Article Text

Abstract
Over the last decade, patient volumes in the emergency department (ED) have grown disproportionately compared to the increase in staffing and resources at the Toronto Western Hospital, an academic tertiary care centre in Toronto, Canada. The resultant congestion has spilled over to the ED waiting room, where medically undifferentiated and potentially unstable patients must wait until a bed becomes available. The aim of this quality improvement project was to decrease the 90th percentile of wait time between triage and bed assignment (time-to-bed) by half, from 120 to 60 minutes, for our highest acuity patients. We engaged key stakeholders to identify barriers and potential strategies to achieve optimal flow of patients into the ED. We first identified multiple flow-interrupting challenges, including operational bottlenecks and cultural issues. We then generated change ideas to address two main underlying causes of ED congestion: unnecessary patient utilization of ED beds and communication breakdown causing bed turnaround delays. We subsequently performed seven tests of change through sequential plan-do-study-act (PDSA) cycles. The most significant gains were made by improving communication strategies: small gains were achieved through the optimization of in-house digital information management systems, while significant improvements were achieved through the implementation of a low-tech direct contact mechanism (a two-way radio or walkie-talkie). In the post-intervention phase, time-to-bed for the 90th percentile of high-acuity patients decreased from 120 minutes to 66 minutes, with special cause variation showing a significant shift in the weekly measurements.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See:
Statistics from Altmetric.com
Problem
The Toronto Western Hospital (TWH) is an academic tertiary care centre in Toronto, Canada. In 2015, the TWH ED had approximately 64,000 patient visits. Despite increasing demand for services by the community - indicated by a 6% annual growth in patient volume over the last ten years - there has not been a proportional increase in resources for staffing or infrastructure.
Greater patient volumes in emergency departments (EDs) create congestion and can compromise the delivery of high quality patient care.1 ,2 When all ED beds are occupied, patients who are waiting to be seen, including those with high-acuity concerns, must remain in the waiting room until a bed becomes available. Following a brief clinical assessment, the ED triage nurses are responsible for monitoring these medically undifferentiated and potentially unstable patients until they are assigned to an ED bed. Concurrently, triage nurses must also evaluate new patients as they arrive for registration. As the number of patients presenting to the ED outpaces the number of beds available, the increasing patient-to-provider ratio in the waiting room creates an unsafe environment for high-acuity patients and a precarious medico-legal situation for providers.
This project aimed at facilitating the flow of high-acuity patients from the waiting room to a bed in the ED, where comprehensive assessment and close monitoring can be performed by the ED health-care team.
Background
A patient presenting to the TWH ED first sees the triage nurse who performs a brief assessment to determine the severity of the patient's complaint, which is used to prioritize patient care needs.3 Once the subsequent administrative registration is completed and unless they require immediate and critical medical attention, patients remain in the waiting room until a bed becomes available in the ED.
The TWH ED contains one resuscitation room and 21 monitored beds designated for the management of high-acuity patients. There are also 17 unmonitored beds and many more chairs designated for lower-acuity patients. Once a patient is assigned to a bed, members of the health-care team perform a comprehensive assessment, order investigations as required, and determine the course of treatment. As a result of the typically high volumes of patients seen on any given day and the length of time required to manage patients' complaints, most ED beds at TWH are continuously occupied. This leads to an increasing number of patients bottlenecked in the waiting room.
Our team has previously published in BMJ Quality Improvement Reports our experience to improve the waiting time of patients with low-acuity complaints.4 The aim of this quality improvement project was to improve the flow of patients with high-acuity concerns from the waiting room to a monitored ED bed, in order to facilitate timely access to care. The scope of this project was limited to ED-related processes, with hospital-wide issues affecting the flow of admitted patients to inpatient wards beyond our scope.
Baseline measurement
Our primary outcome measure was time-to-bed - the length of time between triage and assignment to a monitored bed for high-acuity patients, measured in minutes. Time-to-bed was abstracted from an administrative database. The 90th percentile (P90) is a default metric for public reporting in our institution, and allowed us to capture the expected experience of nine patients out of ten. Our baseline measurement captured 2,354 patient visits over a 9-week period, revealing an average weekly P90 time-to-bed of 120 minutes. We set a stretch goal of reducing the P90 time-to-bed for high-acuity patients to 60 minutes (a 50% improvement), within three months. Data analysis was performed using CHARTRunner (V3.6, PQSystems, Dayton, OH).
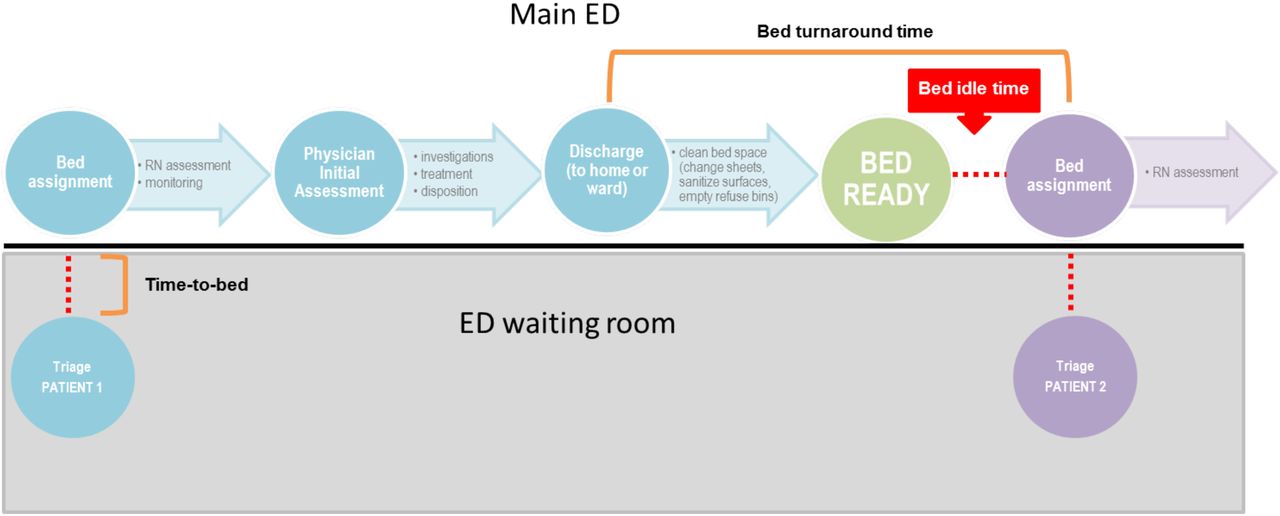
As a process measure, we tracked bed turnaround time – the length of time between two successive patients occupying a bed (i.e. time elapsed between patient 1 leaving and patient 2 arriving; see Figure 1), measured in minutes. On-site audits were performed by volunteers and revealed that bed turnaround could be further sub-divided into the following components: (1) notification period: bed status is updated to ‘needs cleaning’ by clinician on the digital information management board (the ‘WhiteBoard’), and notice is received by environmental services team; (2) cleaning time: environmental services team cleans the bed space (includes changing sheets, sanitizing all surfaces, and emptying refuse bins), and updates bed status on WhiteBoard to ‘clean’; (3) bed idle time: time elapsed between notification of a clean bed on WhiteBoard and a new patient assigned to bed by triage nurse. Audits revealed that bed turnaround lasted 48 minutes on average (see Figure 2 for component times).

Illustration of the bed flow process from triage through discharge for two successive patients.

Breakdown of component periods of bed turnaround time process.
Design
This project was constrained to the ED operational budget, so cost-neutral improvement strategies were designed and implemented (i.e. no physical space or providers were added). We conducted in-depth stakeholder analysis to inform our change ideas. Stakeholders included front-line health-care providers, medical and nursing leadership, clerks, and environmental services team. The analysis highlighted two potential issues: inefficiencies in the demand-capacity ratio of patients-to-available beds and unnecessary delays in bed turnaround processes.
The first change idea addressed the inefficient utilization of monitored beds. Some patients require the use of a monitored bed for the duration of their visit (e.g., for ongoing cardiorespiratory monitoring), while others are considered stable following their initial clinical assessment and during their investigative and treatment period. This latter group does not require a bed and could tolerate transfer into an alternative location, which we created and called the ‘Transitional Care Area’ (TCA). The TCA is where ED patients continued to be observed for the duration of their ED visit while not necessitating a bed, thereby freeing up the bed they were previously utilizing for new patients. Several PDSA cycles were performed to test various combinations of locations and processes for the TCA concept.
The second issue identified by stakeholders involved delays within bed turnaround time. With involvement from front-line ED staff and clinicians, we produced a flow chart detailing the process of preparing a room for a new patient after the previous patient is discharged. Our stakeholder group felt that the ‘notification’ and ‘cleaning’ components of the process were unlikely to be meaningfully shortened, but determined that the ‘bed idle time’ was inappropriately long and could likely be improved. Our second change idea therefore focused on decreasing bed idle time by improving the communication between the environmental services team, who cleans the beds, and the triage nurse, who assigns new patients in those beds.
Strategy
We conducted seven PDSA cycles to test the TCA and the improved communication strategies, in order to more efficiently use monitored bed space and decrease bed idle time for these beds, respectively. During each cycle, our core project team engaged various members of the ED staff, including front-line (bedside) nurses, nursing and administrative managers, clerks and physicians.
PDSA CYCLE 1: ELIGIBILITY CRITERIA
The objective for PDSA cycle 1 was to create a comprehensive and useable list of criteria to identify patients appropriate for the TCA. The core project team and clinical staff delegates, including nurses and physicians, contributed to the development of the decision-making aid. Multiple iterations were created, using as a backbone the hospital's standards for admitted patients to be temporarily moved to inpatient units' unmonitored hallways. Various iterations of the list focused either on inclusion criteria (i.e. patients must fulfill all of them) or on exclusion criteria (i.e. patients cannot fulfill any of them), and varied from very detailed and narrow to broad and generic. The final list focused on the broad set of exclusion criteria that would preclude patients from being moved out of their monitored beds: hemodynamic instability or acute change in oxygen requirements, need for continuous telemetry monitoring, altered level of consciousness (including delirium and dementia), intoxication or agitation, patients psychiatrically unstable or unsafe, patients fully immobile requiring a bed, and those requiring airborne, droplet, or contact precautions for infection control reasons.
PDSA CYCLE 2: FEASIBILITY AUDIT
For PDSA cycle 2, we hypothesized that 2-4 patients fully assessed by a physician and nurse (in our 21-bed monitored area) would be deemed appropriate for the TCA utilizing the decision-aid. We undertook feasibility audits at various times of the day, with the majority of audit events revealing at least two patients meeting the criteria. Typically, eligible patients were awaiting results of laboratory or imaging tests, being observed for response to treatment, or receiving intravenous solutes or medications prior to discharge.
PDSA CYCLE 3: LOGISTICS
The objective for PDSA cycle 3 was to determine the most functional format and location for the TCA. The main waiting room was felt to create a poor patient experience; the hallway was felt to be too crowded to move additional patients into; and the ambulatory zone was too far removed from the high-acuity zone and may have created an ‘out of sight, out of mind’ situation that could have led to worse and delayed care. The final concept was to transform one of the 21 monitored rooms (with had one bed) into an area with four chairs (one of which would have access to cardiorespiratory monitoring). The net gain (one less bed but four extra chairs) would therefore be of three additional patients potentially being managed in our department at any given time.
PDSA CYCLE 4: LOCATION AND STAFFING ASSIGNMENT
The objective of PDSA cycle 4 was to modify existing nursing assignments to ensure fair workload and adequate workflow, and alleviate patient safety concerns. Various rooms were considered for the TCA, given considerations of size, proximity to the nursing station, amenities specific to certain rooms that we did not want to lose (e.g., isolation with ante-room, dialysis capability, etc.). Through discussions with the front-line nurses, we determined the best arrangement for the TCA and adjacent rooms.
PDSA CYCLE 5: OPERATIONAL TIMING
For PDSA cycle 5, we hypothesized that the operational hours of the TCA would be optimized during typical ED high occupancy periods (i.e. weekday evenings). We tested operational timing and capacity of the TCA during morning, afternoon, and evening periods, on weekdays and on weekends. After multiple attempts, we discovered that on most occasions, most patients located in monitored beds in our ED had exclusions that precluded them from being moved to a chair in the TCA - most often relating to isolation or cardiovascular telemetry requirements. In practice, typically fewer than two patients met TCA eligibility criteria during our tests of change, resulting in no net gain of managed patients in the department.
DECISION POINT: TCA IN PRACTICE
As we hypothesized, late evening periods were the optimal time for TCA operation from a patient-need perspective. However, this period coincided with lower nursing coverage and fewer nurses available to safely care for additional patients (a request for additional nursing coverage was not accepted). Moreover, as an as-needed solution, time for set-up and take-down was required to convert the space from a monitored bed to the TCA space, which made the process inefficient. For these reasons, we elected to pivot away from a TCA solution and to focus on other means of achieving our aim.
PDSA CYCLE 6: IN-HOUSE HIGH-TECH SOLUTION
Moving away from TCA, PDSA cycle 6 addressed the hypothesis that optimization of efficient but under-used in-house technology would be easy and useful to the providers to reduce bed turnaround time. We engaged front-line staff, including environmental services and nurses, to clarify and refine the process of using the in-house digital information management board (the ‘WhiteBoard’) to communicate the availability of clean beds between ED staff. In practice, however, the inconspicuousness of this notification was inefficient in the context of the rapid and high-traffic triage process - recognition and response to the signal by the triage nurses did not happen in a timely fashion.
PDSA CYCLE 7: LOW-TECH SOLUTION
We hypothesized that a more effective signal for triage nurses would have to be more noticeable, without being a disruption to their workflow. Despite the availability of the high-tech WhiteBoard, we elected to try other low-tech methods to balance the priorities of achieving timely recognition and response to the signal and maintaining an uninterrupted workflow. A pair of walkie-talkies was assigned to the environmental services team and to the triage nursing station. Once a clean bed became available, the environmental services team would notify the triage nurse by sending a one-way ‘ping’ via the walkie-talkie. This unobtrusive signal allowed the triage nurse to finish his or her current task, but to be aware to focus on patient assignment to the clean bed as soon as possible. All parties involved found the process user-friendly and useful.
Results
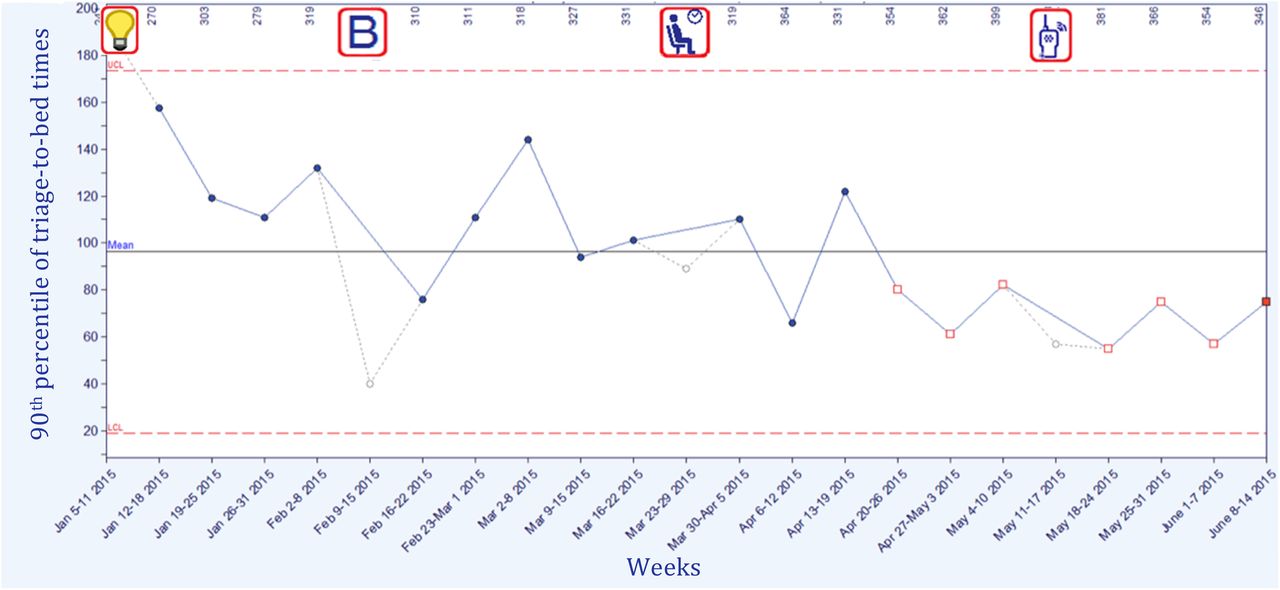
Results are shown in the Shewhart chart in Figure 3. Prior to the first PDSA cycle, the baseline average P90 time-to-bed was 120 minutes (Figure 3, “B” symbol). PDSA cycles #1 to 5 targeting the TCA occurred from mid-March to mid-April, 2015 (Figure 3, patient in chair symbol), with no clear and consistent shift of the weekly P90 time-to-bed. Starting in mid-April, we shifted our focus to improving communication strategies in the bed turnaround process and, following iterative testing, the final walkie-talkie process was operationalized in May (Figure 3, radio symbol).

{kind=link}
{kind=link}
{kind=link}
Shewhart chart of weekly 90th percentile of triage-to-bed times. Numbers on the x-axis indicate the weekly volume of high-acuity patients. The Shewhart chart rule for special cause variation was satisfied by the final eight weekly measurements, indicated on the chart by the open red squares. Legend: light bulb – project conception; B – mid-baseline period; patient in chair – TCA testing; walkie-talkie – bed turnaround streamlining.
The implementation of improved communication strategies in PDSA cycles 6 and 7 coincides with the onset of a significant shift in P90 time-to-bed in the final eight-week period of measurement in the Shewhart chart. During this period, the weekly P90 time-to-bed was 66 minutes on average (our stretch goal was 60 minutes). Bed idle time, our process measure, was observed to have decreased to 13 minutes following PDSA cycles 6 and 7 (baseline: 26 minutes).
Lessons and limitations
This project benefitted from early buy-in and support from institutional leadership. The goals of this project were aligned with organizational and governmental health care priorities, allowing our team to be afforded time and resources to dedicate to the project.
As project leads, we were reminded that front-line staff engagement is vital to the success of any initiative. Our staff were integral in supporting the changes we sought to implement, and we engaged them through the application of adaptive leadership principles: involvement of trusted champions and leaders in the ED, continuous communication via email and daily huddles, and creating a safe and open environment where any staff member could voice issues with an intervention, and importantly was encouraged to offer alternative solutions to emerging challenges. We employed the Highly Adoptable Improvement (HAI) model in order to increase the sustainability of our initiative. The HAI model states that the success of a healthcare improvement is dependent on a balance between the perceived value of an initiative and the resulting change in workload by providers.5 Throughout the project, we attempted to simplify the work needing to be performed by various providers to improve patient flow. We also emphasized the positive impact on patient safety, while acknowledging the change in workflow for nursing and other clinical staff intended to receive additional patients inside the department. By rallying the team with the over-arching theme of improvement of the overall patient experience, we were able to make significant gains.
Despite our theoretical knowledge of the need for small, rapid, and repeated tests of change, as project leads, we reflected that we likely spent too much time trying to design the perfect system at the outset. We discussed and conferred at length with colleagues about the best way to operationalize various elements of the TCA or to develop the safest eligibility criteria and most user-friendly and screening tool - rather than implementing and modifying during subsequent PDSA cycles. Although this may not have affected the final outcome, it did delay the initial operationalization of our project.
Conclusion
Our project aimed to improve time-to-bed for the sickest patients in our urban academic tertiary care centre. Using adaptive leadership, the Highly Adoptable Improvement model, and testing old and modern information technologies, we aimed to decrease time-to-bed by 50% within three months. Average time-to-bed decreased from 120 minutes at baseline to 66 minutes following seven PDSA cycles. Change ideas included defining and creating a ‘Transitional Care Area’, where stable patients could be transferred from their monitored bed to spend the remainder of their ED visit after initial assessment, as well as the use of walkie-talkies to improve communication during the bed turnaround process. We believe that our results can be replicated in other EDs using similar quality improvement methods and adapting solutions to the local context, and we are currently testing a similar model of care at our second institutional ED site.
Acknowledgments
This project was facilitated by the Health Quality Ontario IDEAS program (Improving & Driving Excellence Across Sectors). We wish to acknowledge Joe Mauti for his mentorship in conducting this study. We also thank the TWH core team for their support: Mary Kay McCarthy, Dr. Anil Chopra, Dr. Sam Sabbah, Kathy Bates, Dr. Steven Friedman, and Jason Dickson.
Footnotes
Declaration of interests Nothing to declare.
Ethical approval All data analyzed for the purpose of this study were collected as part of routine quality assurance processes; only de-identified aggregate metrics were provided to the study team for analysis. No identifying information or patient data was collected. This project was reviewed by the Research Ethics Board at University Health Network and was deemed to be a quality improvement initiative and thus exempt from the ethics review requirement.