Article Text

Abstract
Introduction Hospital use increases with age. Older people and their families have reported poor experiences of care at the time of discharge home from hospital. As part of a larger project, we established and evaluated a quality improvement collaborative to address hospital to home transitions for older people.
Methods We convened an expert panel of 34 stakeholders to identify modifiable issues in the hospital-home transition period. We established a collaborative involving health professionals across a range of agencies working to common goals. Teams were supported by a network manager, three learning sessions and quality improvement methodology to address their identified area for improvement. We used mixed methods to evaluate whether the establishment of the quality improvement collaborative built networks, built capacity in the health professionals and improved the quality of care for older people. Evaluation methods included interviews, surveys, network mapping and case studies.
Results Nine teams (n=41 participants) formed the collaborative and attended all meetings. Mapping showed an increase in networks between participants and organisations at the conclusion of the collaborative. Interview data showed that building relationships across services was one of the most important parts of the collaborative. Survey results revealed that most (77%) believed their quality improvement skills had developed through participation. Advice and regular meetings to progress project work were considered important in ensuring teams stayed focused. In terms of improving the quality of care, some participants indicated that they achieved the stated aims of their project better than expected (21%), most (41%) felt they achieved their aim as expected, 26% got close to their aim and the rest did not know the outcome (13%).
Conclusions Establishing a quality improvement collaborative was a positive activity in terms of building a network across organisations and progressing quality improvement projects which aimed to achieve the same overall goal.
- quality improvement
- healthcare quality improvement
- quality improvement methodologies
- qualitative research
Data availability statement
Data are available on reasonable request. Excerpts of deidentified data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- quality improvement
- healthcare quality improvement
- quality improvement methodologies
- qualitative research
Key messages
What is already known on this topic?
The transition from hospital to home can be a difficult time for older people and is complicated by the fragmented nature of health and aged care services. Local solutions to improve transitions and prevent avoidable hospital readmissions may be required.
What this study adds?
We showed that coordinating efforts to prevent avoidable admissions through a quality improvement collaborative was an effective way of building relationships between services. A network manager employed to support the collaborative provided the encouragement, reminders and connections across services that helped teams progress their projects.
How this study might affect research, practice or policy?
While individual services can address parts of the hospital to home transition process, creating relationships across services may be more effective in improving quality and preventing readmissions.
Background
Hospitals account for the greatest proportion of health costs in Australia and public hospitals received AUS$57.7 billion in funding in 2017–2018.1 Hospital use increases with age and older people account for approximately 41% of overnight hospitalisations.2 Research shows that a number of factors increase the risk of hospitalisation for older people. These include: older age, being male, having lower levels of education, living alone, having multiple comorbidities and having a recent hospitalisation.3–5
Older people typically spend longer in hospital6 and are at risk of complications such as falls,7 delirium,8 functional decline9 and medication related harm.10 These adverse events can have long term consequences such as long-term disability or triggering a move to a residential care home. Older people describe negative experiences during a hospital admission and report feeling insignificant and powerless during their stay.11 This continues after discharge from hospital with people reporting that the transition home is often difficult and complicated by poor communication between the hospital, caregivers, home support services and their primary care practitioner.12
The negative impact of potentially preventable hospital admissions for both older people and the health system means that there has been significant interest in reducing these admissions. However, systematic reviews of studies which aim to prevent hospital readmissions have shown mixed results. Linertová et al found that neither hospital-based approaches (eg, geriatric assessment, comprehensive discharge planning) nor home-based approaches (eg, outreach teams) consistently achieved desired outcomes for older people.13 They concluded that success may be linked to targeting interventions to those most in need rather than ‘one size fits all’ approaches. An Australian think tank on the issue concluded that a ‘whole of system’ approach was required with better integration across primary and acute care with improved engagement between service providers, patients and carers.14
The work described in this paper was part of a larger programme of work, the State Action on Avoidable Rehospitalisations and Unplanned Admissions (STAAR-SA) project, which aimed to address avoidable admissions for older people in South Australia.15 A network of people involved in hospital admissions and transitions was established comprising healthcare professionals from primary, acute and community care, researchers, aged care and community care organisations, consumers and consumer advocacy groups. The STAAR-SA programme of work is described elsewhere15 but in brief involved (1) using registry data to profile individuals at risk of admissions, (2) evaluating the effectiveness of existing out-of-hospital programmes within the state and (3) implementing a state-wide quality improvement collaborative (QIC) to improve care for hospitalised older people. This paper describes the process and outcomes of the STAAR-SA QIC.
QICs are a popular method of tackling healthcare problems in a twice daily to improve care. Small teams from multiple settings and/or sites are brought together to address a specific, common issue. The teams are supported by experts and involved in structured activities, usually over a course of several months. Teams are guided to assess their own performance, develop strategies to improve performance, trial strategies, evaluate progress and continue this cycle as required. QICs have been applied in a number of settings and overall outcomes are positive with a systematic review finding that 83% of studies reported improvements in one or more outcomes.16
The aim of this project was to establish and evaluate a state-wide QIC to improve the quality of care for older people at times of transition between hospital and usual living environment (home or residential care home).
Methods
Aim
This study took place in South Australia and was guided by a project steering group. Stakeholder meetings occurred regularly and group newsletters providing updates on the project were sent to a large group of interested parties.
The aim of the STAAR-SA QIC was to align quality improvement activities with priority areas identified by topic experts. The objectives were to:
Improve networks between different health and aged care services involved in hospital transitions for older people.
Build capacity in the workforce to undertake quality improvement projects.
Improve the quality of care for older South Australians at the time of transition.
Patient and public involvement
This study involved an expert panel to guide the process of QIC and multidisciplinary groups as QIC participants:
Guiding the process: an expert panel
Prior to establishing the QIC, we convened an expert panel to inform who should be involved, what work could be done to improve care and advise on what outcomes the collaboratives should strive to achieve. We invited 34 people to attend the panel discussion, from a diverse range of sectors across metropolitan and regional South Australia, including primary and allied health, aged care, consumer advocacy, government and non-government services and academia. The panel was provided with a summary of the programme of work, data about predictors of hospital admission in older people in South Australia and a summary of the evidence for interventions to prevent or reduce admissions. The expert panel was separated into four small groups: two groups with expertise in community care and two groups with expertise in residential care. Groups were asked to map a planning diagram in which they identified the main problems in preventable admissions, readmissions, and transitions. They then reported back to the larger group on the main problems identified. The whole group was then asked to vote on the most important modifiable problems for each population. Results of voting are presented in table 1. The panel members were then asked in their small groups to brainstorm how to measure change for these important modifiable problems; notes were shared with the project team at the end of the panel.
Expert panel voting results: main modifiable problems
QIC participants
Calls to participate in the QIC were advertised beyond the STAAR-SA project team to the stakeholder group who were asked to promote the activity within their networks and/or nominate teams to be involved. Self- nomination was also accepted. We invited multidisciplinary groups whose scope of work involved working with older (aged 65+) South Australians at some point during hospital transition to be involved in the project. Where health professionals were interested but did not yet have a dedicated team, the network manager who was appointed to support STAAR-SA QIC helped them to form teams with relevant stakeholders. We aimed to recruit a range of health professionals including hospital medical specialists and general practitioners, nursing, allied health, paramedics and health managers. We also invited consumers to participate in the collaborative meetings so that they could share their advice and experience with the teams. Two consumers attended the learning sessions and were also available to provide individual support to teams. In addition, we encouraged teams to link with consumer representatives in their own organisations.
The network manager was embedded in the state health department and was an experienced allied health professional with over 30 years’ experience working within government health roles. Following recruitment of teams, the role of the network manager was to communicate regularly with the groups to provide encouragement, support and share knowledge, to connect groups with other relevant parties and other groups with shared goals or interests.
The QIC team members were asked to identify an issue linked to the modifiable problems identified by the expert panel and to test ideas using a 'proof-of-concept’ approach that had the potential to improve quality of care and reduce unplanned admissions and representations for older people. The QIC projects were initiated from the ‘ground up’ by health professionals working directly with clients and who were acutely aware of the issues facing older people at times of transition. Each QIC team (the Project Team), consisted of 3–5 project team members and a project lead. Each project also had an executive sponsor such as a senior geriatrician or a department head. The role of the executive sponsor was to support the QIC project, promote the activity at a senior level and consider opportunities for sustainability.
QIC learning meetings
Members of the QIC were invited to attend three group learning meetings over 10 months (see: timeline in online supplemental appendix 1). These meetings were held face to face and lasted approximately 3 hours each. The first meeting involved introductions and presentations from the project steering group regarding the evidence around hospital admissions in older people and recommendations from the expert panel on priority areas. In addition, attendees were presented with information about QICs and quality improvement methodology. At the conclusion of the first meeting the Project Teams used a template to begin to develop their project plan. The template required participants to state their problem, breakdown the problem, set a target, undertake a root cause analysis, plan intervention, intervene (using iterative Plan, Do, Study, Act, PDSA cycles) and evaluate. At the first meeting participants were asked to complete the template to the point of intervention planning. The second meeting provided an opportunity for the Project Teams to meet and share information about project progress including barriers and enablers. The third meeting involved each group sharing information about the outcomes of their projects with the other groups and discussions about sustainability.
Supplemental material
Evaluation methods
This mixed-methods evaluation used surveys, field notes, case studies, mapping and interviews to gain information about whether the QIC achieved its intended objectives. Objectives and methods of measurement are outlined in table 2.
Research objectives and approach to measurement
Survey
The same survey was used to measure the outcomes of objectives 1 and 2. The survey included a mixture of likert scales and open-ended questions (online supplemental appendix 1). The survey was built in Qualtrics, and an electronic link emailed to all participants in the QIC by the project steering group at the conclusion of the project. Responses were anonymous. Data were presented descriptively in tables. We also sent an electronic questionnaire asking participants in the QIC to map their relationships with other service providers prior to and following the project. We asked participants to do this retrospectively (ie, ‘before working with the project, please indicate your relationship with the following organisations’ and ‘after working with the project, please indicate your relationship with the following organisations’). Relationships were plotted visually.
Interviews
Interviews with project leads and the network manager were conducted by a research assistant (JR), audiorecorded and transcribed. In-person or videoconferencing methods were available depending on the preference of the project lead. Two members of the team (JR and KL) reviewed the transcripts and coded information in NVivo. The codes were discussed by KL and JR and key themes identified in relation to the research questions. Discussion then occurred with the wider research team.
Case studies
The network manager provided each team project lead with a case study template in which to report the outcomes of their project. The project lead completed this with assistance from the network manager as required.
Results
We recruited 41 health or aged care workers who formed 9 quality improvement teams. As three of the teams shared similar aims they worked together as a larger team as indicated below. There were no withdrawals of teams between the first learning session and the completion of the project and all teams adopted the suggested approach of intervening using PDSA cycles. The aims of the teams are presented in in online supplemental appendix 1.
Survey responses
Surveys were sent to 41 participants in the QIC. At the conclusion of the project a total of 35 people completed the survey (response rate 85%). Most (n=25, 71%) of these were project team members and the remainder were project leads. At least two respondents from each project team completed the survey (range 2–6).
Interviews were conducted with the nine project leads (n=9, 100%).
Did the QIC improve networks between services?
Results of the survey suggested that most participants had a better understanding of local organisations and that the activities of the QIC had led to improved relationships with key stakeholders (as presented in table 3).
Most (74%) respondents reported that they were probably, or definitely likely to maintain these relationships after the QIC ended. All respondents (100%) reported that contact from the network manager was helpful. Survey responses included that the network manager helped direct effort, maintain focus, and drive the project forward when teams lacked the time to do this themselves. In terms of creating a network, the manager brought participants together within services and across local health networks and assisted with standardisation of approaches across the state. The manager outlined how ‘There might have been some things where I used my networks to find out information for them’ (Participant3). The network manager also directly supported teams with setting up databases to track progress. On a personal level, teams found the manager warm, supportive, encouraging, well-connected and knowledgeable.
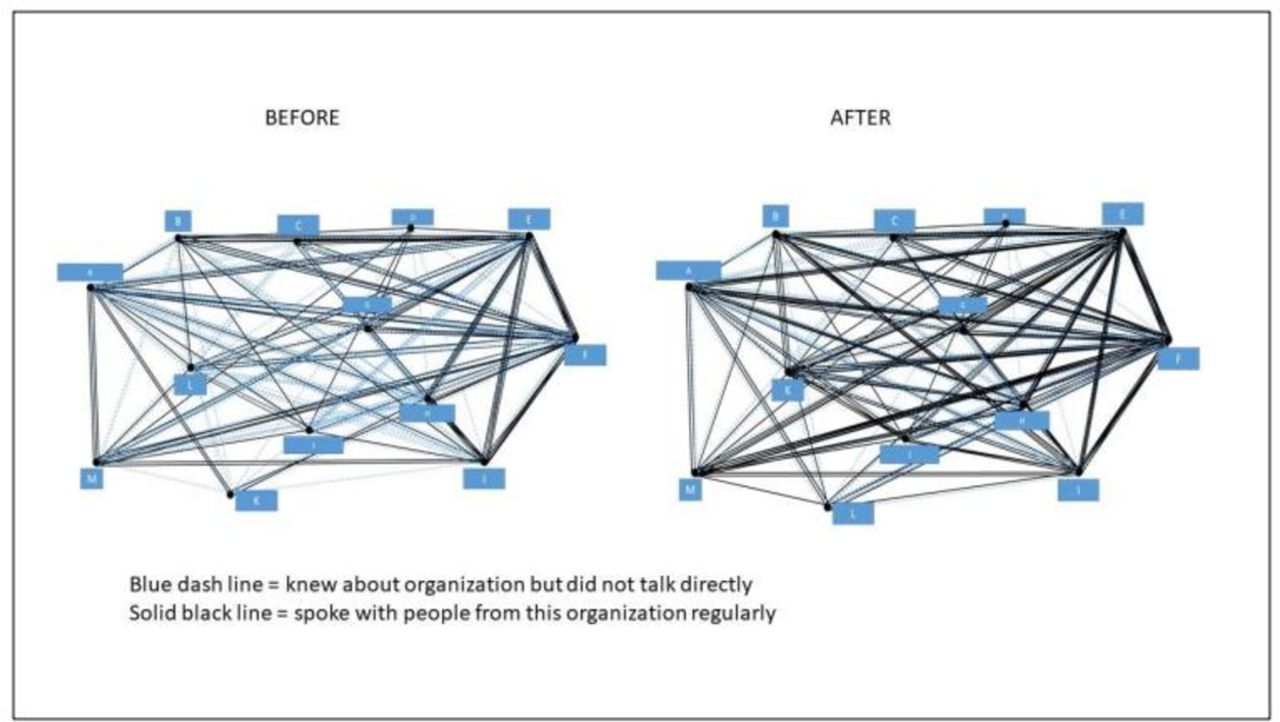
We received 37 responses to the electronic questionnaire ascertaining relationships with other service providers before and after the QIC. Results are presented in figure 1.
{kind=link}
Relationships between participants from the organisations before and after the project.
While services were initially aware of other organisations, the level of communication between these had increased at the conclusion of the project. Before the QIC, participants reported that they spoke regularly with people from an (external) organisation on 95 occasions and this increased to 139 occasions at the conclusion of the QIC.
Participants reported that building relationships was one of the most helpful aspects of participating in the collaborative. Sometimes this involved developing relationships within their own organisations:
…there were people within our health network that were involved that I hadn’t previously had anything to do with (Participant2).
More commonly, participants spoke of the benefit of being connected to external services that were involved within the network.
…it was hugely beneficial because it gave me access to leaders within SA Ambulance (Participant1).
Working in collaboration with external providers offered new perspectives:
I think everybody sees situations based through their own lens, and that’s heavily influenced by what your discipline is, so I think nursing sees patients in a different way to medicine, in a different way to the ambos. So, this was a really good opportunity to see what we had in common … and then start to bridge those gaps (Participant1).
Participants found that they shared a lot of the same problems:
…it was also really good to see people from other health networks and see that they have exactly the same types of presentations, and exactly the same challenges that we have here (Participant1).
The role of the network manager was key in building relationships. The network manager initiated regular contact with project teams—usually weekly to fortnightly. With a background working in multiple roles in the state health service the manager was well positioned to link the teams with other relevant people, services and initiatives.
She’d give us contacts around—we were seeking information around palliative care documentation and the language to use, and she gave us a few contacts from that, from palliative care in town, and from Central—Central Health Network. So, we sort of had lots of people who I’d never heard of before, but you know, through email I came to know them really well (Participant6).
The teams described the network manager as being responsive, supportive, guiding them through the quality improvement process and ensuring teams did not get stuck in the detail and remained focused on the bigger picture. The regular meetings and actions ensured that teams continued to take action. The network manager reported that developing the relationship was critical:
I think the biggest thing is building the relationships and the trust with the clinicians. So, if I said I was going to go something, making sure that I delivered on that and in a timely way and respecting that they are all busy clinicians (Participant3).
Did the STAAR-SA QIC build capacity in the workforce to undertake quality improvement projects?
Survey results showed that most (77%) respondents agreed that their ability to do quality improvement activities had improved. Almost two-thirds (64%) reported that they used the skills developed through participation in the QIC in other projects.
Although team members were involved in the network because they had some leadership responsibilities in their organisations, few had taken part in quality improvement activities or at this level:
I have done quality improvements at a ward level but … not overarching such a large footprint or working with other health networks, I haven’t done that (Participant1).
…it’s actually really nice to be involved in something that was a bit of a more formal QI and a more formal project. And because it is good to sometimes step through and apply a bit of a structure to it and a model to it (Participant9).
They spoke of the opportunity to be involved in a state-wide project:
…it was very beneficial for me to see how a project at this level works and to be able to have, work with people who are highly esteemed or work at a very high level, and to be able to be in a collegial manner with them was hugely beneficial for me (Participant1).
Clinicians sometimes reported that being involved required a multitude of skills such as considering how to measure change, conducting online education and public speaking. Above all, they found the structure of the process, the tools and the support of the network manager helped them to develop their skills in quality improvement. The network manager reported a key benefit of the project was the encouragement to try something new:
…it gave people the ability to try things that they perhaps wouldn’t have tried otherwise, and we often use the phrase don’t be afraid to fail and think outside the box” (Participant3).
Did the QIC improve the quality of care for older South Australians at the time of transition?
One in five (21%) survey respondents indicated that they achieved the stated aims of their project better than expected and a further 41% of respondents felt they achieved their aim as expected. Some (26%) got close to their aim but achieved less than expected and some (12%) didn’t know. In terms of degree of improvement, outcomes on selected measures improved significantly (25% respondents), improved slightly (47% respondents), reported no measurable change (16%) or did not know (13%). All respondents indicated a degree of success in implementing quality improvements; 55% reported ‘very successful’ and 45% reported ‘partly successful’ implementation. The network manager linked likelihood of success with having support from leaders within the organisation:
…those that had good connections with their leadership teams and the trust of their leadership teams to make decisions (Participant3).
While we were unable to capture pre-post outcome data for all teams, all project leads could describe positive outcomes for clients arising from the work:
There were two patients that we knew that had been—that we had, our doctor had been to our education session, and they were discharged to residential care. So, we looked them up to see what happened, and the 7-step pathway and the discharge summary were fantastic, they were really good (Participant6).
Importantly, most of the teams described that they would continue to either maintain service improvements or continue to initiate further improvements:
I can only see us going from strength to strength, it’s actually really quite good (Participant5).
Despite efforts within the QIC to connect services, participants reported that there were limits as to what could be achieved in terms of seamless care transitions, often due to restrictions in other services’ capacities. They particularly mentioned the challenges in aligning care with general practices or residential aged care home facilities as these organisations typically have many sites, a different staff profile (with few senior clinicians) and operate via different funding mechanisms, meaning that communication with these stakeholders was hard.
Two case studies are presented below which describe what and how the team improved the service and the subsequent outcomes for older South Australians (box 1).
Case studies
Virtual support for patients in residential aged care homes
Problem: Residents presenting to hospital when care would be more appropriately provided within the residential aged care home. The ambulance service attending 40–50 calls per day from residential care homes with the majority of patients (85%) transferred to hospital.
Collaborative group: consultant geriatricians, nurse consultants, operations manager and team leader ambulance service.
Strategies to address: Identify a single point of contact who can provide advice remotely, develop pathways for alternatives to hospital presentation, extended hours of operation.
Outcomes: Most residents referred to the ambulance are now remaining at the residential aged care home rather than being transferred to hospital (Across the three health networks, 66%, 62% and 71% of patients are now remaining at the residential aged care home).
Country health in-home monitoring
Problem: High number of chronic-disease related hospital admissions for people currently receiving home care packages in the Riverland, South Australia. Contributors included no discharge notification to the community home care package team upon hospital discharge, long waiting periods for doctor appointments, limited health literacy amongst patients and lack of general practitioner (GP) involvement in care planning and patient goals.
Collaborative group: Service director, team leader, nurse, home care package case manager, manager of service reform.
Strategies to address: Virtual clinical care home remote ambulatory monitoring for home care package clients at risk of hospital admission, education of case managers and support workers on telehealth and chronic disease self-management, introduction of AWACCS Tool to monitor and document changes in health status.
Outcomes: New referral process, increased knowledge in support workers about health and monitoring of changes, resources supplied to allow monitoring of patient’s condition in their own home, improved knowledge about patient health for GPs and specialists. Changes in admission rates to hospital are unknown.
Discussion
In the absence of clear evidence for interventions that can prevent or reduce hospitalisations in older people, it is important to focus on strategies which are most likely to be successful given the context and nature of existing problems. As part of a larger programme of work we formed a QIC involving nine teams across different services. Each team had its own aims, strategies and evaluation plan. Our evaluation suggested that the STAAR-SA QIC was effective in terms of improving networks between services and building capacity in clinicians to conduct quality improvement initiatives. Unfortunately, we were not able to use rigorous methods (such as an interrupted time series analysis) to understand the effects of the collaborative on outcomes for older people. A single process measure that could be used by all teams was also lacking. Our participants did however report positive outcomes of their work in the surveys and in the case studies.
A strength of QICs is that they support implementation of evidence in different contexts. Another strength is involving health professionals who work on the front line in the work. The local team considers the best way to overcome local barriers and how to best adapt the evidence. The ‘ground up’ approach was novel, and the result is improved ownership of the work and local solutions most likely to be acceptable to their population. Our data also showed that we built capacity among QIC members to lead future quality improvement initiatives. Collection of rigorous data arising from QICs works well in structured settings (eg, hospitals) in groups focused on the same hard outcome (eg, number of tests ordered or drugs prescribed) where this data is routinely collected and easy to obtain (eg, administrative data within a hospital). We invited health professionals to join the STAAR-SA QIC from different settings (community, hospital) and to address different outcomes (eg, medication review, patient satisfaction, transfer to hospital following ambulance call). This meant that collection of data was difficult and unable to be pooled across groups. Interestingly, involving health professionals from different contexts proved to be a strength. Participants were able to appreciate problems from other perspectives, build relationships across services and gain access to leaders from external sites. With limited time and resources, we chose to invest in building engagement within the STAAR-SA network and with the QIC teams. The trade-off was that we did not have the resources to provide financial support for the teams to assist with rigorous data collection. This tension is likely to be common among all QICs working with healthcare teams in real-world settings.
The Royal Commission into Aged Care Quality and Safety in Australia largely overlooked the issue of hospital-home transition. However, the Commissioners repeatedly identified how fragmented care resulted in worse outcomes and a key recommendation included in the final report was that the government ‘coordinate the development of an integrated system for the long-term support and care of older people providing for their needs for welfare support, community services directed at enhancing social participation, affordable and appropriate housing, high-quality healthcare and aged care’.17 Achieving integrated care across health and aged care settings requires whole system redesign which is rarely achievable. This project took steps towards integration by examining how services can better work together to improve outcomes for older people at the interface of acute-community and health-aged care services.
QICs range in terms of their methods and approaches. The roles of the personnel involved are rarely described in detail. In this QIC, the role of the etwork manager was the key to supporting teams to make progress. The manager’s previous employment in different roles in the health service was useful in assisting the teams to build relationships. The network manager’s office was situated within the central SA Health team which also increased their knowledge of current initiatives across the state. The expertise, responsiveness and facilitation skills used by the network manager likely contributed to the lack of withdrawals and the high levels of satisfaction reported by teams. We are seeking to sustain the partnerships and work conducted to date by applying for funding to employ a network manager to work across sectors.
The key limitation of this evaluation is that we were unable to rigorously evaluate whether the quality improvement resulted in reduced preventable admissions or rehospitalisations among older people. Ideally, we would have used an interrupted time series analysis to examine effects on a single key outcome however we had limited resources to invest in the evaluation. A further limitation is that the teams did not collect or present high-quality pre–post data. We encouraged teams to measure their own improvement over time and there were limitations in what data were collected and the methods of data collection. Another limitation of the work is that teams tended to address quality by focusing on improving communication and team processes. This is understandable given that these factors can be influenced and controlled by the team. However, literature shows that older people report the hospital discharge process leaves them feeling powerless and insignificant; more work could have been done to improve quality by empowering consumers.
The findings of this study suggest that QICs involving health professionals across sectors can assist in improving the integration of care. The findings also show that different sites have different priorities but supporting the sites through the process of quality improvement can result in positive outcomes and helps to build capacity in clinicians. Finally, deliberate and action-focussed activities (such as establishing a QIC) to connect people across silos helps to build a network for ongoing collaboration.
Data availability statement
Data are available on reasonable request. Excerpts of deidentified data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The evaluation of this study had ethics approvals from SA Department for Health and Wellbeing Human Research Ethics Committee (Ref: 2021/HRE00124). The study also has Site Specific Approvals for the following sites: Central Adelaide Local Health Network (2021/SSA00221), Northern Adelaide Local Health Network (2021/SSA00218), Southern Adelaide Local Health Network (2021/SSA00217), Riverland, Mallee Coorong LHN (2021/SSA00219) and SA Ambulance (2021/SSA00220). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to acknowledge the STAAR-SA Study Collaborators Professor Maria C Inacio, Dr. Robert N Jorissen, Dr. Clarabelle T Pham, Professor Jonathan Karnon, Dr. Alice Bourke, Mr. John Forward, Dr. John Maddison, and Professor Craig Whitehead for supporting this study. We also acknowledge South Australian Government Heath (SA Health), the research team of Registry of Senior Australians’ (ROSA) and the Australian Institute of Health and Welfare (AIHW) for ensuring the success of this study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Collaborators Individual authors: Associate Professor KL, EL, JAR, CM, MC, GH. STAAR-SA Study Collaborators: Professor Maria C Inacio, Dr. Robert N Jorissen, Dr. Clarabelle T Pham, Professor Jonathan Karnon, Dr. Alice Bourke, Mr. John Forward, Dr. John Maddison, and Professor Craig Whitehead.
Contributors MC, KL, EL and GH conceived the study. KL and JR reviewed the transcripts. KL drafted the article, and EL, JR, MC, CM and GH on behalf of STAAR-SA Study Collaborators edited the draft. All authors reviewed and approved the final article. KL is responsible for the overall content as the guarantor. KL accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding This study was a part of STAAR-SA programme which was funded externally through a Medical Research Future Fund Rapid Applied Research Translation grant, administered by Health Translation SA. It was peer reviewed as part of the application/award process.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.