Article Text

Abstract
Only 30% of Ontarians are registered organ donors in spite of the vast unmet need for organ donations in Ontario, Canada. The purpose of this quality improvement (QI) initiative was to increase the number of registered organ donors in a primary care practice by providing an educational fact sheet and registration form to patients in the clinic's waiting room. Three Plan-Do-Study-Act (PDSA) cycles were conducted. In the first PDSA cycle, we created an information sheet to explain the need for organ donors and the registration process. Nine patients were surveyed regarding the clarity of the information sheet, which resulted in subsequent modification of the information sheet prior to the second PDSA cycle. For the second cycle, the revised information sheet was attached to a donor registration form and distributed to 30 patients in the primary care practice over a two-week period. 23 forms were returned, in which 4 patients were already registered organ donors and 5 patients completed registration forms. In the third PDSA cycle, a more compelling graphic was used on the pamphlet. Similarly, 30 forms were distributed; 23 forms were returned, with 6 newly completed registration forms. Overall, the project increased the donor registration rate from 10.0% to 28.3%. The process allowed patients to become more knowledgeable about organ donation need and aware of the Trillium Gift of Life website. We believe that providing patients with an information pamphlet and registration form in the clinic waiting room enhanced their awareness of organ donation and facilitated registration without delay. This QI initiative represents an effective and practical study to increase donor knowledge and provide opportunities for interested individuals to become registered organ donors.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Toronto, Ontario is the most populated city in Canada and home to some of the largest organ transplant programs in the country, yet Torontonians are lagging far behind other communities with respect to their participation in organ donation.1 As of June 30, 2016, only 21% of health card holders in Toronto were registered donors, placing Toronto at a rank of 164 amongst 170 cities in the province of Ontario and well below the provincial average of 30%.1 Meanwhile, top-ranking cities have donor registration rates exceeding 50%, highlighting substantial room for improvement in Toronto.1
Currently, registration for organ donation in Ontario occurs online or in-person through ServiceOntario (a governmental agency).2 There is no opportunity for recipients to interact with a specialized healthcare provider to ask questions about the donation process or clarify any misconceptions that they may have. This may result in several missed opportunities to recruit potential donors. In hospitals, it is often physicians working in the intensive care unit (ICU) that will discuss organ donation as a part of end-of-life care; however, many do not raise this topic with patients due to lack of time, training, commitment, or personal discomfort given the sensitivity of the topic.3 Therefore, we propose an alternative setting in which to raise awareness about organ donation. Prior studies have investigated the use of informational videos and kiosks in primary care clinics to promote organ donation and have found improvements in registration rates following these interventions.4 ,5 Given the prior success of promoting organ donation in the context of a primary care clinic, we are proposing an intervention that requires minimal resources and may be a more cost-effective means to promoting organ donation in the context of primary care. We will provide patients with a registration form and educational pamphlet in the waiting room of a primary care clinic. Patients will have the opportunity to learn the key facts about organ donation, return and fill their forms as they're waiting for their appointment, and raise any potential concerns with their family doctor during the visit.
We chose to implement our quality improvement (QI) initiative in a family doctor's office in Scarborough, Ontario, which is a subdivision of Toronto. It is a University of Toronto affiliated community-based teaching site that trains residents and medical students, and serves approximately 1000 patients. The purpose of this QI initiative was to increase the number of registered organ donors in the clinic by 10% in 3 months.
Background
In 2014, 2356 organ transplants were performed in Canada, yet over 4500 patients remained on the waiting list, and of those, 278 died awaiting surgery.6 These statistics become especially disconcerting when considering the success and life-saving potential of modern transplant procedures. Researchers at the University of Ottawa Heart Institute conducted a retrospective chart review and found a 90% survival rate in patients who had received heart transplants.7 Similar improvements have also been noted in other fields of transplant surgery owing to modern advances and innovations in medicine.8 ,9 Given the success of these procedures, transplant lists are steadily growing and while donation registration rates are also on the rise, the number of available organs and tissues remains insufficient to meet the demands of patients requiring surgery.9 Furthermore, the demand for organ transplantation is projected to continue rising in the face of an aging population with multiple morbidities.6 ,9 At this time, there is a critical need to emphasize promotion and education about organ donation amongst Canadians to increase registration rates.
Survey data has shown that 85% of Ontarians express support for organ/tissue donation, yet only 30% are actually signed up to be a donor.1 ,10 Clearly, there is a gap between the number of individuals who are interested in donation and those who actually register, thereby highlighting a need to facilitate the registration process in alternative ways. Cities worldwide have undertaken different initiatives to promote organ donation from online social media to challenge campaigns.11 ,12 This QI initiative investigates the effects on donor registration rates by providing organ donation educational material to patients waiting at a primary care clinic.
Baseline measurement
The family clinic did not have any pre-existing information on organ donation within their current medical charts as this was never requested or recorded by the doctor; therefore, we used two different sets of baseline data in this QI project. In each Plan-Do-Study-Act (PDSA) cycle, we asked patients whether or not they were currently registered as an organ donor. In doing so, each patient served as their own control and we were able to compare whether or not the intervention influenced non-donors' decision to register. This information was collected in the second and third PDSA cycles respectively, and is described in greater detail under the “Strategy” section. Baseline data was collected from a combined total of 60 patients over the course of PDSA cycles 2 and 3. In total, 6 out of 60 patients were registered donors, corresponding to a baseline registration rate of 10%.
We also used data provided by the Trillium Gift of Life Network – a government agency that coordinates organ and tissue donation and transplant in Ontario - as a baseline measurement of donor registration rates in the city of Toronto and Scarborough, Ontario. Of the 2,368,162 Torontonians covered under Ontario's Health Insurance Plan (OHIP), 473,009 were registered donors as of March 30, 2016 – a 20% registration rate across eligible donors.1 ,13 Scarborough – a subdivision of Toronto and the regional source of our participants - ranked even lower with a registration rate of 14%.13 Pre and post-intervention registration rates at the clinic were compared to the city-wide donor rates in order to evaluate the impact of our intervention and its potential to improve organ donation in other clinics across the Toronto area. Given that this project was conducted in a family medicine clinic that catered to a very particular demographic of patients (multi-ethnic and of lower-mid socioeconomic status), we were also interested in comparing the baseline registration rates at the clinic to the Scarborough average, since any significant differences across our participants could impact the external validity of the results. Our baseline registration rate of 10% did not vary substantially from the Scarborough-wide rate.
Design
The design and implementation of this project involved a multidisciplinary team of staff and students. The project champion was a family physician and associate professor at the University of Toronto's Department of Family and Community Medicine. The project champion was involved in the planning of the PDSA cycles and coordinated the implementation of the project. The QI initiative was executed in the project champion's family practice in Scarborough, Ontario and involved the office secretary, a clinical clerk, and medical residents working in the clinic. Our team consisted of four students who were involved with the University of Toronto's Chapter of the Institute for Healthcare Improvement (UT IHI) – one in a Master of Management of Innovation program, one in a Master of Health Informatics program, and two in a Doctor of Medicine program. The students worked closely with the project champion to identify changes that could be easily incorporated into the primary care clinic's workflow and design an intervention that would encourage more patients to register as organ donors. The students performed a literature search to identify the most common barriers to organ donation and interventions that have been previously implemented across different jurisdictions (e.g. Spain - the country with the highest rate of organ donation worldwide - employs an opt-out system where consent is assumed unless an individual specifically expresses a desire to not donate their organs or tissue).14 ,15 Our goal was to create a project that could be implemented on a much smaller scale in the setting of primary care with minimal resources. Findings from this literature search and further cause-effect analysis with the project champion led us to identify the following modifiable factors influencing organ donation: lack of knowledge about the need for organ donation and the registration process, and lack of urgency to register which could cause potential delays in the process (see Appendix 1 for the Fish-Bone Diagram showing the cause-effect analysis). These considerations guided the QI team to create an information pamphlet that could be disseminated to patients in the clinic waiting room alongside a physical copy of the registration form. We developed three Plan-Do-Study-Act (PDSA) cycles to test this intervention and achieve the following goals: increase patient awareness about organ donation, dispel myths, provide an immediate means of registering, and in turn, raise the rate of organ donor registrations at the primary care clinic.
Strategy
For the first PDSA cycle, we developed an educational pamphlet on organ donation to accompany the standard provincial registration form created by Trillium Gift of Life. The pamphlet provided information on the registration process, dispelled common myths based on literature findings, emphasized the importance of becoming an organ donor, and provided links to more resources so that patients could seek additional information if interested. The Trillium Gift of Life Network was contacted and permission was granted to use their logo on the pamphlet. At the bottom of the information pamphlet was a cut-off portion asking patients for their contact information (Name, Date of Birth, Phone Number), whether they were currently registered as an organ donor [Yes/No/Unsure/Prefer not to answer], if they would like to learn more about organ donation [Yes/No], and permission to contact patients in subsequent follow-up regarding their registration status. This cut-off portion would be collected by the medical resident, clinical clerk, or office secretary in the waiting room during subsequent PDSA cycles. In the first PDSA cycle, we were primarily interested in pilot testing the information pamphlet for clarity, comprehension, and persuasion. We distributed the pamphlet to a convenience sample of nine patients at the clinic where the QI initiative would be implemented. Patients were asked to rank the clarity of the pamphlet on a ten-point Likert scale and provide any feedback for improvement. Given the sensitivity of the topic of organ donation, we also asked patients to discuss any discomfort elicited by the information presented in the pamphlet. Additionally, we asked patients about their current organ donation status and whether the information conveyed would sway them to register as an organ donor, in order to pilot test the effectiveness of the pamphlet. The complete list of questions asked to patients in PDSA 1 is provided in Appendix 2. The office staff was also invited to provide comments that helped us revise the pamphlet for the second PDSA cycle. Edits were made to clarify information that was unclear to patients. For example: we clarified the statement “You cannot be too old or too sick to register as a donor” to explain that pre-transplant assessments would be conducted.
In the second PDSA cycle, the revised pamphlet was distributed to patients in the clinic waiting room (see Appendix 3 for a copy of the pamphlet). While the pamphlet contained the website registration information, the organ donation registration form, retrieved from the Trillium Gift of Life Network, was attached to the pamphlet to make the form more readily accessible to patients and thus, expedite the registration process. The team physically collected the completed registration forms from patients and placed them in a drop box. The cut-off portion of the information pamphlet was also collected in order to gather baseline data for each patient. The registration forms were reviewed by the student team members for completion prior to mailing them off to Trillium Gift of Life. The aim of the second cycle was to test the feasibility of providing the registration form along with the informational pamphlet and provide a more convenient method for patients to register as organ donors. Feedback from the patients was positive in regards to the incorporation of the registration form. The medical staff also provided positive feedback about the convenience of the form and did not raise any concerns about the intervention diverting time away from their clinical duties.
In the third PDSA cycle, we continued to improve the educational pamphlet for patients, replacing a statistical fact with a graphic, as this is a key persuasive tactic often utilized in advertising and marketing to appeal to audiences.16 ,17 The pamphlet distributed in PDSA 3 is provided in Appendix 4. The medical staff continued to provide patients with the pamphlet and registration form and collect the cut-off portions from the pamphlet which contained the baseline personal information. Patients who completed the registration form returned them to the clinic staff to be mailed to Trillium Gift of Life (See supplementary – Appendices 1-4).
supplementary appendices
Results
Based on the interviews conducted in PDSA Cycle 1, our informational pamphlet was well received by patients. The average rating of the clarity of the pamphlet was 9.1 on a ten-point Likert scale, with the lowest score being a 7. Nobody expressed any discomfort based on the information presented in the pamphlet and only one patient required further clarification of the wording in one of the phrases (which was subsequently revised). Two of the patients that were non-donors felt compelled to register after being presented the information on the pamphlet. A third patient also expressed an interest in donating on the basis of the intervention but cited an inability to do so based on religious beliefs. Ultimately, we were satisfied with patient's receipt of our intervention and its potential effectiveness and made the necessary modifications based on patient feedback before proceeding to PDSA cycle 2.
We distributed 30 pamphlets and registration forms in each of the subsequent two PDSA cycles and calculated the improvement in the number of registered donors. We included drop-outs in our final analysis, similar to an intention-to-treat analysis, in order to be conservative in our interpretation of the results and avoid overestimating an effect size. The goal was to increase organ donor registration by 10% overall.
As demonstrated in Figure 1, 23 pamphlets were returned in the second PDSA cycle, of which 4 individuals were already pre-existing organ donors. This corresponded to a baseline organ donor rate of 13.3%. Of the 19 remaining participants and 7 drop-outs, 5 individuals returned a new organ donor form, signifying a 19.2% new donor registration rate and a total registration rate of 30.0% over the course of PDSA 2.

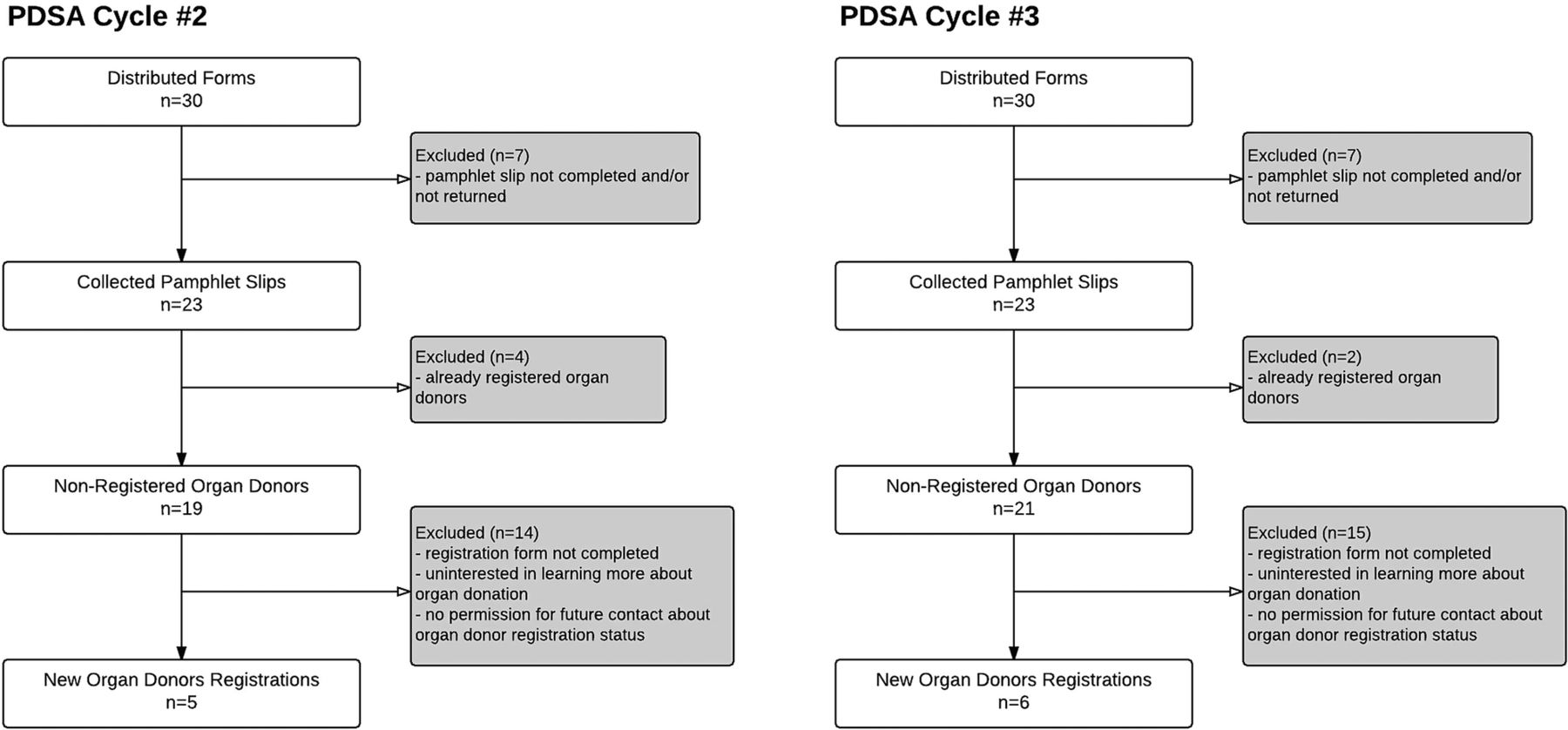{kind=link}
In the third PDSA cycle, 23 of the 30 pamphlets were returned, but this time only 2 individuals were registered as pre-existing organ donors. This corresponded to a baseline registration rate of 6.7%. 6 of the 28 participants who were non-donors completed and returned an organ donor form, constituting a 21.4% new donor registration rate and a total registration rate of 26.7% in this sample and a 20.0% increase in donor registration in PDSA cycle 3.
Overall, we recruited 11 new donors over the course of the two PDSA cycles, thereby leading to an increase in registered donors from 10.0% to 28.3%. This QI initiative resulted in a 18.3% increase in the number of registered organ donors within this primary care practice surpassing our goal of 10%.
Lessons and limitations
A number of valuable lessons were learned from this initiative. The importance of accessibility was a pivotal and positive finding. Attaching the organ donor registration form directly to the information pamphlet provided patients with an accessible method to register and we hypothesize that this reduced the number of delayed registrants. We also speculate that paper, which serves as a tangible visual reminder, may be particularly effective in a primary care office over online forms. In future studies, it could be of value to interview patients directly and ask them which factors are most important to them when deciding whether or not to register - more specifically, if it was the act of receiving a paper form, the setting of a primary care clinic, or the information pamphlet that influenced their decision to register.
In order to further validate our findings, it is also necessary to replicate this project with a larger sample size. Over the course of the two PDSA cycles, 14 of 60 participants did not return the pamphlet, corresponding to a drop-out rate of 23.3%. It is possible that there may be meaningful differences between the characteristics of our sample and non-responders; therefore, the possibility of non-response bias should be taken into account in the interpretation of our results.
Following review of the completed consent forms prior to mailing them in, it came to light that the Trillium Gift of Life organ donation consent form was not fully intuitive to patients, as several had filled the information out incorrectly. This suggested the need to review the form with the patient upon receipt, in order to clarify any misunderstandings and make necessary corrections. This may be difficult to achieve in a community-based clinic where residents or clerks are not readily available to individually review each registration form prior to collection. The lack of clarity in the Trillium Gift of Life form also poses other challenges for patients. For example, our patient population represented an ethnically diverse group of individuals, where English was not necessarily their first language. This was taken into account in the creation of our educational pamphlet as we sought to create text that had an appropriate reading level. Language barriers may have limited some patients' ability to comprehend the registration form and potentially deterred them from filling out the form altogether. Therefore, it is possible that the number of registrants in this study does not represent the true number of patients who actually wished to register.
This QI initiative was tested at the project champion's medical practice, which meant that we were working with a supportive and involved physician, who was well versed in quality improvement and had access to resources that facilitated the implementation of this initiative, namely the support of a medical resident and clinical clerk. Recognizing this, it is important to identify that some medical practices, especially those in remote areas, may lack the human resources required to carry out such a project. Furthermore, physicians may be apprehensive to adopt this initiative due to a lack of knowledge about the organ donation process as well as the sensitive nature of this topic. Given that patients may have questions related to the registration process that they wish to discuss with their physician, it is important to ensure that primary care physicians are informed about the organ donation process and feel comfortable discussing the topic with their patients.18 Therefore, it may be beneficial to complement this intervention with physician education. Additionally, physicians may be concerned that raising the topic will divert time away from the patient's primary reason for their visit or alternatively, prolong each patient's visit. To mitigate this, it is important to review the physician's office workflow to determine how this initiative could be best tailored to fit into their current practice. Our team had success with either the office secretary or a medical learner distributing and collecting the forms. We hypothesize that this approach could be easily adapted to fit the logistical workflow and availability of human resources in other clinics that would also like to implement this project.
Moreover, it is important to prevent the patient from feeling pressured to fill out the consent form on the same day that the form is given out. Rather, the purpose is to simply offer key information regarding the organ donation and registration process, facilitating knowledge transfer to patients so that they can understand the critical need for organ donations and make an informed decision about whether or not to register.
While we can speculate that our results will be generalizable, this study was only performed at a single physician's practice in Scarborough, Ontario. However, the diversity of the practice adds positive predictive value for other physician practices. Additionally, this project's findings is limited by the small sample size (69 patients engaged in total).
Another inherent limitation in this project is that we did not follow-up with patients who failed to return the registration form on the day of their visit. This would imply that our results only reflect the number of forms submitted on the day of the patient visit, when in fact the number of newly registered donors could have been even larger had patients individually mailed in their forms from home or registered via the website. In the future, patients should be followed up via phone call to confirm whether or not they actually registered and provided consent, in order to gauge an accurate estimate of donor registration rates following this intervention.
Conclusion
This initiative had significant and meaningful findings, namely the ability to facilitate the organ donor registration process through the direct provision of a registration form as well as the ability to coordinate this process within a clinical environment. By increasing awareness and linking organ donation to a physician's office, we saw an 18.3% increase in patients that completed organ donor registration consent forms. This initiative therefore adds unique insight into factors that may promote organ donation registration.
Moreover, our intervention increased donor registration above the baseline rates in both the city of Scarborough and Toronto, Ontario. Therefore, this QI initiative may be an effective option to continue to increase organ donor registration in clinics throughout Toronto. We anticipate continued improvement in registration rates with this methodology. Since there is a lack of literature on this specific method of increasing organ donation registration, we hope that the results of this project encourage other physician groups to consider implementing this strategy.
Acknowledgments
We would like to thank Alexandra Mardimae, Joyce Lui, and Rizza Love Turalba for their assistance with data collection at the primary care clinic.
Footnotes
Declaration of interests None declared.
Ethical approval No ethics approval was required for quality improvement study initiated at our institution.