Article Text

Statistics from Altmetric.com
- coproduction of healthcare
- patient care outcomes
- patient engagement
- co-creation of health
- patient activation
- self management
- healthcare partnerships
- learning health systems
Introduction
If the core aim of a healthcare system is to minimise both illness and treatment burden while reducing the costs of care delivery, then we must accept, however reluctantly, that our efforts are largely failing.
Life expectancy in highly developed countries is declining for the first time in decades. Long-term conditions and obesity are replacing infectious diseases as the most prominent health problems in developing nations. Meanwhile, average per capita healthcare expenditures are increasing despite efforts to restrain them. For example, in the USA, the average per capita healthcare expenditures are approaching $10 000 a year and consuming over 18% of its gross domestic product. Innovations in biomedicine, information technology and healthcare delivery systems may help address some of the challenges, but instead of containing costs these innovations tend to expand services.
There are indications that interest in a concept called coproduction in healthcare is increasing. The core thesis is that by leveraging professional and end user collaboration, patients can be supported to contribute more to the management of their own conditions. This is especially true when dealing with long-term conditions, where supporting the person to learn how best to reduce the burden of both illness and treatment is an undisputed good. The goal is to cocreate value. Ostrom,1 based on her seminal work as an economist, called this coproduction.
The cocreation of value already lies at the heart of most service sectors. Shopping, banking and travel all enlist the end user to coproduce value in the delivery of services. Coproduction can be even more powerful where people form alliances to share resources and generate solutions, by using what Christensen et al 2 refer to as ‘facilitated networks’. Facilitated networks offer a powerful strategy that has been adopted by many organisations to increase access, and to improve quality while lowering costs. For example, Uber and Lyft, Airbnb, eBay, and Wikipedia have rapidly changed how we travel in cities, find accommodation, sell used goods and search for information by successfully using facilitated networks to connect resources.
Healthcare service is of course more complex than a travel agency, bank or a ride share service. Health is a long-term commitment that requires specialised and nuanced expertise of clinicians and patients. The context and complexity are constantly changing: attention to short-term problems at age 20 is vastly different from dealing with dementia or with chronic obstructive pulmonary disease diagnosis in a man of 80. As options for managing illness expand, so does the role of coproduction, both at individual and population levels. The use of standardised incentives may conflict with the agreements achieved by collaboration. For example, my provider and I might decide not-so-tight control of my cholesterol is best given the low-risk factors and significant side effects. A clinician might be working in a pay-for-performance environment where statins prescribing is rewarded. Patient-centred models, such as the chronic care model,3 patient engagement,4 evidence-based self-management5 and shared decision making,6 may need to address these challenges if they are to achieve their full potential.
While it is important to note that healthcare has unique challenges that are directly attributable to the challenges of illness, it is also true that healthcare organisations have been slow to adopt coproduction principles. This is despite the work of pioneers who have proposed different patient-centred models, such as the chronic care model,3 patient engagement,4 evidence-based self-management5 and shared decision making.6
Current models of care delivery may need to invest in making these ideas central to their operation, and acknowledge that allowing services to become shaped by collaborations between patients and professionals would create greater value.7
Healthcare organisations often use the term ‘service lines’, as if they were characterised by assembly lines for standard ‘products’ such as diagnostic tests, injections, infusions and surgical procedures. It is true that some procedures can fit a ‘product’ model. The Aravind Clinic in India is a good example of a focused factory approach by doing high-volume cataract surgery at high quality and at low cost.8
However, the factory approach alone fails to provide solutions for the majority of problems in healthcare. Elderly people usually have multiple, interacting long-term healthcare problems, and, where complexity occurs, so does the need for tailored approaches. Such problems are emblematic of current population needs. It is in these situations that coproduction holds the most promise. There is increasing evidence from many settings—rheumatology,9 inflammatory bowel disease,10 kidney dialysis,11 oncology12 and primary care13—that it is possible to use coproduction principles, not only to help patients to reduce the burden of illness, treatments and costs.
Our goal in this article is to describe the potential added value of ensuring that end users are engaged in an effective process of coproduction when seeking healthcare.
The emergence of coproduction
Over the last few decades the nature of how work is completed has changed dramatically. In the 1960s, no one would put fuel in their own car. Obtaining cash would require a visit to the bank. Arranging a vacation meant working with a travel agent. As these industries realised the advantages of coproduction, investments in new technologies emerged. By combining the use of an international system of credit cards and a screen that guides payment and how to safely fill the fuel tank, the end user becomes a willing coproducer of the service. Similar combinations of screens, algorithms and user-centred devices have transformed banking, checking into flights and paying for groceries. Coproduction is more than sharing decisions or advocating that practitioners become better at patient-centred care. Coproduction processes harness the synergistic effect of user-centred design, technological innovation and human learning, and are worth the effort and investment because of the convenience and efficiency they offer to the mutual parties.
There has been no similar transformation in healthcare. Obtaining access to advice typically requires making an appointment using a person-to-person telephone call and attending a physical location, as does undertaking most tests. Prior authorisation delays care and becomes a time-sink for clinicians. Obtaining medication requires visiting yet another location. People with long-term illness such as asthma, diabetes, rheumatoid arthritis, inflammatory bowel disorders or Parkinson’s disease report that they are often left untaught about how to best manage the challenges, and they often learn more by making their own connections with others who have faced the same problems.
We want to imagine, therefore, the potential benefit of adopting coproduction principles, to increase access and provide much more efficient care, where end users learn to become more self-sufficient. While some medical problems need the diagnostic accuracy of face-to-face examination or invasive tests, there are a significant number of healthcare problems that are capable of being managed safely using communications channels such as video-conferencing. An increasing number of tests could be done by near-patient testing using samples of saliva, urine or finger-prick blood samples. With advances in online shopping, people will also expect a similar service for medication. The opportunities to engage the end user are being enhanced by new technologies, and yet systems seem resistant to adopt the potential new models of care.
Coproduction has been embraced by some patients with kidney failure who need to attend dialysis units. Some units have helped people learn how to use the dialysis machines in collaboration with the staff. By choosing to dialyse at night they can work during the day,11 and thereby increase the efficiency of the dialysis unit. The users learn from each other, provide feedback and share solutions in ways that the health professionals had not expected. In short, coproduction increased patient satisfaction and enabled cost-effective, high-quality care. Other examples of where coproduction opportunities have been realised exist in people who have cystic fibrosis,14 rheumatoid arthritis15 and inflammatory bowel disease.10 In summary, healthcare is a service poised to harness the motivation, experience and ingenuity of end users, especially when linked to the leverage given by the innovative use of technology to monitor and give feedback.
Defining coproduction
Batalden et al 16 have described the coproduction of healthcare services as ‘The interdependent work of users and professionals to design, create, develop, deliver, assess and improve the relationships and actions that contribute to the health of individuals and populations’.16
Coproduction typically relies on a process and/or technology that leverages an end user’s time, motivation and skills to add value by making a desired goal or outcome more convenient, efficient and cost-effective. In healthcare, this often involves doing activities in new settings that maximise convenience or minimise the need to travel.17 Healthcare has been slow to enhance the role of end users in monitoring their health, learning how to self-manage where possible, or seek support from facilitated networks to get the knowledge and advice of others who have faced similar challenges. Collaboration is promoted over passive patienthood, and professional recommendations are replaced by engagement, where agency is conferred using shared decision making and self-management.18
Why is coproduction a potentially better way?
Coproduction aims to generate personalised solutions that minimise both the burden of illness and the burden of treatment. Recognising this shift, the American Board of Internal Medicine19 summarised recent work in this area in a publication titled The Value of Co-Creation in Health Care. Evidence for this approach across a number of conditions is summarised in box 1.
Coproduction using patient-reported outcomes
Higher remission rates for children with inflammatory bowel disease.
A learning healthcare system where remission rates for children with inflammatory bowel disease increased from 55% to over 77% between 2007 and 2014.26
Reduced disease activity in rheumatoid arthritis.
Patients with rheumatoid arthritis had a 50% decrease in inflammatory activity using a dashboard to track and manage symptoms.15
Adult patients with cancer.
In a randomised controlled trial of patients with metastatic solid tumours, patients in the test group who reported their symptoms between visits had improved quality of life at 6 months and higher survival rates at 1 and 8 years.12
Arguments that support a shift to coproduction
Patient resilience and autonomy
Effective coproduction enables people to manage the burdens of health problems when possible, and to potentially reduce the likelihood of future problems by achieving effective control of risk factors such as high blood pressure, or high glucose levels in diabetes, or effectively managing exacerbations of inflammatory bowel disease or rheumatoid arthritis. Although these efforts to mitigate the risks of illness require time and attention, people value the control and convenience afforded, as well as the possibility of better long-term outcomes.20
Time saved
A typical person with long-term illness might spend a couple of hours every year visiting clinicians. But there are almost 9000 hours in a year, so the time people spent managing their illness far outstrips the time spent in clinics. One of the coauthors (AH) is a parent to a child with cystic fibrosis, and calculated that he works at least 2 hours a day, every day to coproduce effective care for his child. Coproduction is cost-effective and convenient for patients and their carers, and it creates enormous efficiencies to the health system at large.
Economic efficiency
The concept and term coproduction is attributed to Elinor Ostrom, a Nobel Laureate in economics. In settings such as forestry and fishing, she showed that coproduction led to lower costs because it was a more efficient way to meet social and community needs.21 Similar efficiencies are reported when coproduction is implemented in healthcare settings such as serious illness,20 palliative care,22 mental health,23 rheumatology24 and primary care.25 Efficiency is particularly true where patients learn to self-manage complex processes such as dialysis (box 2), and for example parents who learnt how to do intravenous therapy at home for infection in cystic fibrosis saved an estimated 2000 hospital days per year at the Karolinska Institute (Andreas Hagar, 2018, personal communication).
Coproduction in rheumatology and renal dialysis in Sweden
Case 1: Rheumatology Quality Register.
Patients with rheumatoid arthritis and their clinicians have used ‘coproduction dashboards’ since 2004 to display data that patients report about their symptoms and outcomes.
The number of patients with high rheumatoid activity has been reduced by approximately 50% between 2004 and 2014. The blue line in figure 3 represents disease activity trend in Gävle County, Sweden. The vertical line indicates when all rheumatologists in Gävle County used the coproduction dashboards, and demonstrates a clear additional improvement.24
Case 2: Renal Dialysis Clinic at Ryhov Hospital, Jönköping.
A patient asked his renal dialysis nurse to teach him how to manage his own treatment in 2005. Since then, the patient and the dialysis nurse have taught many patients to do the same. Nearly 60% of the clinic’s patients are self-dialysing, with fewer side effects, greater satisfaction and lower costs.11 By thinking of patients as resources rather than as passive customers, the clinical team were able to achieve better results, despite the need to teach and learn how to safely use sophisticated medical devices.

Disease activity based on C reactive protein (CRP) levels in Sweden and in Gävle County, 2004–2014.
How might coproduction be part of mainstream healthcare?
What is different in a coproduction approach?
A coproduction cycle
In a traditional approach to long-term conditions, assessment and diagnosis lead to unilateral recommendations. The patient is then asked to monitor whether the treatment is effective. Follow-up adjustments are done as needed by the clinician. This approach can often be successful, but there is a well-known risk that unilateral recommendations may not align well with individual priorities, preferences or constraints, and so problems occur.
Coproduction is different because it involves a collaborative process (see figure 1), where an individual’s goals help determine the plan, as well as professionally set targets, guidelines or clinical recommendations. What might appear to be a subtle shift of power can lead to a profound difference in roles and approach. The clinician and patient work together to coassess the patient’s situation, paying attention to the impact of illness on the patient’s life and well-being. Critical, to codeciding the best treatment is based on an explicit discussion of the patient’s goals regarding symptoms, function and other priorities, such as key milestones in life. The third step, codesigning the care plan, takes other contextual factors into account, and critically considers how the patient and their families could contribute. In this design process, a number of different capabilities to codeliver the care will be considered and leveraged.

Coproduction cycle: cooperation for optimal care.
Role shifts
Coproduction demands new work from everyone: it relies on patients sharing their concerns and goals, participating in decisions, and in many situations learning to manage long-term conditions. Clinicians need to become curious about patients’ goals and work collaboratively to codecide and codesign care, so that care can be codelivered. These new roles require new skills and often significant attitude changes.
Learning health systems
Coproduction often occurs when a motivated clinical champion takes the initiative. However, spread across teams and systems requires leadership and change at system levels, and the development of what is becoming known as a learning health system.26 Indeed, progress in achieving patient-centred care in front-line clinical practice has been painfully slow since the 1970s. It could be argued that the real contribution of the coproduction principles and methods is the realisation that change will require simultaneous and synergistic developmental work at policy, organisational, as well as microsystem and interpersonal levels.
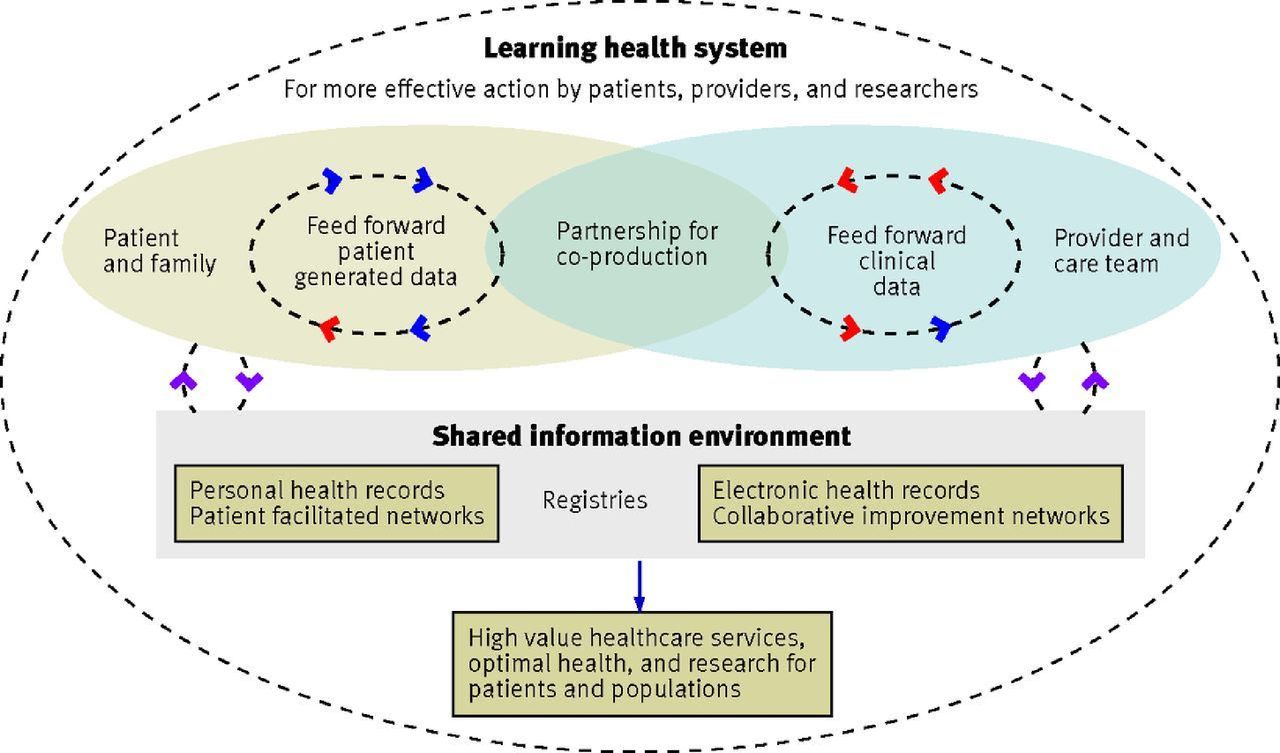
Learning health systems use change management methods to measure and improve performance, where patient-reported measures and clinical outcomes are made visible to clinicians and others (see figures 2 and 3). By ensuring that data from both medical evaluations as well as patient-reported outcome and experience measures become inputs into shared decisions, a different kind of collaboration is forged. Enhancing these data flows by setting up measurement systems and dashboards has led to significant improvements in the care of rheumatoid arthritis and inflammatory bowel disease (see box 1). Harnessing such information in registries and research databases reinforces quality improvement cycles.
{kind=link}
{kind=link}
{kind=link}
Learning health system (adapted from Nelson et al 15).
Conclusion
The interest in coproduction is increasing at an international level, with two hubs based in Jönköping and Dartmouth now supporting multiple communities of practice.27 It is true that current financial incentives often focus on the achievement of biomedical proxies that might not be the highest priorities for patients. If incentives could be better aligned, the coproduction concept has the potential to bring together many patient-centred ideas by connecting shared decision making to the use of feedback dashboards and patient registries. Coproduction also makes a connection between practice improvement and organisational design by leveraging the power of learning health systems towards the increasing focus on value-based care.28 The concept, in other words, connects powerful ideas and stands a good chance of delivering a better healthcare service.
Acknowledgments
We wish to acknowledge the revisions suggested by Frank Davidoff, MD, as well as the contributions made by Paul Batalden, MD, and Elliott Fisher, MD, MPH.
References
Footnotes
Contributors EN and GE initiated the article, and were joined by AH and AP to develop the arguments. Each author contributed to drafts and has agreed on the final manuscript. GE acts as guarantor for the article.
Funding This work was supported in part by grants from the Robert Wood Johnson Foundation (grant numbers 71211, 72313), the Cystic Fibrosis Foundation (grant number OCONNO04Q10), the Crohn’s and Colitis Foundation of America Quality of Care Initiative (grant Number 3372), and the Health Assessment Lab/Medical Outcomes Trust.
Competing interests GE has edited and published books that provide royalties on sales by the publishers: the books include Shared Decision Making (Oxford University Press) and Groups (Radcliffe Press). He has in the past provided consultancy for (1) Emmi Solutions, which develops patient decision support tools; (2) National Quality Forum on the certification of decision support tools; (3) Washington State Health Department on the certification of decision support tools; and (4) SciMentum, Amsterdam (workshops for shared decision making). He is the Director of &think, which owns the registered trademark for Option Grids patient decision aids. He provides consultancy in the domain of shared decision making and patient decision aids to (1) Access Community Health Network, Chicago (Federally Qualified Medical Centers), and to (2) EBSCO Health Option Grids patient decision aids. GE initiated the Option Grid Collaborative, tools that are hosted on a website managed by Dartmouth College, on http://optiongrid.org/. Existing Option Grids hosted on this website are freely available until such time as the tools have expired. He owns copyright on measures of shared decision making and care integration, namely collaboRATE, integRATE and Observer OPTION. These measures are freely available for use. EN holds stock in a quality measurement company (Quality Data Management). AP is the patient editor for research and evaluation at The BMJ. No other conflicts to report.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note AH is a father of a patient who has cystic fibrosis and lawyer in Sweden who has dedicated the last 17 years of his career to the development of coproduction systems, starting in the legal industry and since 2008 shifting to work within chronic care collaboratives. AP is the patient editor (research and evaluation) at The BMJ, a doctoral student at the University of Oxford and a patient with long-term medical conditions. EN has expertise in patient registries, clinical collaboratives and quality improvement. GE is a clinician-researcher who has developed a focus on shared decision making in the context of supporting a model of coproduced care.