Article Text

Abstract
Falls are common and preventable adverse events that occur in a hospital setting. Falls can cause pain, damage, increase cost and mistrust in the health system. Inpatient fall is a multifactorial event which can be reduced with multistrategic interventions.
In this project, we aimed to reduce the fall rate in paediatric ward of Jigme Dorji Wangchuck National Referral Hospital, Bhutan by 25% from the baseline over a period of 6 months by focusing on fall risk assessment, staff education on fall prevention measures and devoting more attention to patients at high risk of fall.
We tested three sets of interventions using the Plan–Do–Study–Act approach. For the first cycle, emphasis was on staff education in terms of proper use of fall risk assessment form, risk categorisation and fall prevention advice. In the second cycle, in addition to the first we introduced the ‘high risk of fall package’ and the third cycle focused on early and easy identification of high-risk patients by continuous fall risk assessment and use of high risk of fall sticker.
We observed that at the start of the quality improvement project despite our intervention the fall rate of our ward went up but as we continued adding more ideas focusing on high risk patients, we could achieve a fall reduction of 49.3% from the base line by end of third cycle. Our ward saw fall free days of almost 90 days at the end of project.
We conclude that inpatient falls occur due to multiple factors therefore a multi-pronged strategy is needed to prevent it. One of the prime preventive strategy is identifying patients who are at high risk of fall and concentrating attention to those patients.
- healthcare quality improvement
- paediatrics
- patient safety
- PDSA
- quality improvement
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. ‘Not applicable’ data are included within the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Children in hospitals are at risk of fall and it leads to additional physical, emotional and financial burden to already sick patients and their worried family members. Every healthcare centre around the world are striving to reduce the incidence of preventable falls by using different methods/approaches.
WHAT THIS STUDY ADDS
This project highlights that in a resource-limited setting/low-income and middle-income country, carrying out a simple multidisciplinary quality improvement (QI) project (Plan–Do–Study–Act cycle), which has minimal or no additional financial implication to the institute is one of the cost-effective approach in reducing fall rate.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The positive result of this fall prevention QI initiative will motivate and provide directions to healthcare workers/policy makers in my country and other low-income and middle-income countries to implements similar cost effective ideas and bring an improvement in the healthcare delivery.
Problem statement and rationale
The increasing fall incident rate at the paediatric ward of Jigme Dorji Wangchuck National Referral Hospital (JDWNRH) was of great concern to all those involved in the patient care. It questioned the safety domain of care we were providing to our patients. JDWNRH is a 350 bedded tertiary level government Hospital in Thimphu, capital city of Bhutan. JDWNRH receives patients from different parts of the country for diagnostic and management care. The 33 bedded paediatric ward admits patients from 1 month to 12 years of age. The ward is manned by 3–5 nurses and paediatric residents and consultants on rotation basis. Paediatric ward had a baseline fall rate of 3.08/1000 patient-days which is noticeably higher than the fall rate reported from other countries. Keeping in mind that clinical safety is an essential component in delivering safe healthcare services, we planned this inter-professional quality improvement (QI) initiative with an aim to reduce the fall rate in paediatric ward by 25% from the baseline over a period of 6 months.
Background
A fall is ‘an unplanned descent to the floor, either with or without patient injury’.1 Falls are common adverse events that occur in any hospital setting and it accounts for 42% of all cases in paediatric ward.1 In paediatric patients, the fall rate has been reported as 1.36,2 0.573 and 0.56 to 2.19.4 The formula ‘falls × 1000/patient-days’ is used to calculate the fall rate.5 Falls in a healthcare system reflects failures in organisational process and structures. Falls lead to negative consequences like pain, injury, increase costs and lack of trust in the health system.6
As children go through various developmental stage with difference in their physical and cognitive abilities to approach mobility, this puts them at higher risk of fall.7 Medical equipment which are attached to them, sedative medication and unattended toileting needs further increases the risk of falls when they are admitted in hospital.8
Clinical safety, as one of the crucial dimensions of quality healthcare, focuses on identifying patients at risk of fall and mitigating the risks factors.9 Study shows that almost half of the falls can be prevented with proper design of the process and the system.9 10 Fall risk assessment, categorisation of patients into high risk and low risk and appropriate intervention for different groups is the foundation of any falls prevention programme.11 Identifying patients at risk of fall by proper fall risk assessment and diverting more attention to them leads to decline in the fall rate by approximately 19%.12 The Humpty Dumpty Fall Scale (HDFS) is one of the tools used in paediatric patients to assess fall risk. The tool consists of components such as age, sex, diagnosis, cognitive impairments, environmental factors, response to surgery/anaesthesia/sedation, and medication usage for which different scores are given. Score of <12 categorises a patient as low risk and score >12 categorise as high risk.13 Basic fall prevention measures for the those at low risk of fall consists of patient orientation to the room, environment safety by clearing of clutters around the patient bed, use of non-skid slippers while ambulating, patient and family education on fall risk prevention measures. For the high-risk patient additional measures are use of a high-risk signage/sticker (‘Humpty Dumpty’ sticker) on the patient’s bed and chart for identification, frequent rounding of patient, ambulation with assistant and moving the patient closer to the nursing station Overall, evidence strongly suggests that implementation of a paediatric fall prevention programme using an effective tool such as the HDFS leads to increased awareness among the healthcare providers in identifying patients at risk for fall and there by act on preventive measures to reduce the fall incidences in inpatient paediatric population13 14 Falls in hospital cannot be entirely prevented however we can work on reducing the fall rate by putting in different measures as above.
Specific aim
This QI initiative aimed at reducing fall rate among patients in paediatric ward by 25% from the baseline within 6 months (From July to December 2021).
Method
This QI study was carried out in the paediatric ward of JDWNRH, Thimphu. Bhutan. JDWNRH is a 350 bedded tertiary level government hospital in Thimphu, capital city of Bhutan. JDWNRH receives patients from different parts of the country for diagnostic and management care. The paediatric ward had 33 beds and admits patients from 1 month to 12 years of age The average monthly patient admission is about 80–110 patients. The ward is manned by 3–5 nurses and paediatric residents and consultants on rotation basis. The common problems seen among the admitted patients are pneumonia,gastroenteritis, urinary tract infection,glomerulonephritis, nephrotic syndrome, meningitis, encephalitis, seizure disorders, failure to thrive and surgical condition like abscess, burns, appendicitis and gastrointestinal obstruction.
Measurement
This QI project looked into the outcome measure which was ‘fall incident rate’. Fall rate is reported as per 1000 patient-days.
Numerator=number of inpatient falls.
Denominator=total patient-days.
Fall rate=number of inpatient fall/total patient-days × 1000.
At the start of project, the data for last 6 months were extracted from fall excel sheet maintained by the ward in-charge and from the admission register and baseline fall incident rate calculated as 3.08/1000 patient-days.
During the QI period, data on number of daily fall and daily patient-days were collected from the ward fall and admission excel sheet and entered into predesigned daily data collection sheet. At the end of the each month, data were compiled in a monthly data compilation sheet and fall rate calculated.
Design
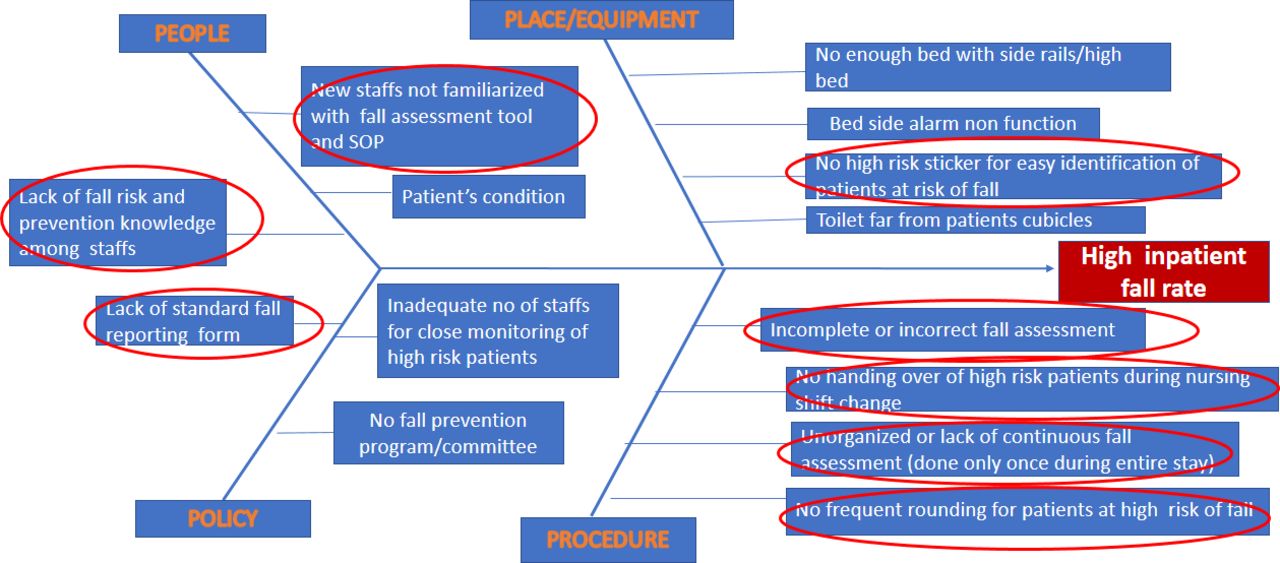
The following steps were implemented phase wise during the project: (1) Formation of interprofessional team comprising of ward in-charge, paediatrician, paediatric resident and paediatric nurses; (2) Studying the baseline fall rate by collection of data from the admission register and fall excel sheet of the unit; (3) Root cause analysis using fishbone diagram and literature review; (4) Meeting of QI members and the ward nurses to decide on the doable intervention and (5) Testing change ideas using multiple Plan–Do–Study–Act (PDSA) cycles.
Strategy
The root cause analysis pictured multiple cause for high fall rate in our ward. We targeted our intervention on causes which were implementable and doable at our level as highlighted in figure 1.

Fish bone analysis and targeted intervention.
Three PDSA cycle were tested with different change ideas as below (tables 1–3).figure 2
First PDSA cycle (July 2021)
Third PDSA cycle (October 2021)

Run chart showing the fall incident rate by month. PDSA: plan-do –study-act.

{kind=link}
{kind=link}
{kind=link}
High risk of fall sticker used on a patient's bed.
Second PDSA cycle (August 2021)
Intervention package for ‘high risk of fall’ patients
Total patient admission for July was 137 with Fall incidence rate of 3.11/1000 patient-days.
The total patient admission for August was 103 with fall incidence rate of 2.5/1000 patient-days. This was about 28% reduction from the baseline.
September: In September, we continued with the above interventions to see how it will works. The total patient admission in September was 99 with fall rate of 3.8/1000 patient-days. Due to increase in fall rate, we planned third PDSA cycle with addition change idea for October.
The total patient admission in October was 101 with no fall incident reported in the entire month.
For the month of November and December, the total patient admission was 94 and 109, respectively, and there was no fall incidence for November and December too.
Results
Paediatric ward, JDWNRH had a baseline fall incident rate of 3.08/1000 patient-days during last 6 months prior to this QI project. In July (first PDSA cycle), the total admission was 137 with 39 patients (28.46%) categorised as high risk of fall and fall rate reported was 3.11/1000 patient-days, a marginal increase from baseline. In August, the total admission was 103 with 20 patients (29.12%) categorised as high risk of fall and fall rate reported was 2.5/1000 patients. By the end of second PDSA cycle, there was reduction in fall rate by 28% from the baseline. The total admission in September was 99 with 34 patients (34.3%) categorised as high risk for fall and fall rate reported was 3.8/1000 patient-days. Due to increase in fall rate in September, a third PDSA cycle was planned for October. In October, the total admission was 101 with 35 patients (34.6%) categorised as high risk of fall. There was no fall incident in October. The QI project was continued till the end of December incorporating the change ideas of all three PDSA cycle. For November and December, the total admission was 94 and 109, respectively, with high-risk patient percentage of 26.59% and 32.1%, respectively, with no fall reported in both the months. By the end of the project we had a fall free days of almost 90 days. The average fall rate for the QI period (July to December 2021) was 1.56/1000 patient-days (around 49.3% reduction from the base line). The month wise trend of fall incident rate is depicted in the run chart (figure 2).
Discussion
This goal of this QI project was to reduce the fall rate in paediatric and improve the safety domain of the healthcare services. There are multiple risk factors for falls in hospitalised patients including intrinsic and extrinsic factors and associated comorbidities.15 As per literature review, the fall reduction needs multiprofessional team approach, proper fall risk assessment and implementation of preventive measures and communication of fall episodes.16 This QI project also had a multiprofessional team approach with focus on proper fall risk assessment using HDFS and implementation of fall preventive measures. Similar to other QI projects on falls, with the use of the HDFS and by focusing on high risk patients, we also saw a reduction in fall rates from 3.08 to 1.56/1000 patients. Initially as we started the QI project, there was an increase in the fall rate and this can be explained by the increased awareness on fall reporting and uniform reporting of fall incidents, even those without injuries. One of the previous study gives a similar report that falls in children are sometimes considered normal, and if not associated with injury are unlikely to be reported. The reported rate of incidents can go up with proper education, awareness and interventions.17
The increase in the fall rate (3.8/1000 patient-days) in the month of the September could be explained by having more high risk for fall patients in this month (34.3% were high risk) and not yet having a system of easily identifying them for intervention. Once the additional idea of using a visual signage (high risk sticker) for high-risk patients was started from October, we had a consistent result with no fall reported for October to December.
Studies have highlighted that to prevent and reduce fall rates, multiple kinds of ideas and intervention like nurses and parents education, use of a validated fall risk assessment tool and focusing on high-risk patients is the key to success.2 14 15 Likewise our QI project had a positive impact in reducing fall rate with implementation of similar ideas and interventions.
Lessons
Forming a multidisciplinary team is of paramount importance in making any project successful and bringing change to the system. Having the ward in-charge and paediatric resident as the members of our project added strength to the project as they could disseminate the new change ideas to their colleagues working in the ward more effectively. This project also taught us the significance of doing things systematically in order to achieve our target. Preventing falls is not a single person’s task. Rather, fall prevention requires the active engagement of many individuals and teams involved in caring for the patients. The support and cooperation rendered by all the staffs of paediatric ward while implementing the QI initiative was instrumental in achieving the success.
Limitations
Although this QI project was successful, there are some limitations and challenges. (1) Collecting a baseline data on fall rate was very taxing as there was no separate fall incident report form and no uniform reporting system in the unit. (2) The project only looked into the outcome indicator (fall rate) but looking into process indicators is equally important to have a bigger impact on fall reduction. (3) As we reflect back we wish we could have given more time for each new ideas to sip into the system and studied the result but due to time constraint we landed up testing several ideas together within a short span of time. (4) The project was carried out in the midst of the COVID-19 pandemic and each member were occupied with their own duties so we confronted trouble in organising meeting in person never the less we overcame this challenge by using virtual means/social applications for discussion.
Conclusion
Patient safety in the hospital setting is a priority in any healthcare. The hospital environment places patients at increased risk of fall.14 Inpatient fall is one of the common adverse event leading to wide gap in the safety domain of any healthcare setting worldwide. Considering the increasing fall rate in paediatric ward, JDWNRH, this QI initiative was taken up with the aim to reduce the fall rate and there by deliver safer healthcare services to our patients. PDSA cycle approach was used for our project to test new change ideas like uniform and continuous fall risk assessment, risk categorisation, fall prevention advises, using of high risk of fall sticker and high-risk intervention package. The average fall incidence during the project period (July to December 2021) declined to 1.56/1000 patient-days, which was 49.3% reduction from the base line.
We conclude that carrying out a systematic fall risk assessment with risk categorisation and diverting more attention to those patients who are at high risk of fall can prove to be an effective approach in reducing the incidence of falls. Using the Model for Improvement through PDSA cycles can be an effective way to bring quality changes to our work place and the system.
Sustaining any change in a system needs simple and cost-effective measures along with regular monitoring. Keeping this in mind, we have put in some simple cost-effective and undemanding measures to sustain the positive impact this project. (1) Reviewing of fall incidence data and taking corrective measures on quarterly basis. (2) Briefing of all new nursing staffs and residents on fall assessment tools and fall prevention measures and advices when they join our unit. (3) Appointing a ‘fall champion’ for our ward who will look after fall related matters and coordinate the quarterly fall review meeting. (4) Incorporating the new change ideas in our existing fall SOP standard operating procedure so that it is uniformly practised by all.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information. ‘Not applicable’ data are included within the article.
Ethics statements
Patient consent for publication
Ethics approval
The Medical ethics research unit, JDWNRH and the Research Ethics Board of Health (REBH), MOH, approved the project.
Acknowledgments
We wish to express our sincere gratitude to Quality Assurance and Standardisation Division (QASD), JDWNRH for giving us the opportunity to carry out this project. We also extend our sincere thanks to Dr.Yoriko Nishizawa, Neonatologist, FoPGM, Khesar Gyalpo Medical Sciences of Bhutan for the guidance rendered to us throughout the project. Lastly the project could not have been completed without the participation and support from the nursing colleagues of pediatric ward. Their contribution to this project is gratefully acknowledge.
Footnotes
Contributors KC, UR, GL, BK and SD contributed in designing the overall QI project and studying the root cause analysis. UR, BK and SD Contributed in data collection. KC, GL and BK participated in developing the tables and figures. All the authors participated in drafting and revising the manuscript. All authors reviewed and approved the final version. Guarantor:KC
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.