Article Text

Abstract
Background On 3 August 2020, Public Health Scotland commenced a prospective surveillance study to monitor the prevalence of COVID-19 among asymptomatic outpatients attending dental clinics across 14 health boards in Scotland.
Objectives The primary aim of this quality improvement project was to increase the number of COVID-19 tests carried out in one of the participating sites, Glasgow Dental Hospital and School. The secondary aim was to identify barriers to patient participation and staff engagement when implementing a public health initiative in an outpatient setting.
Method A quality improvement working group met weekly to discuss hospital findings, identify drivers and change ideas. Details on reasons for patient non-participation were recorded and questionnaires on project barriers were distributed to staff. In response to findings, rapid interventions were implemented to fast-track increases in the numbers of tests being carried out.
Results Over 16 weeks, 972 tests were carried out by Glasgow Dental Hospital and School Secondary Care Services. The number of tests per week increased from 19 (week 1) to 129 (week 16). This compares to a similar ‘control’ site, where the number of tests carried out remained unchanged; 38 (week 1) to 36 (week 16). The most frequent reason given for non-participation was fear that the swab would hurt. For staff, lack of time and forgetting to ask patients were identified as the most significant barriers.
Conclusion Public health surveillance programmes can be integrated rapidly into outpatient settings. This project has shown that a quality improvement approach can be successful in integrating such programmes. The key interventions used were staff engagement initiatives and front-line data collection. Implementation barriers were also identified using staff questionnaires.
- Quality improvement
- COVID-19
- Surveys
- Healthcare quality improvement
Data availability statement
Data are available on reasonable request. Raw data can be made available on request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Since the outbreak of the coronavirus COVID-19 (SARS-CoV-2) pandemic, there has been increasing awareness of the significant role asymptomatic carriers play in the spread of the disease. Systematic reviews and meta-analysis of over 40 000 cases from over 100 studies estimated that 13%–17% of positive cases were asymptomatic.1 2
On 3 August 2020, Public Health Scotland, on behalf of the Scottish Government, commenced a prospective surveillance study to monitor the prevalence of COVID-19 among asymptomatic outpatients attending dental clinics across 14 health boards in Scotland.3 The aim of the project was to investigate SARS-CoV-2 infection in asymptomatic-screened dental patients to inform community surveillance and improve understanding of risks in the dental setting.4 This was a public health project aiming to gain a better understanding to help with control of COVID-19. Ethical approval was waived by the West of Scotland Ethics Service. Patient participation was voluntary, and consent was obtained verbally. All patients were eligible provided they were over 5 years of age and asymptomatic for COVID-19. For the period of the quality improvement project (QIP), participants could only be tested in the enhanced surveillance study once. Of the 6115 asymptomatic patients who were tested in Scotland during the first 16 weeks, 34 tested positive.5
Over the first 5 weeks of the programme, on average, 27 swabs were collected each week at Glasgow Dental Hospital and School. The National Programme set targets for each Health Board based on national population distribution. Increased participation was required to meet these targets.
The primary aim of this QIP was to increase the number of COVID-19 surveillance tests carried out in outpatient clinics at Glasgow Dental Hospital and School.
Background
On review of the literature, there were few reports of methods or interventions to improve engagement and participation in public health-related surveillance programmes in an outpatient clinic setting. A feasibility study on oral human papilloma virus (HPV) surveillance in dental settings found that a research nurse recruitment model was more effective than dental care teams.6 Research nurse support was not available in dental outpatient settings and therefore this public health programme would rely on dental care teams. At Glasgow Dental Hospital, a research dental nurse was available for limited sessions to support training and coordinate the programme across several geographically distinct outpatient units.
Measurement
Baseline data on the number of tests carried out in Glasgow Dental Hospital between weeks 1 and 5 were obtained from a central participation log.
To compare the effect of the QIP, the number of tests completed over the 16 weeks was also obtained from the central participation log of another pilot site involved in the surveillance programme (the Control Centre). This acted as the control as it received the same information and support from Public Health Scotland but did not implement a quality improvement methodology as Glasgow Dental Hospital (the QIP Centre).
In week 7, electronic data collection spreadsheets were developed and added to each department’s shared drive. Junior clinicians were asked to collect and input data during their timetabled COVID-19 surveillance duties. Data were collected in several dental hospital departments: Restorative Dentistry, Oral Surgery, Oral Medicine, Paediatric Dentistry and Orthodontics. The following data were recorded from week 7 to week 16:
Number of patients participating in the surveillance programme (outcome measure)
Number of patients attending the dental hospital (process measure)
Reasons for non-participation
Number of patients ineligible to participate
Number of patients treating clinicians deemed inappropriate to participate
Number of patients refusing to participate
When patients refused to participate, they were asked if their demographics could be recorded (gender, age group) and primary motivator for refusal from a predetermined list:
I do not have enough time for the test to be done.
I am concerned the swab will hurt.
I am concerned a positive test will have an impact on work.
I am concerned I am COVID-19 positive and do not want to know.
I do not want to be part of a public health programme.
I do not want to say.
Other (optional to specify reason).
Incidences where attending patients did not participate but a reason was not recorded were labelled ‘missed events’. These represented instances in which either the patient was not asked or the reason for refusal given was not recorded or communicated.
Design
A QIP working group was established at the beginning of week 6. Approval from the hospital’s clinical governance committee was granted in September 2020. Within the hospital, different departments have varied clinical environments and patient demographics. Therefore, departmental leads were assigned within the working group. A plan, do, study, act (PDSA) improvement model was adopted. Weekly meetings were held to discuss hospital and departmental findings, identify drivers and change ideas (driver diagram can be viewed in online supplemental figure 1). Due to the ongoing COVID-19 pandemic, and necessity for rapid data collection, interventions were implemented on a weekly basis to increase the number of tests being completed.
Supplemental material
Strategy
The first PDSA cycle (week 6) was the involvement and training of junior clinicians, and this was adapted the following week (week 7) by asking the junior clinicians to collect and record data. The hope was that this would influence the number of swabs being carried out by junior clinicians by encouraging accountability.
Email updates and reminders were implemented from week 7 and this was modified after studying the intervention by introducing the addition of a hospital ‘league table’ showing the numbers of swabs carried out by each department. The hope was that this would initiate some competition between departments, thus increasing the number of swabs carried out.
To aid with change decisions and to gain an insight into the perceived barriers to the surveillance programme, three questionnaires were developed and distributed to the three staff groups of junior clinicians (week 8), senior clinicians (week 12) and dental nurses. Senior clinician refers to consultant and any non-training grade dentist providing patient care in the dental hospital. Junior clinician refers to dental core trainees. These questionnaires were intended to provide a dual purpose in that they served as a reminder and a means to influence behaviour.
The questionnaires were created using Microsoft Forms, and the link was distributed via email. The participants were asked a number of yes/no questions and also asked to rank a listed set of barriers to carrying out surveillance. The lists, specific to each staff group, consisted of 10 barriers and were predetermined by the QIP working group. All responses were submitted anonymously.
Email reminders appeared to improve numbers but, in an effort to make the reminders more personable, a PDSA cycle in week 9 involved including a reminder about the project at individual department preclinic huddles. The preclinic huddles appeared to lead to an improvement and in light of this, similar reminders were issued at the dental nurse manager morning meetings (week 11).
Forgetting to ask patients to be involved was one of the chief barriers drawn out of the questionnaires. In response to this, reminder posters were created to prompt clinicians to ask their patients. These were displayed in clinical rooms in view of both the patient and clinician (week 11).
Involvement of junior clinicians was successful and therefore this was expanded to include training of dental nurses (week 11) and dental undergraduates (week 14).
Results
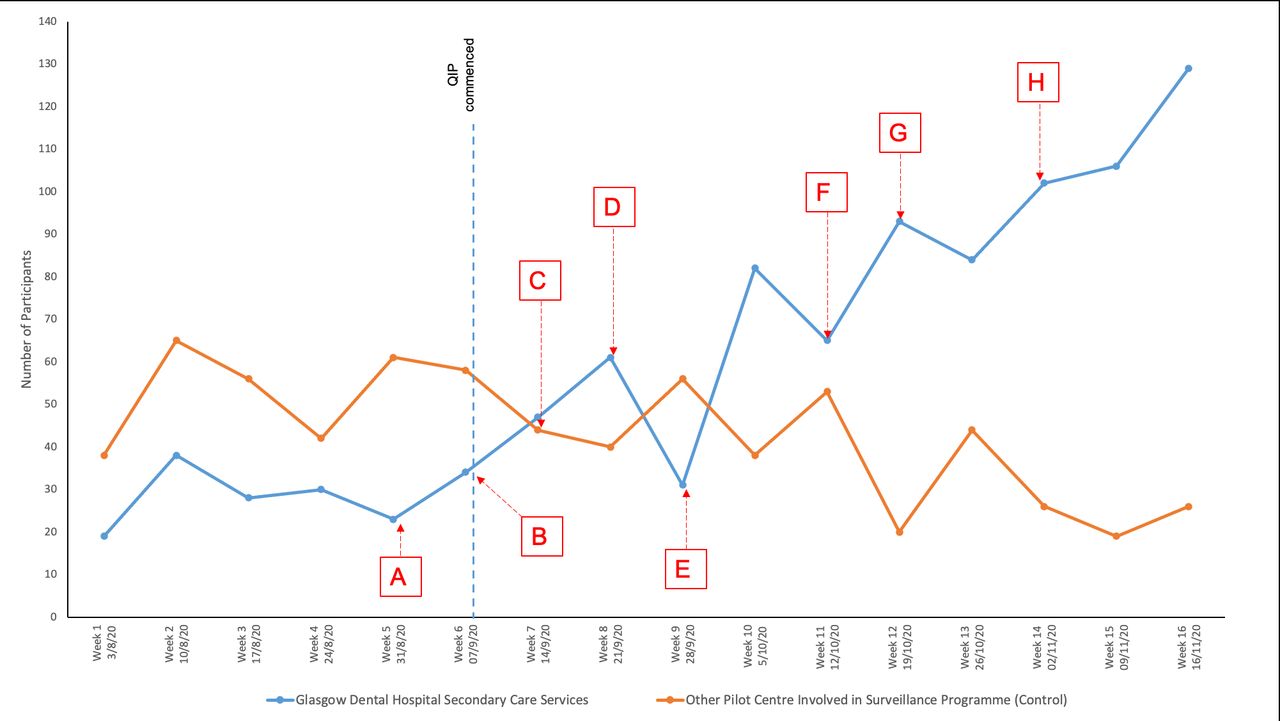
Over the 16-week period, 972 tests were carried out in Glasgow Dental Hospital Secondary Care Services (QIP Centre). The number of tests per week increased from 19 to 129 (figure 1). The other Pilot Site, which acted as the control (Control Centre), completed 686 tests and the number of tests per week decreased from 38 to 26.

Number of surveillance programme participants over time compared with control ‘pilot centre’ and chronology of interventions. Blue line shows increasing trend in numbers of participants following commencement of the quality improvement project (QIP). Orange line shows numbers of participants taking part in a control pilot centre also involved with the surveillance programme. Interventions: (A) Commenced training of junior clinicians. (B) Junior clinicians commenced clinics and department data collection spreadsheet implemented. (C) Presentation at local clinical governance meeting and commencement of weekly department update emails. (D) Junior clinicians questionnaire circulated. (E) Inclusion in preclinic huddle. (F) Commenced dental nurse training, reminder posters distributed in clinical and patient waiting areas, inclusion in dental nurse managers huddle. (G) Senior clinician questionnaire circulated. (H) Undergraduate training.
The mean baseline of the number of tests carried out in the QIP Centre, before the QIP started, between weeks 1 and 5 was 27.6 (SD=6.5). The mean baseline in the control centre was 52.4 tests (SD=10.6). The mean number of tests carried out during weeks 12–16 in the QIP Centre and the Control Centre was 102.8 and 27 tests, respectively.
The number of patients who attended the QIP Centre from week 7 to week 16 was 2725. It is important to note that these data is an approximate obtained from the sum of individual department records who participated in the QIP. Footfall was estimated to increase from 152 patients attending in week 7 to 431 in week 16. Footfall data from the Control Centre is not available but footfall across all dental sites increased in response to remobilisation of dental services.7
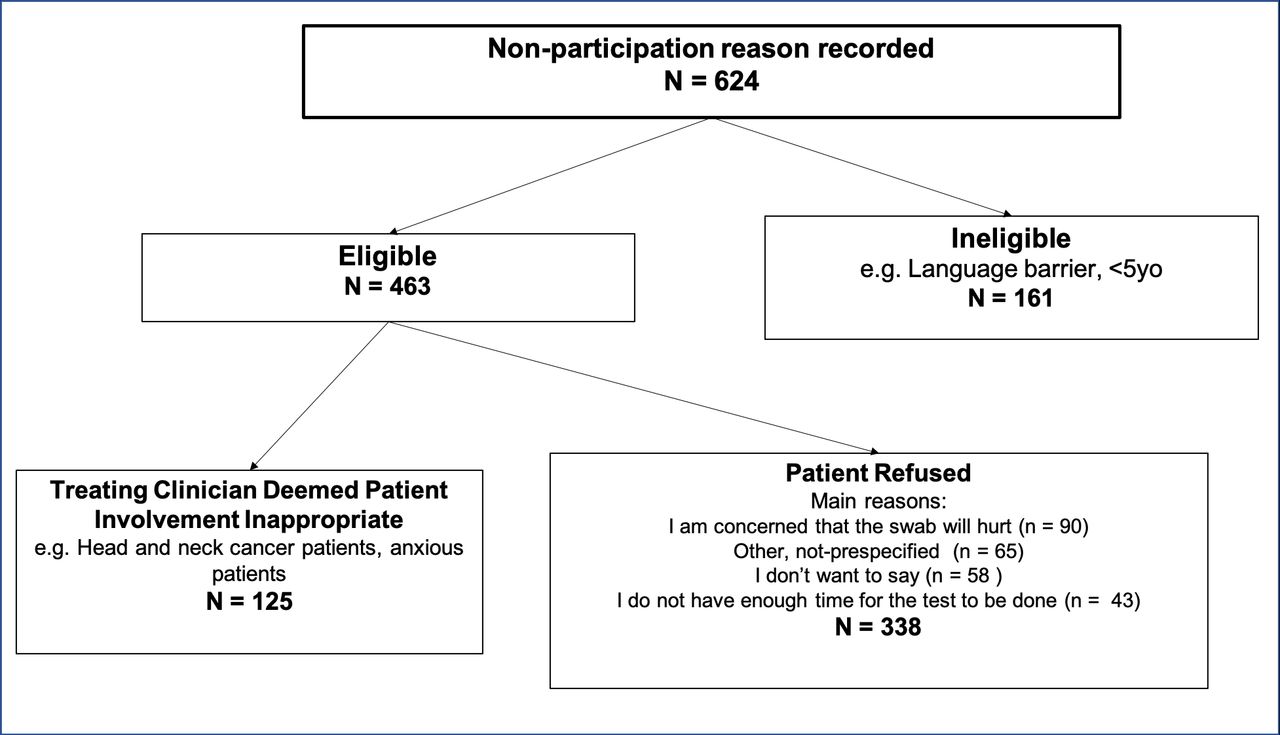
The reasons for non-participation at the QIP Centre were recorded (figure 2). Non-participation was defined as a patient attending but not taking part in the Surveillance Programme. This included eligible and ineligible patients. Due to varying clinical demands and staff participation, not all departments were able to collect data on reasons for non-participation. Cases for which no data were recorded were defined as ‘missed events.’
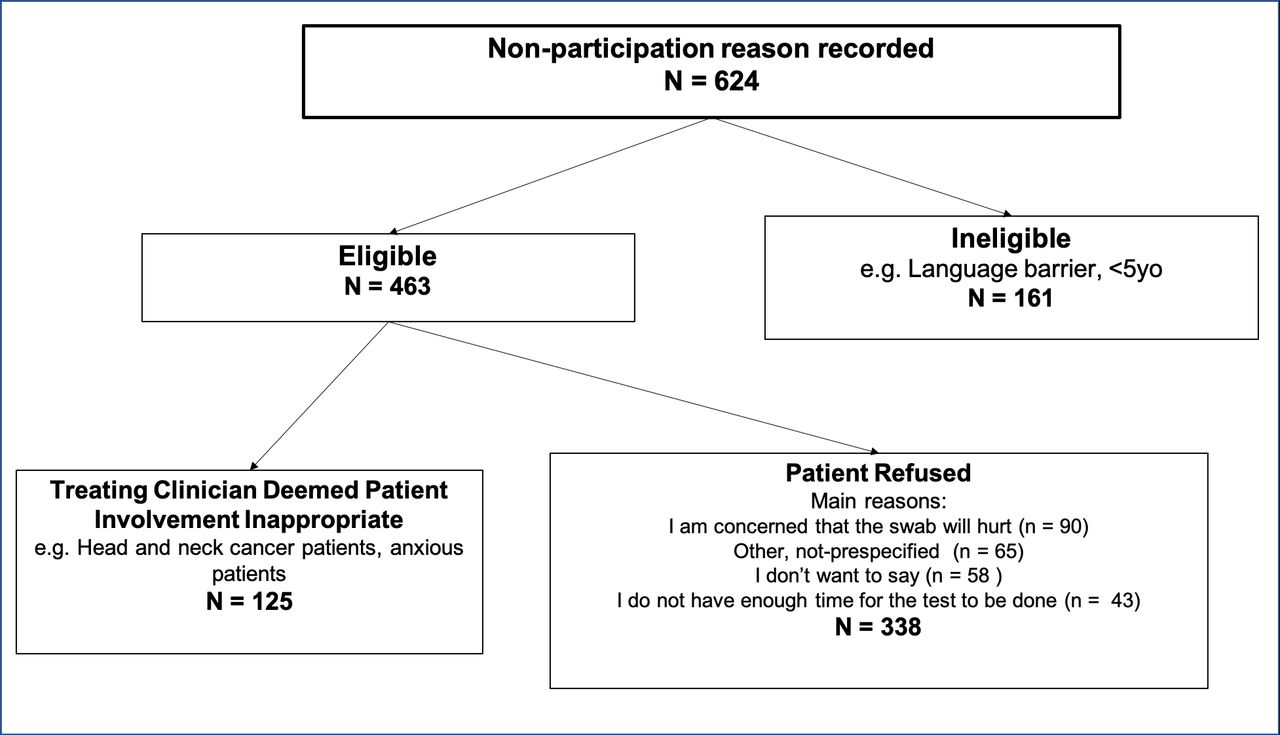
Reasons for non-participation. The majority of non-participation was due to patient refusals, with the “other” category being the most selected option. It is important to note that there were also a number of missed events which included patients not being asked or the reason was not recorded. Other reasons for patient refusal can be found in online supplemental figure 2.
Supplemental material
One hundred and sixty-one patients were recorded as ineligible to participate in the study. The most common reasons for exclusion were that they had already anticipated in the surveillance project at a previous appointment or there was a language barrier. Patient information was subsequently made available in a number of different languages and Public Health Scotland commissioned a Health Inequalities Impact Assessment of the entire programme that included reviewing how to make the programme more accessible to people whose language is not English.8
Details of patient refusal were recorded for 338 patients (online supplemental figure 2). Of these, 190 were females, 117 were males and gender was not recorded for 31 patients. One hundred and twenty-five were in the 19–44 age group, with the remainder spread evenly across other age groups. Of the seven predetermined patient refusal reasons, the most common reason selected was ‘I am concerned that the swab will hurt’ (26.6%, 90/338). Nineteen per cent (65/338) of these were recorded as ‘other’. This accounts for various other reasons that were not considered as possible patient barriers at the time of project design.
Treating clinicians decided that 125 patients were inappropriate for participation and did not invite them to participate. Prioritising patient care was at the centre of the surveillance protocol, and in these cases the treating clinician deemed that requesting patient participation in the surveillance programme could potentially compromise their clinical care. Examples of this would include extremely anxious patients, or head and neck oncology patients with extremely complex local anatomy. Twenty per cent of these patients had a current or previous diagnosis of head and neck cancer and were attending for pretreatment assessment or oral rehabilitation post-treatment.
In addition to patient barriers to participation, we sought to identify barriers to staff participation.
Responses to the distributed questionnaires were received from 52% (n=28) of senior clinicians, 100% (n=17) of junior clinicians and 24% (n=17) of dental nurses.
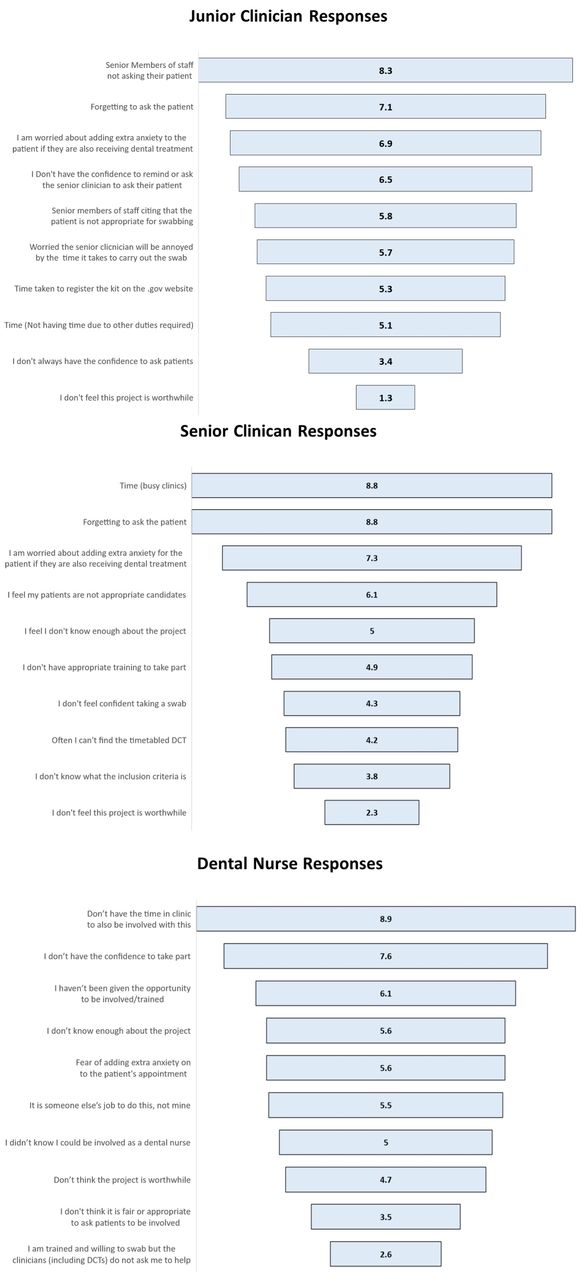
In the final question, staff were asked to rank a list of predetermined barriers from 1 to 10. Responses were assigned a corresponding value based on the inverse of their rank from 1 to 10 (eg, rank 1=value 10, rank 2=value 9) and the mean value across all respondents for each item calculated to represent their significance to each staff group (the higher value, the greater the significance) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Responses to the staff questionnaires showing perceived barriers to participating in the project. Junior clinicians: ‘Senior members of staff not asking their own patients’ had the highest mean rank. Senior clinicians: ‘Time (busy clinics)’ and ‘forgetting to ask the patient’ had the highest mean rank. Nursing staff: ‘I don't have enough time to be involved with this project’ had the highest mean rank. DCT, Dental Core Trainee.
The junior clinicians had timetabled sessions for supporting the surveillance programme, but 29% had other clinical duties to carry out at the same time. This, in all cases, was face-to-face dental patient care. The greatest perceived barrier to junior clinicians asking patients to take part was ‘Senior members of staff not asking their patients’ which had the highest mean value (8.4/10) followed by ‘forgetting to ask the patient’ (7.1/10) and ‘worrying about adding extra anxiety to the patient’ (6.9/10).
The senior clinician questionnaire identified that 89% of respondents had invited a patient to be involved with the project. All respondents, with the exception of one, were aware of the project and 82% felt they knew enough about the project. When asked if they would want training on how to carry out a swab themselves, 64% responded no. ‘Forgetting to ask the patient’ and ‘time (busy clinics)’ shared the highest mean value for perceived barriers (8.8/10).
Of nursing staff who participated in the questionnaire, all were happy to be involved in inviting patients to participate and 71% were happy to carry out a COVID-19 swab. ‘Not having enough time’ in the clinic had the highest mean value of the barriers (8.9/10), followed by ‘lack of confidence’ (7.6/10).
Lessons and limitations
This QIP successfully contributed to establishing and maintaining patient involvement and staff engagement in a rapidly mobilised asymptomatic outpatient COVID-19 surveillance programme. The programme identified that training and engagement of staff at all levels is critical. Measures taken that appeared to be effective were updates at department ‘morning briefs’ or ‘huddles’, and reminder emails containing a department ‘league table’ presenting the percentage of patients swabbed per week in each department. It is appreciated that the number of swabs carried out increased as patient footfall in the hospital increased, nonetheless, had the project not been implemented the authors suggest it is highly unlikely that the number of swabs may have increased with footfall (indeed the changing clinical service would potentially have further compromised the surveillance programme as implied by the data from the control site).
The staff barrier questionnaires provided useful information, as well as serving as a reminder and means to influence behaviour. The biggest barriers perceived by senior clinicians were lack of time, due to busy clinics, and forgetting to ask the patients. This finding ties in with the junior clinicians’ chief complaint of senior clinicians forgetting to ask their patients. The dental nurses felt they were often too busy with normal clinical duties to also be involved in swabbing patients or that they did not have the confidence to participate. Subsequently training was provided to all members of staff wishing to participate, with a focus on specific sessions for dental nurses to improve knowledge and confidence levels. Thus, these findings demonstrate that senior clinician leadership and engagement is key. While sample collection by senior clinicians is likely inappropriate, clearly the senior clinician is a role model to the rest of the team and can influence their attitudes and behaviours.
It should also be noted that the numbers of swabs carried out per week was influenced by many confounding factors and not just the interventions made. Changes in government policy and local procedures relating to the pandemic were likely to have influenced the number of participants during this project, alongside factors such as public holidays during which the outpatient clinics were not operating. From the data collected, this is most notable for week 9 in which the number of participants fell from 61 to 31 (49.2%). Part of this decline can almost certainly be attributed to a public holiday reducing the number of days of surveillance.
During weeks 7–16 of this study, of the eligible patients for whom data were recorded, approximately 25.6% of patients refused to take part in the surveillance study (n=338). In other surveillance studies, a wide range for refusal percentages have been published, from 2.5% up to 90%. In a study investigating influenza-related hospitalisations at 12 sites in countries in the Northern Hemisphere, 2.5% of participants had declined to provide swabs.9 A surveillance study for acute respiratory infections conducted in Germany saw 2.9% of participants withdraw and 48.1% of those eligible refused to participate.10 In the ‘Flu Watch’ study, approximately 10% of households responded to written invitations to be part of the study.11 A pandemic influenza epidemiology study conducted in Vietnam from 2007 to 2010 reported a participation refusal rate of approximately 10%, but no records were kept on the numbers and reasons for non-participation.12 THE HOPSCOTCH study required participating patients to provide oral rinses to test for HPV. The main reason for patient non-participation was patient refusal at 31.6% with dentist refusal very low at 0.9%.6
There were many ‘missed events’ describing patients who attended the hospital but the reason why they did not participate in the surveillance programme was not known and/or the treating clinician did not ask their patient. Anecdotally, ‘missed events’ were usually a result of clinicians forgetting to ask their patients. Sometimes, the staff member tasked to carry out the testing was not available due to sickness or last-minute changes in the rota. The hope, in these situations, was that the treating member of staff would carry out the test themselves. This very rarely happened. This highlights the importance of having a staff member designated or rotated to carry out surveillance. An Australian study assessed the knowledge and attitudes of general practice staff towards pandemic influenza and found only 36% completed the survey provided.13 A Swiss study asked primary healthcare workers to record symptoms of influenza-like illness in a weekly online survey distributed via email and self-collect a nasopharyngeal swab if any symptoms were recorded. Just over half (53.7%) of the staff provided data for the study.14 In Scotland, healthcare staff uptake of rapid lateral flow self-testing has been reported at one time point to be as low as 27.7%.
There was particular difficulty in implementing the project within the paediatric dentistry and orthodontic departments. Junior clinicians, unlike in other departments, were timetabled to be carrying out both regular patient care duties and COVID-19 surveillance. As a result, there was a greater reliance on senior clinicians and dental nurses to engage patients. An additional difficulty, specifically relating to the paediatric dentistry department that became apparent, was the large number of patients deemed inappropriate for involvement. As a specialist unit, many of the children attending have complex medical histories, including autism. In addition, many of the patients are highly anxious or have sustained traumatic dental injuries. As a result, patient care was prioritised for these patients and testing was not offered.
One of the limitations of this project was that balancing measures were not considered or recorded. Balancing measures could have informed if the surveillance study was having effects on normal clinical activity. For example, due to the surveillance study, did more clinics run late? Another balancing measure which was not explored was the effect on patients’ anxiety. Attending the dentist is already an anxious experience for many patients. Introducing another procedure into the appointment may have increased patient anxiety levels and thus their anxiety level during subsequent consultation or treatment.
We were responding to Scottish Government request to rapidly increase testing. Therefore, the baseline data collection was limited, and ideally a baseline of 12–14 weeks of data would be preferable. Similarly, in response to this desire to increase the numbers of swabs being carried out rapidly, there was a decision to simultaneously implement multiple interventions in some weeks, rather than adopting the conventional approach to studying each intervention individually. This made it more difficult to assess the effectiveness of individual interventions. This surveillance project concluded shortly after the time frame studied in this report and therefore it was not possible to assess the sustainability of the interventions. Due to the success of the wider surveillance project, it is possible that dental and other outpatient teams could be involved again in the surveillance of transmissible diseases. Future projects could hopefully use our findings as a baseline and measure the sustainability of these and any further interventions. Senior clinical staff were informed about the project at an early stage. However, information as of itself did not translate into engagement. The improvement team in this project could be described as a peripheral subject group consisting of clinical and academic staff in contrast to a central subject group which would include senior organisational managers. We used concepts of institutional entrepreneurship such as seeking the support of hospital management which helped to raise the awareness of the project, create a power base and allowed the team to use resources.15 The improvement team also used their position as colleagues of senior clinicians to network and build relationships in an attempt to increase their acceptance of the surveillance project. Despite this, senior clinician engagement was found to be a significant barrier to increasing numbers of tests carried out. There were considerable competing demands on senior clinical staff, and future work should investigate how to improve senior staff engagement in the process. In terms of the external validity of this report, it is important to emphasise that this QIP was carried out within secondary care. Further studies would be required to evaluate the success and barriers of integrating this into a primary care setting.
Conclusions
To the best of the authors’ knowledge this is the first example of a QIP in relation to improving participation and engagement in a public health surveillance programme in an outpatient setting. It is likely that there will be an ongoing need for dental—and other outpatient—teams to be involved in public health initiatives—either to address population level issues such as the COVID-19 pandemic or to engage in supporting patients’ general health. This project has shown that it is possible to integrate a surveillance programme into dental clinics, in a secondary care outpatient setting. The pressures of time in a busy clinical environment and forgetting to ask or invite patients emerged as notable barriers.
This project has also demonstrated that a quality improvement approach can be successful in integrating such programmes into a dental setting. The key interventions used were staff engagement initiatives and front-line data collection. Investigating barriers at the ‘coal face’ using questionnaires and training all members of the clinical team can be successful in helping to integrate a surveillance programme into a healthcare setting. It is recommended that further research or QIPs are carried out to investigate interventions which can improve engagement in surveillance programmes and also the barriers that need to be addressed.
Data availability statement
Data are available on reasonable request. Raw data can be made available on request.
Ethics statements
Patient consent for publication
Ethics approval
This was a QIP and was approved by NHS Greater Glasgow and Clyde Oral Health Directorate Clinical Governance Committee in September 2020. It did not need ethical approval.
Acknowledgments
The authors thank the following people for their invaluable help and support throughout the project: Dental Core Trainees, Dentists and Nurses at Glasgow Dental Hospital and School, Christine Goodall, Lisa Johnston, Fiona MacKenzie, Alan McIntyre, Shona Reid, Alastair Ross, Rosemary Watters, Jackie Wilson, Tricia Yuill and the Dental COVID-19 Surveillance National Team.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CW was the lead researcher for the project and guarantor. SH conducted data analysis and interpretation. CW, SH and JS were leads for individual departments and drove changes within respective departments. CB provided support and training sessions. SC supervised this project. PRC and SBMK collected and analysed non-participation data. CW and SH drafted the manuscript. SC, ME, JB, NM, RB, MG, SR, CC, CW and DIC were on the national team for the overarching surveillance project and provided feedback and comments regarding the content of this paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.