Article Text

Abstract
Purpose: Physicians are often reluctant to discuss “Do Not Resuscitate” (DNR) orders with patients. Although perceived self-efficacy (confidence) is a known prerequisite for behavioural change, little is understood about the confidence of physicians regarding DNR discussions.
Subjects and methods: A survey of 217 internal medicine attendings and 132 housestaff at two teaching hospitals about their attitudes and confidence regarding DNR discussions.
Results: Participants were significantly less confident about their ability to discuss DNR orders than to discuss consent for medical procedures (p<0.001), and this was true for both attendings (p = 0.002) and housestaff (p<0.001). In a multivariate logistic model of confidence regarding DNR discussions, women were less confident than men (OR = 0.52, CI = 0.29 to 0.92); house officers were less confident than attendings (OR = 0.35, CI = 0.20 to 0.61), those who were less confident of their ability to discuss medical procedures were less confident discussing DNR (OR = 0.12, CI = 0.06 to 0.25), and those who found talking to patients about DNR orders very difficult reported less confidence than those who did not (OR = 0.06, CI = 0.02 to 0.16).
Conclusion: We conclude that physicians’ confidence regarding DNR discussions is low compared with their confidence regarding other medical discussions and that confidence varies by sex and perceived difficulty of the task. Efforts to improve DNR discussions should explore the need to tailor educational interventions to fit these characteristics.
- Ethics
- house officers
- confidence
- communication
- do not resuscitate
Statistics from Altmetric.com
Among seriously ill patients who are unlikely to survive resuscitation, Do Not Resuscitate (DNR) orders are surprisingly infrequent.1–5 Yet it remains uncertain why this is so. Barriers to end-of-life discussions have been identified among patients, families, health care professionals, and health care systems.6 It has been speculated that physicians might avoid end-of-life discussions because they lack knowledge about advance directive laws, lack training on how to deliver bad news, fear causing the pain of bearing bad news, view death as an enemy to be defeated, anticipate disagreement with the patient or family, have medical-legal concerns, or feel threatened by such discussions.7
Experts have called for the overcoming of these barriers and for more effective discussions about DNR orders.5 8 9 However, changes in physician behaviour take time and are related to numerous factors. Psychological research has shown that one prerequisite to behavioural change is perceived self-efficacy or “confidence”.10 11 The purpose of this project was to explore physicians’ perceptions of DNR order discussions with patients and surrogates and to determine the factors associated with their degree of confidence in engaging in these discussions.
STUDY METHODS
Sample
The study was conducted in 2002 at two private teaching hospitals, St. Vincent’s Hospital Manhattan and St. Vincent’s Hospital Staten Island, both members of Saint Vincent’s Catholic Medical Centers of New York, USA. At both sites, we surveyed attending internists (identified from rosters of medical staff physicians) and medical house officers. Anonymous surveys were distributed to 194 Manhattan attendings, 178 Staten Island attendings, 104 Manhattan house officers and 52 Staten Island house officers. Attending physicians were surveyed via mailings and distributions at subspecialty section meetings and individual offices. House officers were surveyed by a researcher who distributed the surveys at each site. From both sites combined, 349 participants returned surveys: 217 attending physicians and 132 house officers. The overall response rate was 58% for attending physicians and 85% for house officers. The Institutional Review Boards at both St. Vincent’s Hospital Manhattan and St. Vincent’s Hospital Staten Island approved the study.
Instrument
Content of the questionnaire was developed by interviewing experts in pain management, survey research, and medical education. Our questions about confidence were based upon Bandura’s well-established social learning theory,10 11 used extensively in the literature about medical education and patient behavioural change.12–15 We then used cognitive pre-testing16 17 to validate and revise the survey items further by presenting them to physicians at Westchester Medical Center, New York, USA (attending general internists, chief residents and a cardiologist) and to nurses at New York University, New York, USA (nursing faculty and nursing graduate students).
Four items constitute the main dependent variables in this study:
I feel confident in my ability to talk with patients or their surrogates about consent for medical procedures about which I am knowledgeable;
I feel confident in my ability to talk with patients or their surrogates about DNR orders;
I find talking to patients about DNR orders difficult;
When patients cannot speak for themselves, I find talking to patients’ surrogates about DNR orders difficult.
Each of these items was scored on a 5-point Likert scale: “agree strongly,” “agree somewhat,” “neither agree nor disagree”, “disagree somewhat,” or “disagree strongly.”
Demographic information collected on participants included: primary practice location (Manhattan or Staten Island), professional status (attending or house officer), year of medical school graduation, practice specialty (if an attending physician), number of DNR patients cared for in last month, age, sex, race/ethnicity, country of birth, country of medical school, religion, and frequency of attendance at religious services.
Analysis
Comparisons of the sociodemographic characteristics of attending physicians and house officers were performed using t tests or χ2 tests, as appropriate. Comparisons between the responses of attendings and house officers regarding the four main outcome variables (such as attending physician confidence vs house officer confidence) were performed using the Mann-Whitney U test. Paired data (such as a comparison of participants’ confidence in discussing DNR and their confidence in discussing medical procedures) were performed using the marginal homogeneity test, an extension of the McNemar test.18 Spearman’s ρ was calculated to assess intercorrelations between the four main dependent variables.
Initial tests of univariate association between independent variables and confidence talking with patients and surrogates about DNR orders were conducted using the data from the complete, 5-point, undichotomised scale by means of the appropriate non-parametric tests (Spearman’s ρ, Mann-Whitney U, or Kruskall-Wallis). Because responses to participants’ confidence in talking with patients and surrogates about DNR orders were highly skewed, multivariate analyses were conducted by dichotomising the dependent variables to enable the creation of logistic regression models. Confidence discussing procedures and confidence discussing DNR orders were dichotomised into “agree strongly” (high confidence) versus all other responses. Difficulty talking with patients about DNR and difficulty talking with surrogates about DNR were dichotomised into “disagree strongly” versus all other responses. Univariate analysis of associations between sociodemographic data and these four dichotomised items were then conducted. For the sole continuous variable (age), t tests were run. χ2 Tests were run for all other variables (attending physician or house officer, gender, race/ethnicity, practice specialty, religion, frequency of religious services, number of DNR patients cared for in the past month, country of birth and medical training, and research site).
A multivariate logistic regression model was then developed for the item about participants’ confidence in talking with patients and surrogates about DNR orders. All variables found to be significantly associated with this dependent variable in the univariate analyses were tested as independent variables and then dropped in backwards, stepwise fashion if they did not contribute significantly to the multivariate model. Because they were imbalanced between the two sites, race and religion were tested even though not significantly associated with confidence in univariate analysis. In particular, the number of Asian physicians was higher in Staten Island and since we hypothesised that this might be associated with cultural barriers to DNR discussions, we tested for race, dichotomised as Asian versus other, in the model. To test the robustness of our findings, the model was then re-estimated using the same independent variables, but using the dependent variable of confidence in discussing DNR orders dichotomised in an alternate way—“agree strongly” or “agree” versus all other responses.
The statistical software SPSS V.13 was used for all computations.19
RESULTS
Table 1 displays the demographic characteristics of all participants. Most participants identified themselves as being born and/or trained in the United States (71%), male (68%), white (57%), in General Medicine or Geriatrics (56%), and as having cared for between one and five DNR patients in the past month (53%). While 84% reported a religious affiliation, only 23% reported attending religious services weekly or more often. attending physicians and house officers differed significantly in their demographic characteristics. The mean age of attending physicians was higher than house officers (47 vs 30 years, p<0.001) and more attending physicians were men (77% vs 53%, p<0.001). Participating attendings did not differ from the eligible attending pool in sex (p = 0.69) or age (p = 0.38). Participating house officers did not differ from the eligible house officer pool in sex (p = 0.85) or age (p = 0.98).
Confidence
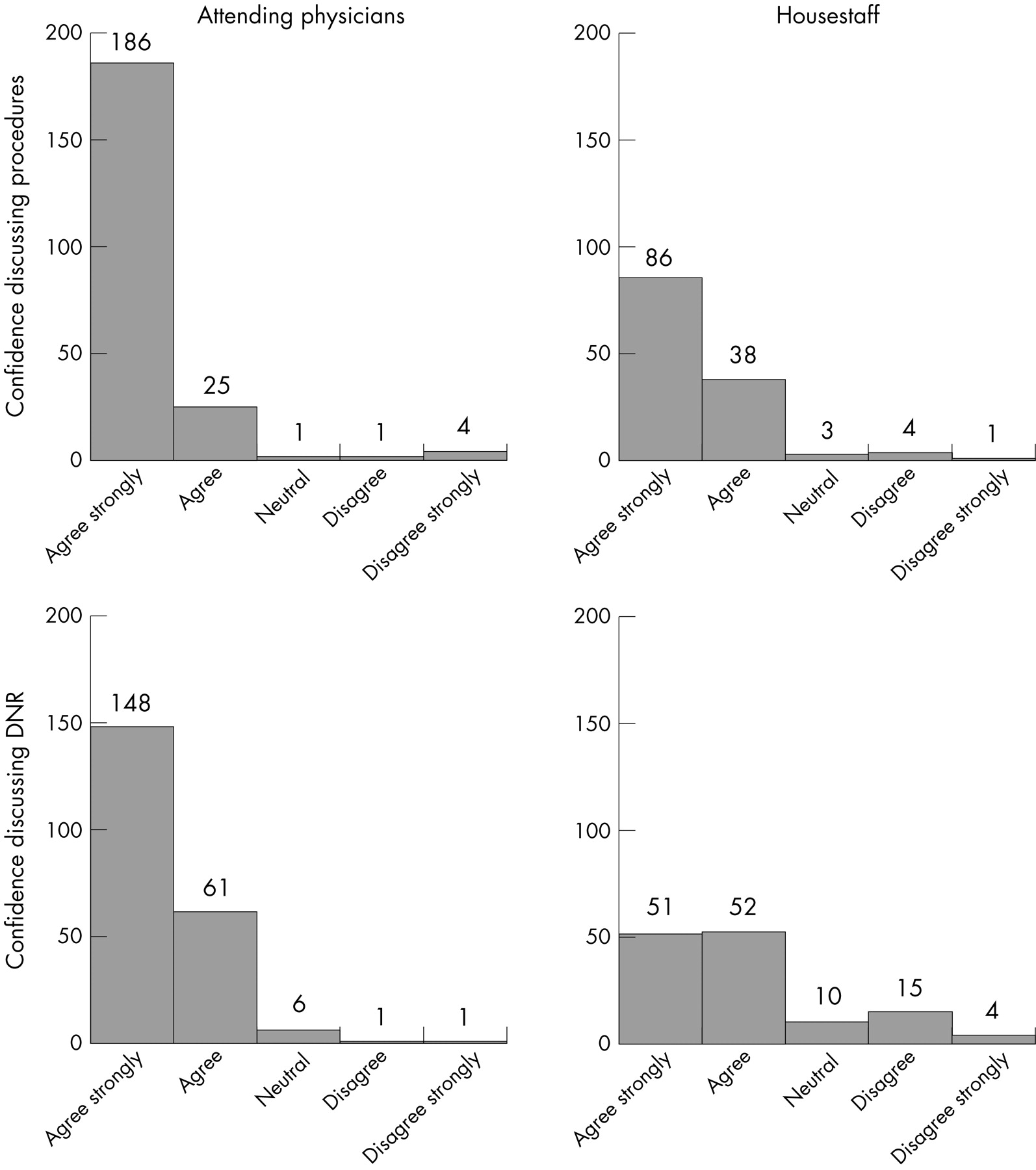
Of all respondents, 78% agreed strongly that they were confident discussing consent for routine medical procedures, while substantially fewer (57%) agreed strongly that they were confident in talking to patients or their surrogates about DNR orders (p<0.001, marginal homogeneity test). This difference in confidence discussing procedures compared with confidence discussing DNR orders persisted in subgroup analyses of attending physicians (p = 0.002) as well as house officers (p<0.001).
Figure 1 displays how attendings and house officers responded to the two measurements of confidence in talking with patients and surrogates about consent for procedures and for DNR orders. There were marked differences between the responses with respect to the confidence questions. Fewer house officers (65%) than attending physicians (86%) agreed strongly that they were confident discussing medical procedures (p<0.001). The difference between the groups in their confidence discussing DNR orders was even greater, with 68% of attending physicians choosing “agree strongly” compared with only 39% of the house officers (p<0.001).

{kind=link}
Difficulty
A plurality of participants reported at least some difficulty discussing DNR orders. On a 5-point scale from 1 (“agree strongly”) to 5 (“disagree strongly”), the mean response for attending physicians was 3.49 for talking to patients and 3.35 for talking to surrogates. The mean response for house officers was 3.06 for difficulty in talking to patients and 2.93 for talking to surrogates. Even among attendings, 31% either agreed strongly or agreed that they had difficulty talking to patients about DNR orders. Only 22% of overall respondents disagreed strongly that they had difficulty talking to patients about DNR orders and only 18% disagreed strongly that they had difficulty talking to surrogates. We found a significant difference in the response patterns — physicians in general found talking to surrogates more difficult than talking directly to the patients (p = 0.02, marginal homogeneity test).
Univariate associations
We explored the associations between participants’ sociodemographic characteristics and attitudes and participants’ confidence in consent conversations with patients and surrogates. The results of the univariate analyses of the dichotomised outcome variables regarding confidence in discussing DNR orders are shown in table 2.
Confidence discussing DNR orders was lower for house officers (p<0.01), for women (p<0.01) and for those who were younger (p<0.01). Confidence discussing DNR orders was also lower for those who reported more difficulty discussing DNR orders with patients (p<0.001), and those who reported more difficulty discussing DNR orders with surrogates (p<0.001). Confidence discussing consent for DNR orders was highly associated with confidence discussing consent for medical procedures (ρ = 0.45, p<0.001). Race (Asian vs non-Asian as well as White vs Asian vs Other), country of origin, and whether the individual reported a religious preference were not significantly associated with confidence discussing DNR orders.
Analysis of these univariate associations by the non-parametric techniques of Spearman’s ρ, Mann-Whitney U, or Kruskall-Wallis, as appropriate, using the data in the form of complete 5-point, un-dichotomised scales, yielded results completely consistent with those obtained on the dichotomised data.
Multivariate model for confidence discussing DNR orders
We estimated a logistic regression model for confidence discussing DNR orders. The final model is shown in table 3. Those who were less confident in discussing procedures were less confident in discussing DNR orders, women were less confident than men, and house officers were less confident than attendings. Those who reported greater difficulty talking with patients about DNR orders reported less confidence than those who reported little difficulty. Neither age, difficulty in talking to surrogates about DNR orders, race, nor religion was significantly associated with confidence regarding DNR discussions in multivariate analysis and these were dropped from the final model. Because older physicians are much more likely to be men, we tested for an age-sex interaction. No such interaction was evident. To test the robustness of these findings, we also ran the model with the dependent variable of confidence dichotomised as “agree strongly” or “agree” versus all other responses and found similar results.
DISCUSSION
Even among patients with poor prognoses1 2 20 21 and among patients who would not want to be resuscitated,22 23 rates of DNR discussions by physicians are consistently low, and experts have called for interventions to improve this situation.5 8 9 According to Bandura’s well-established model of behavioural change, successful performance requires both knowledge and self-efficacy or confidence.10 11 Physicians’ relative lack of confidence appears to be one important factor that may contribute to these low rates of DNR discussions. If this is so, rates of DNR discussion will not improve unless physicians’ confidence in their ability to conduct these discussions can be improved.
Our findings show that physicians are significantly less confident about their ability to discuss DNR orders with patients and their surrogates than they are in discussing more “routine” matters such as consent for medical procedures. We also found that physicians’ confidence in discussing DNR orders varies systematically with sociodemographic and other characteristics of these physicians. House officers were less confident than attendings, women were less confident than men, those who were less confident of their ability to discuss DNR orders reported greater difficulty talking to patients about DNR orders, and those who reported lower confidence in their ability to obtain consent for routine procedures were less confident in discussing DNR orders.
The implications of these findings for the development of interventions to improve physician discussions of DNR orders are complex. Mavis’ study of medical student performance on an ethics Objective Structured Clinical Examination demonstrates the intricacies of the relationship between performance, knowledge, and self-efficacy.24 According to the causal model developed by Mavis, performance is the product of complex relationships between clinical skills and biomedical knowledge, mediated by perceptions of confidence, preparedness, and anxiety. This suggests that while confidence is necessary, it will be important to address multiple factors in order to improve physician practices regarding DNR orders.
That women are less confident than men in discussing DNR orders may be due to gender-specific differences in learning styles or to socialisation factors in society at large or within the medical profession.25 Of interest, this sex difference in confidence was limited to DNR discussions and was not seen in confidence discussing procedures. By understanding differences between men and women in their learning styles, communication skills, and views of death and dying, interventions that address these sex differences could be developed.
That confidence in discussing consent for medical procedures is associated with confidence regarding DNR discussions may represent a more general “halo effect”. Both of these tasks involve communication skills. In addition, those who lack confidence may simply lack confidence globally. These results suggest that to improve DNR discussions, different approaches may be useful for different groups of physician-learners. Those reporting globally low levels of confidence, those who lack confidence only with respect to DNR discussions, and those who are who are already confident of their ability to carry out DNR discussions may have very different learning needs that could only be ascertained through formal needs assessment.
Attendings were more confident than house officers. This unsurprising finding probably reflects the complexity of the skills required to conduct these discussions well, especially the ability to attend to the emotional needs of patients and surrogates.26 No cognitive educational intervention will substitute for the necessary life experience and maturity, but this does not imply that knowledge is unnecessary (even if not sufficient) for carrying out such discussions well, nor does it suggest that education cannot help to nurture latent skills or provide useful techniques.
Limitations
These findings should be interpreted in light of the study limitations. First, all data are self-reported, and participants may not be accurate in their recollections or self-assessments. However, since our main findings are comparative, any such inaccuracies should cancel out of both the numerator and the denominator. Second, because this is a cross-sectional study, causal inferences can only be speculative. Third, the response rate of attendings was much lower than that of house officers and might be a source of bias. However, participating attendings did not differ from the eligible attending physician pool in age or sex, and our response rate of 58% exceeded the mean response rate of 54% for mailed surveys of physicians in the published literature.27 Fourth, the study was conducted in only two teaching hospitals, both Catholic, in a single US city and the results may not be generalisable. However, the study does have strength in that the two hospitals are located in different counties and in the fact that that one provides tertiary care while the other is a community hospital. Fifth, the quantitative data we present can only capture one aspect of a very complex problem and the findings could be amplified by qualitative research. Low confidence and perceived difficulty talking about DNR orders are certainly only parts of this complex problem, and it cannot be guaranteed that efforts to improve confidence and decrease perceived difficulties will improve DNR discussions.
Implications
While DNR orders have been a standard part of clinical practice for over 25 years, significant problems remain in implementing them.28 29 The general need for improved education and training about care at the end of life, including communication skills, is well established.30–33 The current study makes clear that the needs of attending physicians may be almost as great as those of trainees, with 31% attendings “somewhat” or “strongly” agreeing that DNR discussions are difficult. Since confidence is lower for women and those with self-reported difficulties talking about DNR orders, future research about educational interventions to improve DNR discussions might fruitfully pursue practical, experiential learning techniques and might be tailored to meet the different learning needs of men and women.
Acknowledgments
We would like to thank Ruth McCauley, RN, PhD and Charentas Toochinda, MD for assistance with data collection and data entry. We are very grateful to M. Kai He for her assistance with manuscript preparation. Finally, we thank the Greenwall Foundation for their generous grant support that made this project possible.
REFERENCES
Footnotes
Funding: This study was funded by a grant from the Greenwall Foundation.
Competing interests: None declared.
Other content recommended for you
- Honouring patient's resuscitation wishes: a multiphased effort to improve identification and documentation
- End of life decisions: attitudes of Finnish physicians
- The do-not-resuscitate order: associations with advance directives, physician specialty and documentation of discussion 15 years after the Patient Self-Determination Act
- Evaluation of end of life care in cancer patients at a teaching hospital in Japan
- Do Not Resuscitate orders and ethical decisions in a neonatal intensive care unit in a Muslim community
- Scale of levels of care versus DNR orders
- The attitudes of neonatal professionals towards end-of-life decision-making for dying infants in Taiwan
- Increasing use of DNR orders in the elderly worldwide: whose choice is it?
- Should patient consent be required to write a do not resuscitate order?
- “Allow natural death” versus “do not resuscitate”: three words that can change a life