Article Text

Abstract
Ultrasound scan (USS) is a common and important mode of investigation for emergency surgical admissions. Delay in investigation often leads to delayed diagnosis and treatment, and possible extended length of stay (LOS), which has clinical, cost and service provision implications. We aim to investigate the clinical impact on patient care and the cost-effectiveness of a pilot Surgical Assessment Unit (SAU) USS facility. We performed a retrospective data collection on 100 consecutive SAU inpatients who had an USS investigation on the ward since the introduction of the facility, matched by 100 consecutive SAU inpatients who had an USS in the radiology department before the pilot study. Results of the audit show SAU USS has a reduced mean LOS by 1.44 days compared to departmental USS, and led to more same day discharge than departmental USS (20 vs. 5), thus avoiding unnecessary overnight stay. It also significantly reduced mean waiting time from admission to investigation by 5.21 hours, which can be translated into improved patient and staff satisfaction. All these findings are both statistically and clinically significant. The estimated cost of each SAU USS is comparable to the average departmental USS (£29.71 vs. £30.80). Using the average cost of an excess bed day = £273, SAU USS has produced an estimated saving of £394.72/patient. This does not include saved opportunistic costs such as prevented elective operation cancellations, fines incurred from surgery waiting time/A+E breaches etc. To conclude SAU USS has a significant positive impact on patient care in surgical admissions by reducing LOS and investigation waiting time, as well as facilitating same day discharge.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
Ultrasound scan (USS) is a common and important mode of investigation for emergency surgical admissions, as well as a non-invasive and relatively cheap examination. Delay in investigation often leads to delayed diagnosis and treatment, and possible extended length of stay (LOS), which has a clinical impact to patients, cost implication to the NHS trust, and a potential impact to service provision due to bed shortage and cancellations of elective procedures etc. A trial of a ward-based USS facility was introduced in Derriford Hospital in October 2013 to try to improve the effectiveness of USS investigations for acute surgical patients. Despite very positive users report and feedback since the introduction of the pilot scheme, the viability of the service was threatened as there was a lack of funding.
Background
Acute surgical assessment/admissions units are common amongst acute hospitals in the UK, and they facilitate an efficient initial surgical assessment and management. In recent years there has been a growing interest in the development of supporting services to facilitate and improve the effectiveness of patient care in these units. Ultrasound scan, in particular, being one of the most common investigations in emergency surgical admissions, has been introduced as part of the surgical assessment/admissions facility in many hospitals. However currently there has been little report about the clinical impact and cost effectiveness of a surgical assessment unit ultrasound facility.
Baseline measurement
We performed a retrospective data collection on 100 consecutive SAU inpatients who had an USS in the radiology department before the pilot study (between 27th August and 30th September 2013). Lists of patients were generated from the radiology department database using filters of ‘investigation room’ and ‘referring location’ respectively. All outpatient and out of hours investigations were excluded from the study.
Design
A trial of the SAU USS facility commenced in Derriford Hospital in October 2013 as a pilot scheme, with the aim of assessing the clinical impact on patient care in the surgical assessment unit. A clinical room in the SAU was converted into a sonography room. An SAU USS booking sheet was devised, with 10 USS slots available between 09:15 and 12:35 (20 min each). The booking sheet is to be filled in the admission team before the start of the list. A cost-effectiveness analysis was also commissioned to look at the sustainability of the service.
Strategy
After the first few weeks of introduction of the pilot SAU USS service, a users survey was conducted by online questionnaire tool ‘Survey Monkey’. There was a unanimous positive feedback by referrers (surgical consultants, GPs and ward staff), together with comments on how to improve the service. We subsequently performed a retrospective data collection on 100 consecutive SAU inpatients who had an USS investigation on the ward since the introduction of the facility (from 21st October to 13th November 2013), matched by 100 consecutive SAU inpatients who had an USS in the radiology department before the pilot study (between 27th August and 30th September 2013). Lists of patients (n=200) were generated from the radiology department database using filters of ‘investigation room’ and ‘referring location’ respectively. All outpatient and out of hours investigations were excluded from the study.
Results
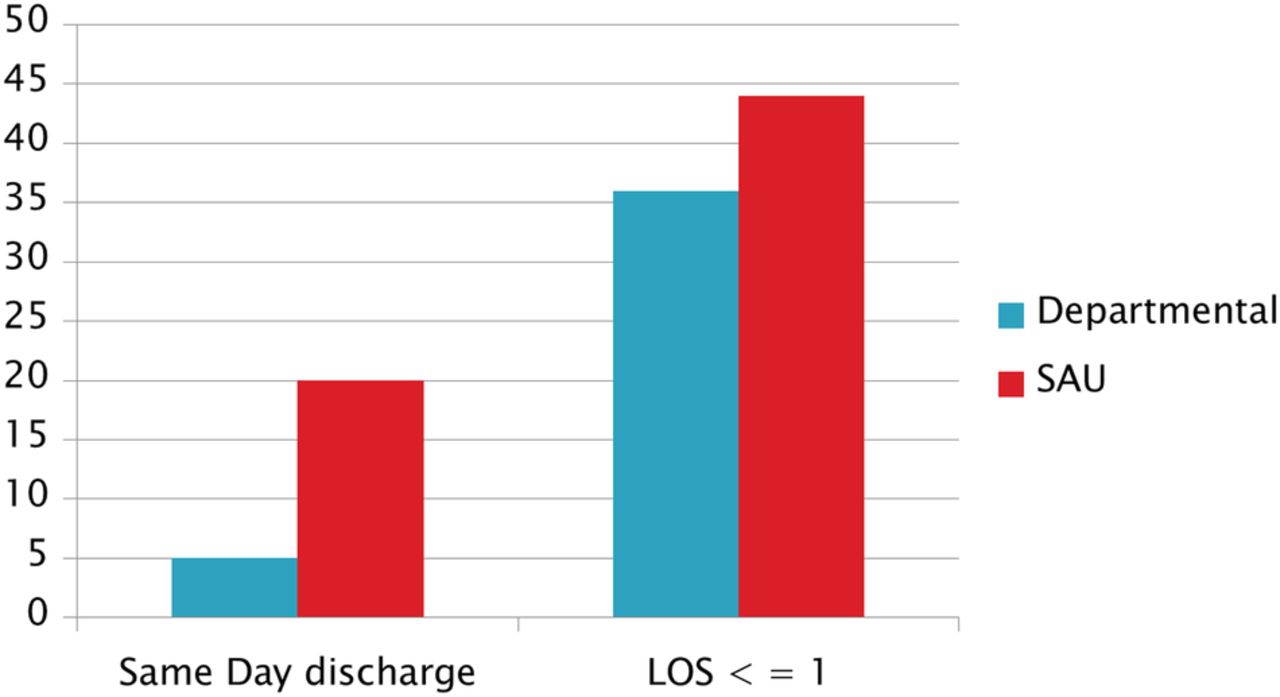
SAU USS has a reduced mean LOS by 1.44 days compared to departmental USS (p = 0.0382, 95% CI of mean reduction = 2.90, 0.079) (Table 1), and led to more same day discharge than departmental USS (20 vs. 5, p = 0.034) (Table 2), thus avoiding unnecessary overnight stay (Fig. 1). There was no difference in readmission rates between the two groups (both 0.17). It also significantly reduced mean waiting time from admission to investigation by 5.21 hours (p = 0.0112, 95% Cl of difference = 1.20, 9.22) (Table 3), which can be translated into improved patient and staff satisfaction. All these findings are both statistically and clinically significant. The estimated cost of each SAU USS is comparable to the average departmental USS (£29.71 vs. £30.80). Using the average cost of an excess bed day = £273 (Department of Health Reference Costs 2012-13, November 2013), SAU USS has produced an estimated saving of £394.72/patient. This does not include saved opportunistic costs such as prevented elective operation cancellations, fines incurred from surgery waiting time or A&E breaches etc. The annual running cost of SAU USS has been estimated as £50,919, with an estimated set up cost of £52,010. These can be covered by savings achieved from 129 and 132 SAU scans (19 and 20 work days) respectively.⇓⇓


{kind=link}
{kind=link}
Lessons and limitations
The authors acknowledged that this is an audit with an aim to improve our current acute surgical service provision based on two improvement cycles. It has the limitation of a short study period.
Since the pioneering and audit of the SAU USS service in 2013, to this day (at the time of article revision in March 2017) the facility has sustained and continued its service despite three ward moves of the SAU, and has now become an established and integral part of the service provision in our surgical unit. There are 10 USS slots per day from Monday to Friday allocated between the SAU and Acute Care Unit, and our recent data has shown a near 100% utilisation of the slots. It is our plan to repeat the audit (third improvement cycle) to confirm an ongoing benefit of the service in terms of reduced LOS and waiting time for investigation, as well as cost-effectiveness of the service.
A potential development of the SAU USS facility is to extend the current successful weekday service to the weekends. We believe that the same benefits of reducing LOS and facilitating same day discharge can be transferred to the weekends, and in particular improving the issue of ‘bed-blocking’ during the weekends as a result of patients waiting for inpatient investigations. However, as in the ongoing debate of a ‘Seven day NHS’, appropriate resource and staff allocation are essential requirements for any further development of this service.
Conclusion
SAU USS has a significant positive impact on patient care in surgical admissions by reducing LOS and investigation waiting time, as well as facilitating same day discharge. Therefore it has been recommended to the trust as a long term service provision. SAU USS has a significant cost benefit with a saving of nearly £400/patient. This is particularly relevant and important to the current financial and operational burden of the NHS. Therefore it has been recommended to the trust as a self-sustainable and economic long term service provision, and has been running up to this date.
Acknowledgments
Mark Edmond, junior doctor in Plymouth Hospitals NHS Trust.
We would like to thank the Plymouth Hospitals NHS Trust radiology department for providing the original data on the SAU USS.
We also thank the Plymouth Hospitals NHS Trust General Surgery Directorate for the financial figures quoted in the article.
Footnotes
Declaration of interests Nothing to declare
Ethical approval This project was exempt form ethical approval as it was deemed an audit.