Article Text

Abstract
Clinicians can enable patients to actively participate in their care but communication with patients is often poor and highly variable. The aim of this study was to explore patients’ understanding of their current illness while in hospital and using a codesign process to create prototype tools to facilitate better communication during ward rounds.
A mixed-methods, multistep design with step 1: Application of a questionnaire addressing domains of care in the acute medical unit; step 2: Development of communication aids that were codesigned with active help of patients, students and a specialist in user centric design to address patient needs and step 3: Evaluation of tools with patients in four Plan–Do–Study–Act cycles.
In the initial survey of 30 patients 12 (40%) patients did not know what their diagnosis was and 5 (17%) did not know the results of recent key tests. 20 (67%) patients felt that staff communication and coordination could be improved.
An intervention was prototyped with four variations: (1) An A6 ward-round summary sheet completed by doctors during ward rounds. The system worked well but was highly person dependent. (2) An A4 patient-owned diary (‘How to Hospital’) that contained information about key processes in hospital and space to document conversations from rounds and prompts for questions. 10 patients read the diary and commented favourably but did not complete any pages. (3) ‘Diary-cards’: a basic set of information cards was given to patients on admission to hospital. (4) Patient specific ‘diary-cards’ were completed by clinicians—10 forms were piloted during rounds and improved subsequent day information retention of diagnosis to 80%.
Our study identified interventions that were feasible but remained person-dependent. The patients’ ownership of information in relation to their care might facilitate retention and satisfaction but the optimal format for these interventions for enhancing communication remains unclear.
- clinical microsystem
- hospital medicine
- patient-centred care
- patient participation
- quality improvement
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
The Ysbyty Gwynedd is a 500-bed district general hospital in Bangor, North Wales and serves a population of 220 000 in a largely rural area with a significant population that speaks Welsh as their first language.
The hospital has 21 wards of which 10 are under the department of Medicine and admits a mean of 1000 patients per month through the acute medical unit (AMU). Patients will present with a broad range of acute presentations including left-ventricular failure, pneumonia, asthma, diabetes, acute renal failure, ischaemic heart disease and geriatric syndromes and will spend between 4 and 72 hours in the AMU for their initial assessment, treatment and monitoring. Patients throughout the hospital will be seen by doctors on ward-rounds each weekday and additionally if unwell or after new test results become available.
The inspiration for this project was the troubling personal experiences of the authors when their relatives became patients at the hospital. The patients knew little about their condition, treatment and results of tests, and generally felt they had minimal understanding and received little input from providers about their care. The communication was difficult for the authors when as healthcare providers, they were related to the patients. The experience was the same for different relatives in different departments, regardless of the first language of the relative or staff.
The authors reflected on what was causing the problem and how we could contribute to improvement. Early efforts in talking to patients made it evident that they felt that too much information was given to them over a short period of time, typically during review on ward rounds, with little effort to assure they understood or remembered the information. It appeared that information recall and overload might be key problems.
Our SMART aim was to increase the proportion of patients who recalled their diagnosis by at least 20% in our AMU in 3 months. We aimed to explore patients’ understanding of their current illness and codesign tools to facilitate knowledge transfer.
Background
The experience of being a hospital inpatient has been described as ‘one of the most disempowering situations one can experience in modern society’1 and it is important to consider how much poor communication factors into this statement. Poor communication can contribute to adverse events, harm and patient dissatisfaction.2–4 Good communication might increase patient satisfaction, adherence to treatment and activation.1 5–8 The majority of complaints at our hospital and others are directly related to poor communication either with patients or their relatives and a large proportion of National Health Service litigation is related to poor communication.9
A systematic review of the literature by Harrington et al6 examined interventions aimed to improve communication between doctors and patients. The majority of included studies were based in primary care or in outpatient settings. Although there are numerous observational studies on lack of knowledge among hospital inpatients, there is limited literature on initiatives to improve communication within a hospital inpatient setting.
Standards and frameworks for communication
The National Institute for Health and Care Excellence states that clinicians should be ‘enabling patients to actively participate in their care’ with the necessary information to allow them to do this.10 Patients cannot actively participate in their care if they do not have the necessary information and agency required to take part in decision making. ‘Shared decision making’ and the importance of embracing this in healthcare is not achievable if patients do not possess or understand the information related to their condition and possible options, leading to feelings of disempowerment and vulnerability.11 12 The literature on implementation and effectiveness of shared decision making in hospital setting is limited. Considering that 25% of patients admitted to hospital suffer from cognitive impairment,13 it is even more important to ensure communication with their relatives and to be aware that the problem of information recall will be even more significant in this group.
Patient-centred care has been defined as care that is respectful of, and responsive to, individual patient preferences, needs and values and ensures that patient values guide all clinical decisions.14 Patient consent procedures, patient-feedback, patient representation in colleges and healthcare trusts and codesign of services are all expressions of this philosophy. Self-care programmes and their measurements are seen as crucial to realise this.15 16
The ‘What Matters To You?’ campaign is a Scottish initiative started in 2016 which aims to ‘encourage meaningful conversations between patients and healthcare providers’17: The annual report following the campaign in 2019 found that what mattered the most to patients was ‘relationships, dignity and respect and communication’.18 Prey et al conducted a systematic review of patient engagement initiatives in the USA.8 Though they did not study communication specifically, engagement and communication are closely linked. They theorised that as the complexity of the engagement technique increased, expected patient usage would decrease, suggesting that any initiatives to encourage engagement should be relatively simple. An American study on ambulatory care patients found that providing patients with a print-out of their health record improved their understanding, motivation to adhere to treatment plans and improved satisfaction.19 This implies that there is a benefit when patients have access to their health information.
Communication context in hospital
One of the problems with communication is optimising the timing and setting for effective communication. Most communication between medical teams and hospital inpatients occurs on the ward round. The structure of a medical ward round traditionally involves the medical team moving swiftly from one patient to another, reviewing the notes, examining the patient and dealing with any new problems. Ward rounds tend to be highly scripted and time constrained which results in only a few minutes being spent with each patient per day.
This study aimed to use a codesign process to create ideas for improved communication, led by patients and staff in response to identified needs of inpatients and was part of an Improvement Science Fellowship by one of the authors (CPS) sponsored by The Health Foundation which aimed to explore a more active role for patients in their own safety in hospital through the use of Personal Health Records.
Measurement
This study was undertaken at the 23-bed AMU of the Ysbyty Gwynedd. It was carried out by doctors in training and medical students from Bangor and Cardiff Universities as part of their Student Selected Component modules throughout 2019. The baseline survey (online supplemental appendix 1) was designed to evaluate the knowledge of patients and contained nine domains. It was first piloted and then completed by 30 patients in the AMU and discharge wards. This demonstrated that most patients did not know their diagnosis or the results of key investigations: 12 (40%) patients knew their diagnosis, 26 knew what tests they had during the present admission but only 5 (17%) actually knew the results of these tests, 23 knew what treatment they received. Twenty patients knew the name of the ward they were on, nine knew the name of their consultant. Twenty (67%) patients felt that communication by staff could be improved.
Supplemental material
We applied Donabedian’s20 framework as a conceptual model in designing our tools. Donabedian postulates that effective interventions need measurable structure, processes and outcomes. The lack of an information repository for patient input (structure) would lead to suboptimal transfer or information (process) and poor patient knowledge (outcome). By creating a physical structure for information transfer, we could measure transfer and recall of knowledge. The Process measure would capture patient engagement by measuring by completion of patient-held documentation (completed yes/no). The Outcome would be measured by re-call of information around four key items from the baseline survey:
Do you know your diagnosis?
Do you know what tests you have had/are going to have?
Do you know when you are expected to go home?
Do you know or have planned a follow-up after your discharge home?
Feedback was gained informally from patients and staff to guide adjustments to the interventions and to develop subsequent prototypes. Measurements of process and outcomes were collected using Plan–Do–Study–Act (PDSA) cycles.21
Design
The project relied on three assumptions:
Most patients can read and write (or have a visiting relative who would be able to read the information for them).
Patients would ask teams on ward rounds scripted questions if instructed to do so.
Doctors would be willing to complete information for patient led documentation if the format of the document was succinct.
The prototypes (table 1) were developed with the assistance of a graphic designer specialising in human-centred design. Each prototype contained questions or information in relation to the survey-items above and was intended to serve as an aide memoire to encourage questions, facilitate recall of information and support the patient’s communication with their own relatives.
Synopsis of interventions with design features and barriers to implementation
The intervention was developed in iterative steps leading to four prototypes that were subsequently tested with patients in our hospital. Semistructured interviews (online supplemental appendix 2) were conducted with patients and direct observations informed the development and refinement of the prototypes.
Supplemental material
Version 1: A5 sheet handed out to patients during ward rounds
An A5 paper sheet containing information about the four items specified above. The sheet was handed to the doctor in training undertaking the ward round (either alone or with a consultant physician). The doctor was asked to complete the sheet and hand it to the patient with a brief explanation.
Version 2: A4 booklet handed out on admission
A version 2, A4 ‘How-To-Hospital’ diary (online supplemental appendix 3) was created in order to improve ownership of information by patients. The diary was handed to patients on admission to hospital. It contained space for patients to complete information about the content of ward-rounds including their diagnosis, tests they underwent and discharge planning. The diary also contained a glossary of common imaging investigations, blood tests, the indications for the test and the usual turn-over times for results. We assumed that an active role in completion of the document would aide information recall. We anticipated that some patients would need assistance with documentation but in general it was designed to be easy to follow and used by a lay person.
Supplemental material
Version 3: A6 cards handed out after admission
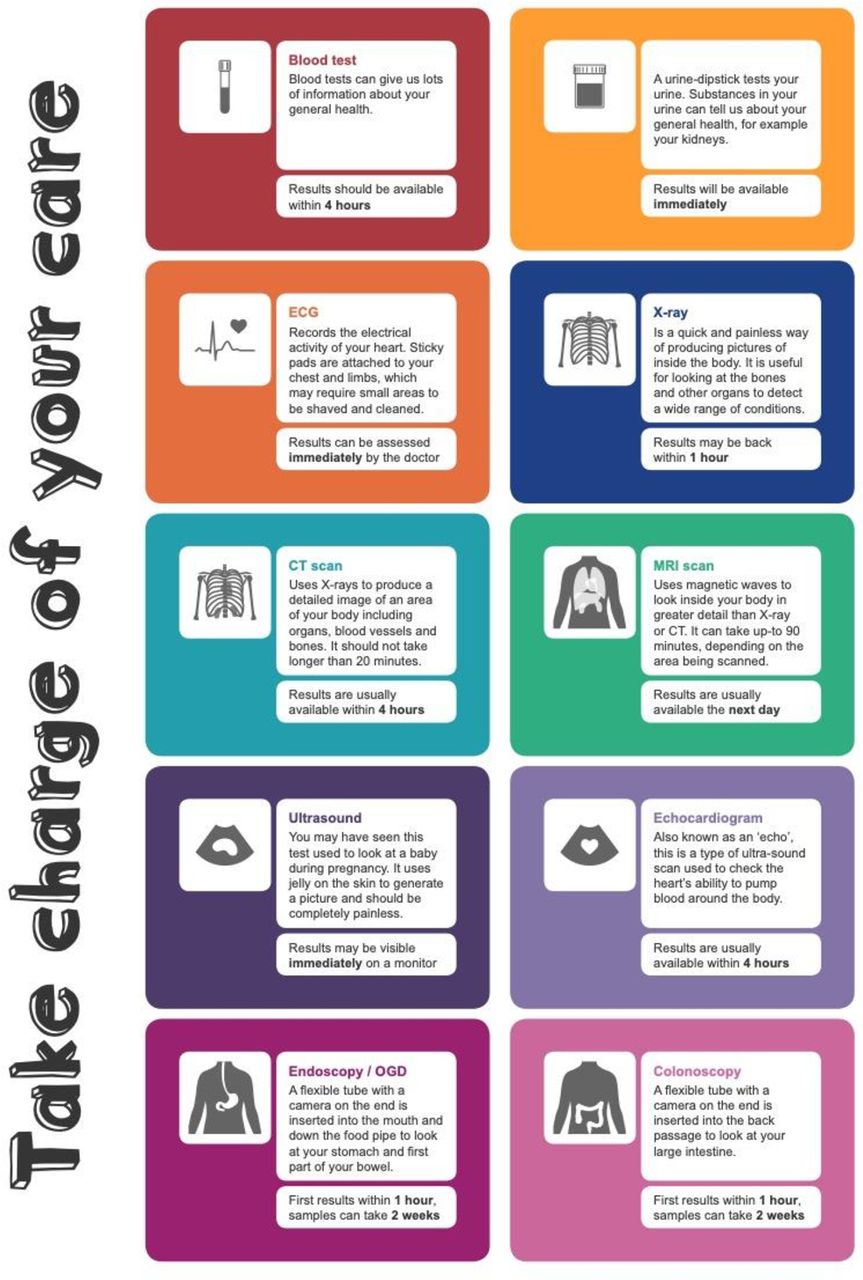
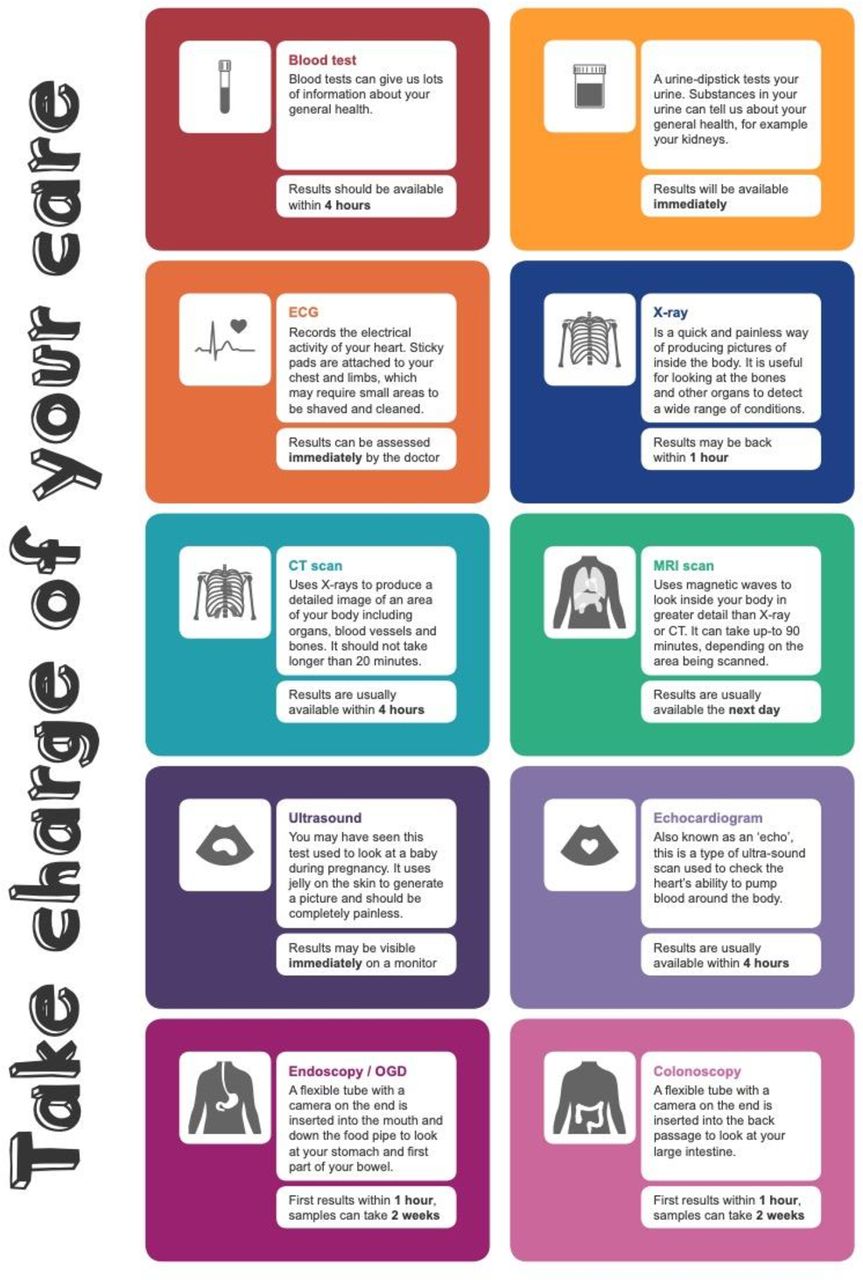
The redesigned version 3 focused on a less intimidating booklet size using an attention-provoking visual layout resulting in a ‘How-To-Hospital’ deck of diary cards (online supplemental appendix 4). The cards had a smaller format (A6) and more condensed information. Each card related to separate topics in a distinct bright colour. The selection of cards for each patient could be matched by clinicians to their pathway: diagnosis, blood tests, X-ray, etc. The patients were handed the cards on admission to hospital and were instructed about how to complete them. A wall chart with all cards was displayed in communal ward areas (figure 1).
Supplemental material
{kind=link}
The ‘How-To-Hospital’ wall chart was displayed in public areas of the ward as a reminder to patients and staff and shows the patient cards.
Version 4: A6 cards completed on ward rounds
For the last innovation cycle version 4, the medical teams were instructed to complete the relevant ‘How-To-Hospital’ diary cards during daily ward rounds. The teams were asked to minimise the use of medical jargon. We assumed that giving the patients a card with information would eliminate the patient-dependent factor while still facilitating communication and enhance information recall.
Strategy
The intervention was delivered in four PDSA cycles, with each cycle deploying a revised prototype document given to patients. In line with usual practice for the development of prototypes small samples were chosen to inform the progression of the design. Completion rates and information recall were used as surrogate measures for process and outcomes. The authors completed reflections of their observations after debriefing with the local clinical team including ward nurses, ward sisters, junior and senior doctors for each cycle.
Results
First PDSA-cycle
During the first PDSA cycle the simple questionnaire was completed by the authors and handed to a convenience sample of twenty patients during consultation at ward rounds. No formal evaluation of this cycle was undertaken. Patients were appreciative of the summary of the encounter but despite repeated encouragement to other colleagues there was no interest from other ward teams. The intervention was judged to be too dependent on the authors (SL and CPS) and alternative approaches were sought.
Second PDSA-cycle
In the second PDSA cycle, the A4 ‘How-To-Hospital’ patient-diary (online supplemental appendix 3) was introduced which contained the same data fields and additional generic information about hospital stays. Ten patients were given the diary and counselled on how to use it. The patients were encouraged to ask questions to assist their completion of the diaries. The initial feedback from patients on introducing the diaries was good, with patients commenting that it could be a helpful tool. Although patients gave positive feedback none of the ten patients completed any text in the diary. We did not anticipate that patients would not fill out the diaries as intended after instruction from a member of the medical team. Several reasons were hypothesised: Not all patients might want an active role in their care, they may have forgotten about completion, it may be that they didn’t receive enough instruction, or it may be that they didn’t feel comfortable asking the questions needed to obtain the relevant information to complete their diary.
Third PDSA-cycle
In the third PDSA cycle, the colourful A6 ‘How-To-Hospital’ diary cards were distributed to 11 patients followed by a semistructured interview (online supplemental appendix 4). Wall charts were designed and put up with a selection of the diary cards in communal areas of the ward (figure 1).
A sample of themes from the interviews is summarised in table 2: Many test results were unknown to patients and several patients expressed reluctance to ask questions about test results and diagnosis; these were also patients who mostly wanted to go home. Underlying fears and beliefs were not explored as part of the interviews. One patient stated that they did not feel comfortable asking questions during a consultation, assuming they would be told everything that was needed. Some patients stated they did not wish to know more than the doctor had shared with them.
Sample quotes from interviews with patients based on questions from online supplemental appendix 2
Patients gave feedback on the format of the diary cards: They stated that they found the diary-cards helpful and stated that they would use the cards. Patients commented that ‘undoubtedly the cards would help a lay person’, for those ‘whose second language is English’, for confused patients and if repeat testing were to be done. One patient requested more diary cards for further tests.
A patient who had been readmitted to hospital after a previous stay had a CT. The patient had used Google to find out what a CT scan was. This patient stated their intention to use the patient diary and thought that it was up to patients to ask questions to understand their illness and jargon. The patient did not complete the cards the next day due to concerns about hand writing, but thought the simpler format was appropriate. Two participants raised concerns whether patients would be expected to record their own test results.
Patients commented on the colour scheme as ‘eye catching’ and ‘engaging’ yet some called them ‘too childish’ or ‘simplistic’. Concerns of blind or colour-blind patients were raised. Test descriptions were thought to be at an appropriate level of information and patients didn’t feel they needed more. Most patients said they would use the cards, yet some didn’t find them necessary. The interviewed felt that patients should fill the diary out, to avoid medical jargon.
Ideas for improvement to be made included making the cards bigger to accommodate more information or tests results, especially for longer stays. One patient hoped the cards would be in an easier format for carrying and several patients felt a booklet type resource would be beneficial.
Fourth PDSA-cycle
The doctor completed the cards during ward rounds. Ten ward patients were selected at random (three patients per bay). Eight patients were female, and their ages ranged from 59 to 88 years (median 79). Five patients did not recall their diagnosis prior to receiving the diary cards and three did not recall the diagnosis even after receiving the cards. Seven patients knew what tests had been requested prior to the card and eight after, three patients knew their discharge date before and nine after, four understood discharge arrangements before and eight after receiving the card. The family members of patients with cognitive impairment indicated that they found the cards useful.
Lessons and limitations
We undertook a pilot study to explore the feasibility of codesigning a tool to facilitate a more active role of, and understanding by, patients during hospital ward-rounds with the specific aim to improve information recall. We designed a series of prototypes (table 1) around key information items for patients that could be completed with limited demands on time of clinicians and patients. The number of data items communicated was small thus avoiding information overload.
Our application of applying PDSA cycles with small samples is in line with usual practice when small samples are used in the development of intervention prototypes as opposed to sampling methods required for the measurement of impact during the implementation of an established intervention.
While the concept of the intervention was well received the uptake was hindered by reliance on compliance by busy medical staff in iterations 1 and 4 and poor utilisation by patients in iterations 2 and 3. Both patients and clinicians required regular reminders. The sample sizes for testing were small and timing of interventions meant that routines could not develop around a different interaction and information-flow between clinicians and patients. While we assumed that better information recall would result in better (shared) decision making we have not tested this hypothesis or indeed measured the impact on behaviours of doctors, nurses or patients. We learnt about the differences in information needs for different patients: While most patients did want to take an active role in their care, some patients did not want to have all the information about their care and preferred a more passive role. Other patients had expectations of being given just the right information and shied away from using the tools to prompt clinicians. It is important going forward that needs of these patients are recognised too.
Our interventions were cheap to produce and easy to disseminate but acknowledgement of the communication problem and ownership of a potential solution by both patients and clinicians presented an ongoing challenge: Informal discussions with colleagues found that most didn’t feel there was a significant problem and most felt their communication with patients was good. Many clinicians might not appreciate the challenges that information recall and information overload present, especially for elderly or unwell patients. The prototypes were only available in English; this might have affected uptake in the Welsh-speaking patients.
The value of patients having access to their health records has been previously explored.22–24 Studies suggest that allowing patients open access to their records improves interaction between the patient and medical team, improves communication, increases quality of care and increases patient satisfaction.25–27 This might aid in facilitating good communication and increasing patient empowerment. While patients’ ideas, concerns and expectations are a key part of patient-centred care28 few studies have investigated a coproduced format for ward rounds with the majority of the literature focusing on training of junior doctors,29 multidisciplinary teams30 and compliance of clinicians with given standards.31 Schedules for rounds with booked time-slots for patients and relatives have been suggested.32 Even when patient preferences for participation have been assessed the formats of ward rounds were not changed.33 Communication needs might be time-dependent: Basu reported that 95% of patients are only satisfied if they receive their test results within a couple of hours.34 The only comparative study we found was in a paediatric setting where a Comms-Chart was designed with play therapists and families.35
Our study touches on broader issues of ownership of information. In hospital patients are usually aware about ‘the destination of travel’ but most of them cannot ‘read the map’ and are thus not able to determine course corrections. In order for patients to drive their safety while hospitalised basic health literacy needs to be supported. The inability of patients to influence decision-making stems from lack of access to information about their care and outcomes. The persistent hierarchical gradient between patient and doctors might affect reliable usage of a tool that requires active prompting from patients36: Patients might be reluctant to ‘interrupt’ doctors to admit they did not understand information even with the background detail provided on the diary cards. Additionally, the quality of the relationship between clinicians and patients might also affect the willingness to ask questions.
Success of a new design can be measured in the way it changes the behaviours of those who interact with it. These behavioural changes depend on capability, motivation and opportunities for those involved.37 While patients had physical capability and opportunities to complete the cards, their motivation that is, beliefs might not support this model of care and social opportunities might be limited by the perceived attitudes of time-poor clinicians.
A final significant limitation of our interventions is that patients who are visually impaired or illiterate would not be able to engage with these tools. Arguably these are patient groups with whom communication is already more difficult and who would benefit the most from improved communication.
Conclusion
It is of concern how little patients might know about their condition, treatment and results of key tests. We feel that meaningful access to safety critical information will aid patients in identifying errors of commission and omission and help to empower them to raise safety concerns and report on improvement of their illness.
While our study demonstrated feasibility of a diary-card type of approach we did not reach sustainability, adoption and ‘normalisation’ of usage.
We found it was not feasible to rely on the patient alone to manage their own knowledge through use of a self-filled diary.
Further research is needed to provide guidance into whether these interventions are applicable to the wider healthcare context.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Research Ethics Committee (REC reference: 18/WA/0110; IRAS project ID:244052). The study was approved as a quality improvement project.
Acknowledgments
The authors would like to thank all the patients who contributed with their feedback to the development of the interventions and the students who collected data as part of the Student Selected Component modules, in particular Mari Davies, Buddug Eckley, Bethan Johnson, Bethan Stacey, Abby Fayen, Gwenllian Roberts, Hannah Dowell and Dr Ben Creswell who assisted with the final round of testing.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @csubbe
Contributors SL and CPS conceived the concept for this study. HT, GMJ, MD, BE, BJ and BS developed the intervention around principles of human centred design, GMJ, MD, BE, BJ and BS, GR, HRD, BC collected the data. SL, CPS, GMJ and PB undertook the primary analysis. SL, CPS and PB wrote the initial manuscript and undertook further analysis. All authors contributed to further versions of the manuscript and approved the final version. CPS acts as the guarantor of the work.
Funding CPS was funded through an Improvement Science Fellowship by The Health Foundation, London, UK (Award Reference Number: AIMS 109280).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.