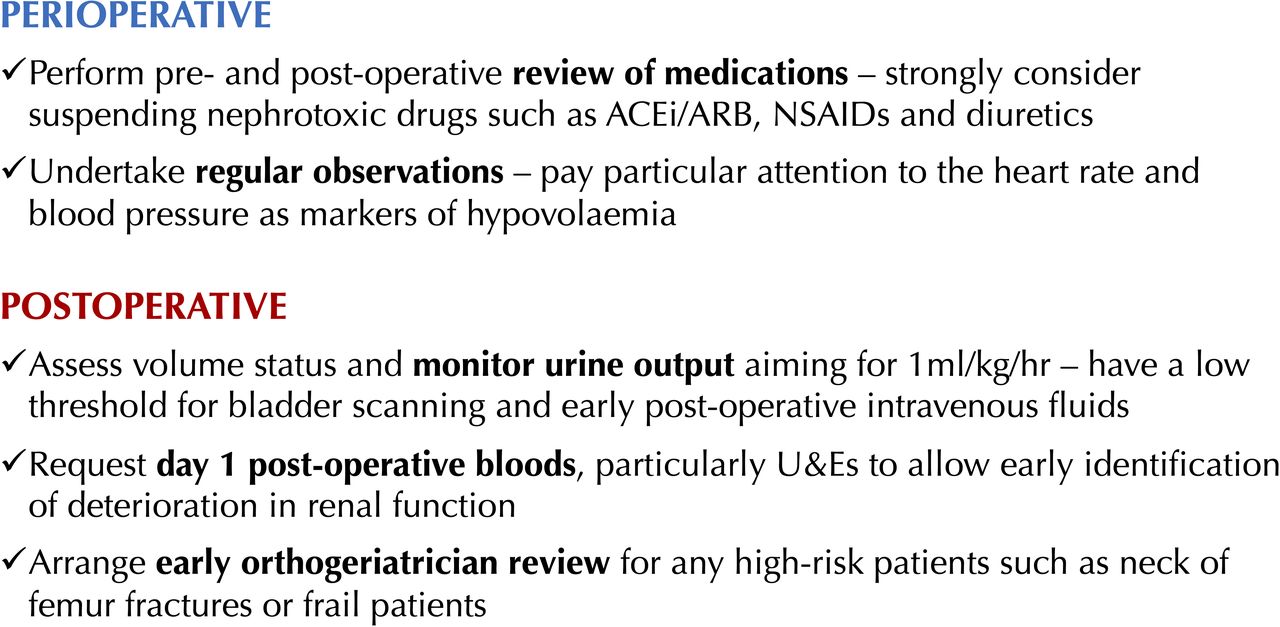
We therefore suggest the following recommendations of perioperative measures for AKI prevention which are outlined in figure 1.
{kind=link}
Recommendations of perioperative measures for AKI prevention. ACEi, ACE inhibitor; ARB, angiotensin receptor blocker; NSAID, non-steroidal anti-inflammatory drug; U&Es, urea and electrolytes.
It should be noted that while the individual drug classes may not have been independent risk factors in our multivariate analysis, patients receiving multiple nephrotoxic drug classes were at significantly greater risk. This may suggest that these medications act synergistically as nephrotoxins, in keeping with their known effects on renal blood flow, thereby producing additive effects and resulting in AKI.
This QIP is one of the first to demonstrate a ‘real-world’ decrease in postoperative AKI in both emergency and elective T&O patients through simple interventions targeting modifiable risk factors. We have constructed a robust and relatively complete dataset given the data were collected across both paper and electronic notes. Considering that we have used an undifferentiated study population with minimal exclusion criteria and have used relatively reproducible interventions, we hope this will improve the generalisability of the findings should others wish to implement them in different departments or even specialties.
However, this project is not without its limitations. First, we were not feasibly able to collect data for patients without AKI in the first two cycles and as such we cannot truly determine whether the prevalence of AKI risk factors reduced across the whole cohort, rather than just within the small proportion of AKI cases. In addition, we did not directly record compliance with interventions, for instance, whether medication reviews were conducted or whether high-risk patients received an orthogeriatrics review, and instead used nephrotoxic drug administration as a proxy outcome measure. However, it should be noted that use of emergency clerking and postoperative proformas and orthogeriatric reviews of high-risk patients has largely been established as standard practice within the department. We appreciate that patient comorbidity is a potential confounder for which we did not collect data, largely due to challenges with clinical coding and our focus on targeting modifiable risk factors. It is plausible, for example, that chronic kidney disease and heart failure are themselves risk factors rather than the ACEi/ARB, which are commonly used in their treatment. We used hypotension as a proxy marker of hypovolaemia; however, literature suggests this may be a late marker of hypovolaemia and hence renal underperfusion.21 While urine output may be a more accurate measure, it is typically poorly documented or not routinely measured. The majority of our analysis focused on the cohort within the final PDSA cycle which took place during the COVID-19 pandemic and therefore contained a disproportionate number of emergency operations. This may have affected our results and thereby the external validity of the findings. Finally, this was an underpowered project to detect statistically significant risk factors and reductions in postoperative AKI incidence; however, as a QIP our primary aim was in affecting a ‘real-world’ reduction within our own department.
Conclusions
Our results show a notably lower incidence of postoperative AKI in comparison to the previous cohort study using both elective and emergency patients.6 One suggested reason for this may be in the differing patient populations; our study population was younger and a greater proportion were of ASA grade 1 or 2. Furthermore, our department is not a major trauma centre and as such will not be operating on these higher risk patients. It is perhaps relevant to note that the percentage of patients receiving ACEi or ARB in this study was 27.2% (1692 of 6220) compared with 11.2% in our final cycle population (104 of 928), although this may be a reflection of differences across study populations rather than the effects of our interventions.
Patient sex and ACEi/ARB use were not independent predictors of postoperative AKI development in our study, while diuretic use was found to be significant, in contrast to previous literature6 11 possibly due to our small sample size. Our results regarding the number of risk factor drug classes prescribed concur with those of Bell et al, perhaps supporting our suggestion of a synergistic impact of these drugs on renal blood flow resulting in an increased risk of AKI.6 Our findings support those previously made with regard to the effect of postoperative AKI on length of hospital stay and postoperative mortality.1 3–5
The implications of this QIP are multifold: first, by reducing the incidence of postoperative AKI we hypothesise (based on our findings) that this will subsequently result in an improvement in patient outcomes, namely in length of hospital stay and 1-year mortality. We would argue that these are relatively cost-free interventions; based on a reduction of approximately 40 postoperative AKIs per year within the department and a 7-day reduction in length of stay, these interventions can potentially save 280 ‘hospital bed days’ per year within our department. This equates to potential savings of £86 800 based on bed costs of similar sized hospitals in the area.22 Finally, our findings may support those seen in other literature regarding the possible negative impact of gentamicin as surgical antibiotic prophylaxis on incidence of AKI.15 16 This therefore warrants a review of our prophylaxis guidelines and a discussion with our microbiology department.
We plan on conducting further cycles following a discussion with the microbiology team and engagement with other healthcare professionals on the ward. We aim to collect data on both patients with AKI and patients without AKI in these cycles to determine whether prevalence of AKI risk factors remains low across the patient population. We hope to integrate our interventions with the current ERAS protocol to ensure these measures form part of routine practice within the department. Further studies evaluating the effect of these interventions on reducing length of stay and postoperative mortality as well as the effectiveness in different T&O departments would be beneficial.
Data availability statement
Data are available on reasonable request. Anonymised data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Sandwell and West Birmingham Hospitals Clinical Effectiveness Team (Audit 583). Data were collected as part of an approved quality improvement project/audit. No patient identifiable information was collected and all data were anonymised.
Acknowledgments
The authors would like to thank the Sandwell and West Birmingham Health Information team who played an important role in data collection.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The project was designed by SK, TR and HN. Data collection for the first cycle was conducted by SK, for the second cycle this was done by TR and AL and for the third this was done by SK, DJ, AG and RA. DJ was our information lead and provided anonymous routinely collected data from electronic patient records. Data analysis was conducted by SK. The primary manuscript was written by SK with input from all coauthors. All coauthors contributed to drafting and production of the final manuscript. The project was supervised by HN and SG. SK is the guarantor of this project and responsible for the overall content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.