Article Text

Statistics from Altmetric.com
Postpyloric (or jejunal) feeding may be required in children where feeding via gastrostomy is associated with problems of severe gastro-oesophageal reflux leading to faltering growth.1 2
A 2-year-old boy presented with what appeared to be a standard complication of tube blockage, having previously been fed through a 6-French jejunal (J) extension via a 16-French Corflo PEG (PEGJ). Gastric feeds were commenced during the suspected J tube blockage, and removal of the J tube was attempted. However, as the J tube could not be withdrawn, gastroscopy was performed to explore this further and have his PEG switched to a balloon gastrostomy.
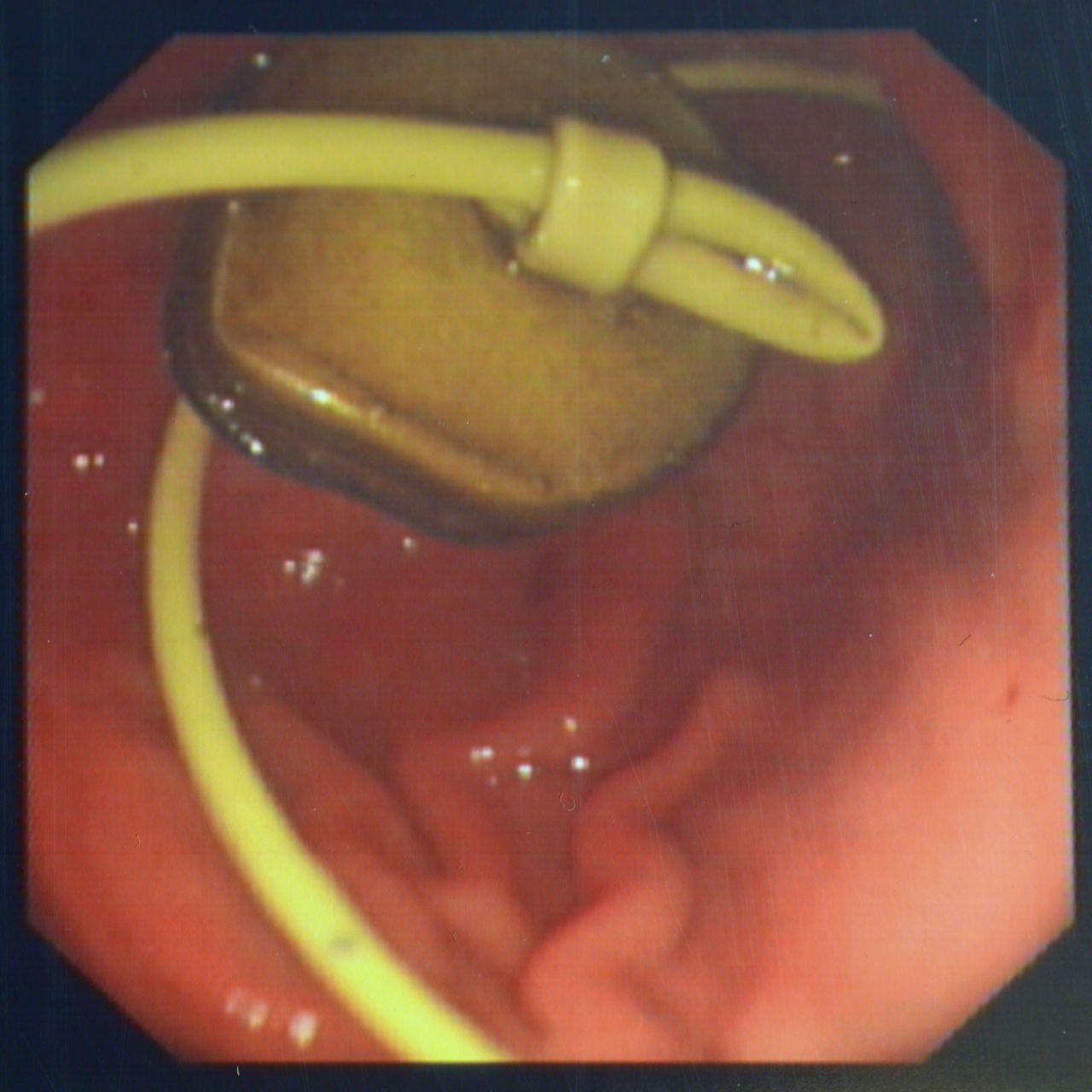
During endoscopy, a true knot was identified in the J tube (figure 1). The J tube was cut and then snared, enabling a standard conversion to balloon gastrostomy to be performed.
{kind=link}
Endoscopy image of knot in jejunal tube.
Tube blockage and displacement are the most common associated problems of postpyloric feeding,3 but in this boy’s case, both occurred simultaneously due to a true knot forming in the J tube.
Alternative approaches to the use of a PEGJ tube are direct J tube placement via deep enteroscopy or combined laparoscopy/enteroscopy. Although this prevents the problem of displacement and reduces the risk of blockage (as a 12 to 15-French device can be inserted), the procedure is more invasive and associated with volvulus and internal herniation.4
Footnotes
Contributors MR wrote the first draft of the piece. DC performed the procedure, took the image displayed and edited the piece.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Provenance and peer review Not commissioned; externally peer reviewed.