Article Text

Abstract
In our newborn intensive care unit (NICU), we practise family participatory care, where the unit staff encourage parents and attendants of sick newborns to partner with them and be involved in care for their babies. There remains a concern that this practice may increase the risk of nosocomial infections being carried into the unit by parent-attendants. Staff observed that handwashing behaviours were suboptimal and inconsistent among parent-attendants. With facilitation from an improvement coach, we formed a quality improvement team of NICU staff to improve hand hygiene practices among attendants. From a baseline estimate of around 20% of attendants adhering to hand hygiene standards, the team planned to reach a target of 80% over 8 weeks by introducing a series of changes. At the end of 9 weeks, 80% of attendants were following standard hand hygiene practices.
- Hand Hygiene
- Healthcare quality improvement
- Infection control
- Patient-centred care
- Compliance
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Sick and small newborns admitted to a neonatal unit are vulnerable to infections. Hand hygiene practice by visitors to the unit is an effective practice to curb the spread of infections.
WHAT THIS STUDY ADDS
We describe the details of improving hand hygiene by visitors to a newborn unit that practises family-centred care.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our work describes a methodical approach to measure and improve compliance to hand hygiene practices by visitors to a newborn unit. Teams working in similar areas may use this to guide their improvement efforts.
Problem
We run a referral newborn intensive care unit (NICU) in a central government hospital in New Delhi, India. Sick newborns in need of specialised care (often in a moribund condition) are referred to us from across North India. Since 2012, we have translated and adapted principles of family-centred care (FCC) in our unit.1 FCC in our NICU involves capacitating and thus empowering the accompanying parent-attendant of a sick neonate in care of their own neonate. This is achieved through a structured training of the parent-attendants regarding essential newborn care with help of an indigenously developed audiovisual training module. Practising FCC allows a linkage for a continuum of care at home after discharge. Through a randomised controlled trial, we demonstrated that practising FCC improved breastfeeding rates at discharge and shortened the hospital stay duration of the neonates, without increasing nosocomial infections at our unit.1 There was a concern, however, regarding the hand hygiene practised by the parent-attendants gaining access to the NICU after the implementation of FCC. Lack of timely cognisance and addressing this problem could pose a serious risk of infection to the admitted newborns. This would consequently affect the successful rollout of FCC. We decided to work on taking this up as a quality improvement (QI) project. Just as we had started working on this improvement project, we had to relocate our unit to a newly constructed building in the hospital complex. We aimed to improve the proportion of attendants complying with hand hygiene protocol while entering the unit from a baseline estimate of 20%–80% over 8 weeks (6 June 2016–31 July 2016).
Background
Hand hygiene is critical to infection prevention and control.2 3 It has been proven to be effective in reducing transmission and infections in healthcare settings.4–6 Healthcare-associated infections are a common problem in intensive care units.7–9 Newborns admitted to NICUs are particularly vulnerable to such infections.9
FCC is an increasingly common and globally recommended standard of practice in NICUs.10 11 This emerging practice has also led to concerns about an increased risk of infections for admitted children.12
While the evidence on handwashing is universal, improving practice may require context-specific efforts. Most efforts on improving hand hygiene are focused on healthcare providers. Among the many interventions and strategies identified for improving hand hygiene compliance in patient care, there is limited evidence on certainty about which works better.13 There is some certainty however that strategies involving performance feedback led to better hand hygiene compliance in NICUs.14 There is limited published work on improving hand hygiene among parent-attendants visiting neonatal units in public healthcare facilities in low/middle-income countries.15 16
Measurement
Our key measure was the percentage of observations in which the attendant entering NICU complied with our hand hygiene protocol. Hand hygiene compliance was defined as a parent-attendant performing three distinct actions. The three actions were (1) handwash procedure lasting at least 20 s, (2) covering all parts of hands while washing, (3) gowning to follow and not precede handwashing. The handwash process was considered a ‘pass’ only if the attendant performed all three actions.
While beginning our improvement project, we decided to observe 10 attendants every day as they entered the unit for compliance with hand hygiene practice. These 10 observations were carried out by a designated staff member through each of the duty shifts. Every third, fifth and seventh entry of attendants was observed across each of the morning, evening and night shifts. There was an additional observation of the ninth entry for the morning shift to make a total of 10 observations per day.
We collected baseline data for 3 days across all shifts. Our FCC coordinator observed 30 attendants entering the NICU, out of which 6 were found to be complying with defined hand hygiene protocol. So, we determined our baseline measurement as 20%.
We subsequently started observation using a surveillance camera. Each observation was analysed and confirmed through video retrieval from camera recording, as being compliant or not compliant as per our definition. The review was done two or three times every week from surveillance camera recordings. We entered these data into a computer and generated a time series chart. Our team reviewed this chart in every meeting.
Design
We formed a team consisting of three doctors (one head of the unit and one resident), a research coordinator, two nurses, two mothers of babies whose babies were currently admitted to the newborn unit and one nursing officer in charge. The team met once a week and was guided by an improvement advisor who helped us understand and apply QI methods. In this meeting, they deliberated on the causes for poor compliance, reviewed time series charts, discussed the results for the last change idea tried and planned their next test of change.
We followed WHO’s four-step point-of-care QI method for our QI project.17
Strategy
To better understand the reasons behind the poor compliance of attendants with standard hand hygiene practices, we informally interviewed a few attendants individually and in small groups. We learnt that while they had been taught about handwash and while they believed they were doing it adequately, they were not aware of the reasons why it was so important for the well-being of their sick infant.
We also closely observed and analysed the attendants’ entry process and handwashing technique through video audits. These observations revealed that the sequence of steps followed by attendants was often variable. For instance, some of them wore gowns first, then washed hands and then changed their slippers.
We organised small group discussions with the nurses, doctors and other staff of the unit to understand possible reasons for poor compliance among parent-attendants at entry.
The steps involved in the complete entry process were listed and this was brought to the attention of all staff. The correct process flow that involves steps of removal of accessories (like shawls, sweaters, watch, bangles, etc), followed by changing outside footwear to ones meant for unit use only, followed by handwashing, drying and then wearing a gown became known to all staff.
Clarity with stepwise process flow provided us with an insight into the lacunae with the existing workplace design. Our changing room, handwashing station, shoe racks and entrance were not located in a linear sequence. This made attendants’ compliance with washing hands only a random event (figure 1).

NICU workspace before and after improvement efforts. FCC, family-centred care; KMC, kangaroo mother care; NICU, newborn intensive care unit; SNCU, sick newborn care unit
We employed the opportunity of relocation of our unit to a new block in our hospital, for planning to redesign the entry area in consonance with the process flow steps for entry (figure 1). The lockers, slipper change area, the handwashing station with soap, drying area and gowns were now kept in a linear sequence. The gowning area was deliberately placed in the next zone following the handwash area to preclude any possibility of an attendant skipping handwash and directly going for a gown change. We also installed surveillance cameras near the entry area to capture entry to the unit and our handwashing area in a single frame. This made it easy to for us to record and study hand hygiene compliance at entry.
On reviewing our key indicator, we observed that the new design of the unit led to an increase in compliance of 40% for a week. The following week, however, compliance to hand hygiene protocol was again down to the baseline of 20%.
In the third week of our attempts to improve, the team added a component of educating mothers about the importance of handwashing as an important step for keeping their newborn safe, to the existing training content. We brainstormed new ideas to improve their handwashing skills. We have a routine orientation and training session for all attendants of babies at admission to the unit. This is aided by an indigenously developed audiovisual training tool that has been developed for structured training of parent-attendants participating in FCC. We realised we needed to make this training more interactive to impart key skills on hand hygiene. We added a step-by-step demonstration in training even in the handwash area. We pasted an illustrative handwashing poster just above the scrub station. Most of our training sessions were carried out by one staff member. We tried to rotate trainers frequently and checked if that could bring improvement. These ideas worked, and there was an increase in compliance with hand hygiene to 50% that week.
Heartened by this success in improving the orientation training for attendants, we made a further attempt at making it more interactive. In the fourth week, we introduced a session on peer-to-peer demonstration of washing hands by attendants. We expected attendants to be able to learn better from their peers. This further improved handwashing compliance. Sixty per cent of observed entries were now seen complying with our hand hygiene protocol.
On suggestion from our unit head, we next tried using GloGerm, a proprietary product that when applied to hands, glows in ultraviolet (UV) light. The user must apply this to their hands and then wash their hands as they would. Any remnant product on the hand could be seen under UV light signifying the unclean areas. This could help the user understand whether their handwashing was thorough or not. We asked attendants to apply GloGerm before washing hands and then examine it using a UV light torch, to look for areas of hands not cleaned by using soap. We expected this practice to provide them objective feedback on how well they were washing their hands and lead to better handwashing. The idea did not work out well because of inadequate and irregular GloGerm supplies and difficulty in using a UV torch. Some team members also thought that this would be expensive to sustain in our unit.
By this time, in week 5 of our efforts, hand hygiene compliance continued to range between 40% and 60% per our continued surveillance video review. Seeing no improvement and anticipating logistical and operational hurdles in the use of GloGerm, we dropped this idea.
One of our team members recalled that peer-to-peer sessions in our routine training were working well. They suggested we could extend this idea beyond the training sessions. We asked attendants to observe each other as they enter the unit and point out if they saw anyone not complying with the defined hand hygiene process. In 2 days, we learnt that this led to unruly arguments among the attendants. In the next morning’s training session, we advised attendants to stop this practice. We later learnt that this had not led to any improvement in the proportion of observations compliant with the protocol.
Around this time, our staff had identified specific attendants who were not following hand hygiene practices. Until now, our training sessions had a standard demonstration video on good handwashing techniques. We now decided to show our training participants a recording of how they had washed hands from surveillance video footage of the last few days. We believed this would help them self-evaluate and understand the exact steps of handwashing that they were not performing correctly. We tried doing this for 1 day and it resulted in those attendants not feeling good about it. They felt embarrassed about being pointed out in a group as being the ones responsible for potentially carrying infections inside the unit. We immediately abandoned this change. Our data chart showed that compliance rates were stuck between 50% and 60%.
After a long discussion in our team meeting next week, one of the team members proposed a different iteration of this idea. She suggested we use footage showing the good technique of handwashing of an attendant. This would give the participants motivating feedback while avoiding anyone being embarrassed. We decided to try using the footage of an attendant who was not present in the training session. The sessions went well, and our trainer could observe participants keenly paying attention to this video clip.
Using this third-person footage helped us increase hand hygiene compliance further. In our team meeting this week, we reviewed our data and saw compliance improving to 70%. We integrated a session on showing this footage in our daily training sessions for attendants and saw our compliance rates improving further to range between 70% and 80%. Various interventions and their impact are depicted in table 1.
List of change ideas developed by the QI team to improve parent-attendant compliance with handwashing
Results
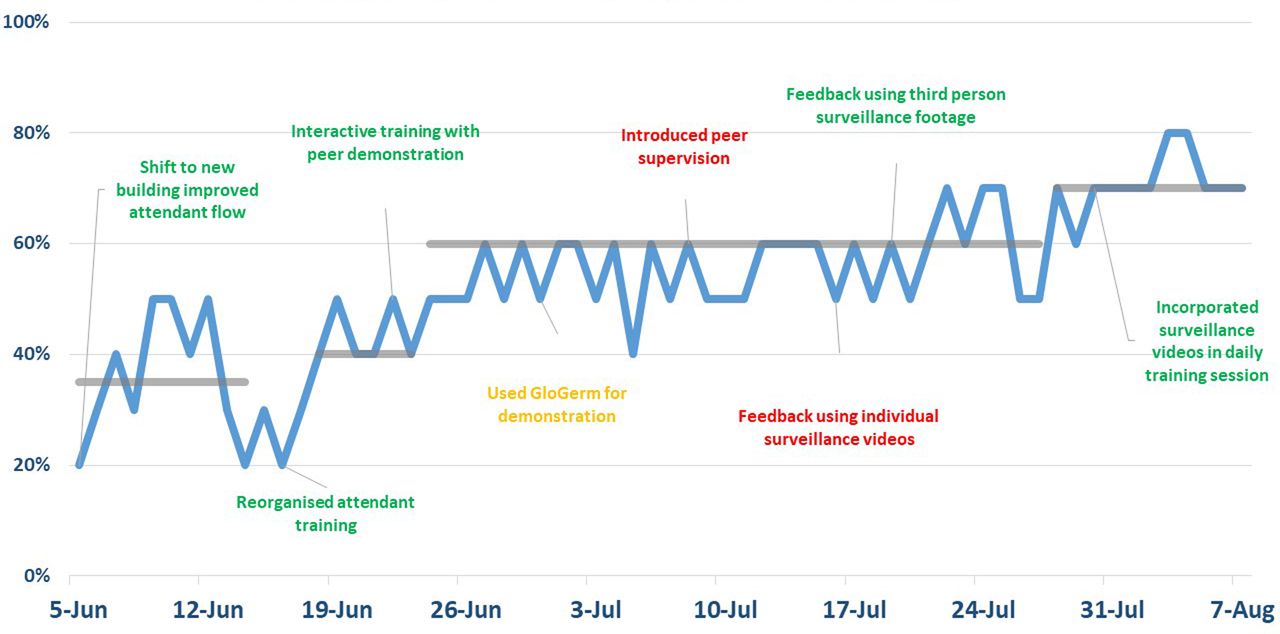
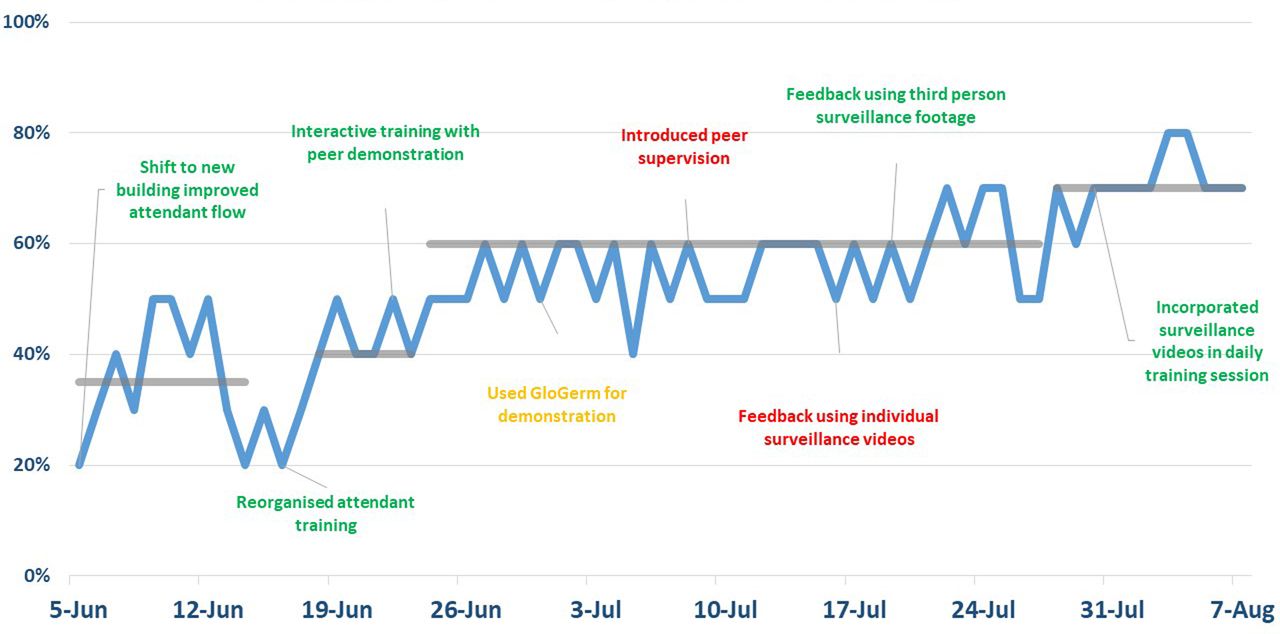
In 9 weeks, since we set out to improve hand hygiene among parent-attendant, our team achieved their quality aim. Eighty per cent of attendants were now following standard hand hygiene practices while entering the NICU (figure 2).
{kind=link}
{kind=link}
Proportion of observed attendants who follow hand hygiene protocol before entering NICU, Dr RML Hospital, 5 June 2016–7 August 2016. NICU, newborn intensive care unit; RML, Ram Manohar Lohia.
Lessons and limitations
Our work demonstrates the need to focus on the details of implementing changes in a microsystem. It also shows how important it is to understand the interplay between the context and the client’s behaviour.
There are many ways to measure handwashing. Mainly these include measuring product use, observation-based data collection on the process and measuring outcomes related to poor handwashing.18 Our work used only indirect observation of the process as a measure. We considered monitoring handwashing-related outcomes for our project but shelved this after a discussion among our team members. Our unit admits newborn babies born in other hospitals and referred to us as a last resort. In most cases, these babies already have infections at admission. Linking our handwashing work with any changes in infection-related outcomes would not have been directly plausible.
Measuring the consumption of handwashing soap might have been a good indirect measure to help us validate our sample video surveillance observation data.
During our QI team meetings and discussions with staff outside of the team, we understood that our staff believed there was excessive consumption and likely wastage of soap because of this project. They also shared that these improvements have also led to staff washing their hands more frequently and thoroughly. We measured the handwashing percentage in the same manner as described, at least once a few months after the project. We found it close to 80%. Thereafter, good hand hygiene practices have become a culture in our NICU. Hence, we did not feel the need to revisit this. In our unit, we have security staff posted at entry near the handwashing station. They revealed that this may have led to a drop in unnecessary visitation to the unit as attendants now believed they were being watched.
Conclusion
Proper hand hygiene is the single most important, simplest and least expensive means of reducing the prevalence of healthcare-associated infections and the spread of antimicrobial resistance.19 The use of QI methods can help in overcoming context-specific challenges in implementing good hand hygiene practices.
We continue to implement the changes we found successful to sustain improved handwashing in our unit. We have revised the curriculum for attendant training sessions which now have more demonstrations and interactive sessions. We routinely rotate our trainers for these sessions and have developed a guidance document for new staff who would be assigned to do this work in future.
In a qualitative study conducted to assess the acceptability of family-centred newborn care among providers and receivers, we found that the efforts to build the capacity of attendants in our unit led to a sense of self-efficacy and empowerment among them. The practices they learn during their baby’s stay in our unit, particularly handwashing, are continued even after discharge from the hospital.20
Our unit has led work on FCC for sick and small newborns admitted to neonatal units in India. We plan to further use QI methods in improving components of FCC. We also plan to share our experience with other neonatal units in India.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
Exemption granted by the Institutional Ethics Committee in view of a quality improvement initiative.
Acknowledgments
The authors thank all babies admitted to the neonatal unit, their parents and the staff involved in care. Ankur Sooden provided on-site coaching for this work with the support of the American people through the US Agency for International Development (USAID) under the USAID ASSIST Project managed by University Research Co under Cooperative Agreement Number AID-OAA-A-12-00101.
References
Footnotes
Twitter @AnkurSooden
Contributors AM accepts full responsibility for the work, had access to the data, and controlled the decision to publish. AM and AS conceptualised this work and drafted this manuscript. AM, AS, RW, RK, KL, VN and IG contributed to the quality improvement project.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.