Article Text

Abstract
Objective: To describe magnetic resonance imaging (MRI) findings in the lumbar spine in asymptomatic elite adolescent tennis players, to serve as the baseline for a future prospective longitudinal cohort study.
Design: Observational study.
Setting: Institutional, national tennis centre.
Participants: 33 asymptomatic elite adolescent tennis players, mean (SD) age, 17.3 (1.7) years (18 male, 15 female).
Methods: Sagittal T1, T2, STIR, and axial T2 weighted MRI images were reviewed for the presence of abnormalities by two radiologists in consensus. Abnormalities included disc degeneration, disc herniation, pars lesions (fracture or stress reaction), and facet joint arthropathy.
Results: Five players (15.2%) had a normal MRI examination and 28 (84.8%) had an abnormal examination. Nine players showed pars lesions (10 lesions; one at two levels) predominately at the L5 level (9/10, L5; 1/10, L4). Three of the 10 lesions were complete fractures; two showed grade 1 and one grade 2 spondylolisthesis, both of which resulted in moderate narrowing of the L5 exit foramen. There were two acute and five chronic stress reactions of the pars. Twenty three patients showed signs of early facet arthropathy occurring at L5/S1 (15/29 joints) and L4/5 (12/29 joints). These were classified as mild degeneration (20/29) and moderate degeneration (9/29), with 20/29 showing sclerosis and 24/29 showing hypertrophy of the facet joint. Synovial cysts were identified in 14 of the 29 joints. Thirteen players showed disc desiccation and disc bulging (mild in 13; moderate in two) most often at L4/5 and L5/S1 levels (12 of 15 discs).
Conclusions: Abnormalities were frequent, predominately in the lower lumbar spine, almost exclusively at L4/5 and L5/S1 levels. Pars injuries and facet joint arthroses were relatively common.
- MRI
- lumbar spine
- tennis player
- facet joint arthropathy
- spondylolysis
- lumbar synovial cyst
Statistics from Altmetric.com
In tennis there is a strong association between junior career performance, early transition to professional status, and success as a professional player. Young tennis athletes spend increasing time training and playing during adolescence. Such repetitive, strenuous, and intense training during the growth spurt is thought to play a role in the increased incidence of injury and musculoskeletal morbidity.1–4
In tennis, trunk injuries are the third most common type of injury after those to the lower and upper limb.5 Few studies have looked at the risk factors predisposing to these injuries5 and hence little is known about what preventive measures to take. There are no prevalence studies looking at radiological abnormalities of the lumbar spine in the asymptomatic or symptomatic elite tennis players of any age.
This study describes the prevalence and nature of these findings using magnetic resonance imaging (MRI) in an asymptomatic group of young elite tennis players. This initial observational study will form the baseline for a prospective longitudinal cohort study with the aim of following the natural progression of radiological changes, identifying radiological risk factors for morbidity, and determining the possibility of prehabilitation.
METHODS
The study was a part of a surveillance programme undertaken with funding from the Lawn Tennis Association and was approved by internal review by the medical ethics committee. Age appropriate informed consent was obtained from each patient or parent before participation.
Thirty three young elite tennis players (18 male, 15 female, mean (SD) age, 17.3 (1.7) years, range 16 to 23), without a history of back pain were recruited from a national tennis centre undergoing an accredited performance programme.
Imaging technique
Imaging was carried out in a 1.5 Tesla scanner (Symphony, Siemens) using sagittal T1 weighted (W) fast spin echo (FSE) sagittal and axial T2W FSE and sagittal short tau inversion recovery (STIR) images.
Sagittal images were obtained from the lower thoracic vertebrae down to and including whole of the sacrum. An axial block of images was obtained from the L1/L2 through to the L5/S1 intervertebral discs.
Imaging parameters used were as follows: sagittal T1W FSE: time of echo (TE) = 13, time of repetition (TR) = 614; sagittal T2W FSE: TE = 106, TR = 3300; axial T2W FSE: TE = 121, TR = 4700; sagittal STIR: TE = 65, TR = 3310, inversion recovery (IR) = 150. The slice thickness was 4.5 mm with a 0.5 mm interslice gap.
Image assessment
Two musculoskeletal radiologists, in consensus, reviewed all images. Each scan was assessed for the presence, location, and degree of facet joint arthropathy, disc degeneration, Modic changes, disc herniation, pars injury, and the presence synovial cysts. The presence and location of other disease was also recorded, including high intensity zones, degenerative conditions (such as Scheuermann’s disease), and apophyseal injuries.
Facet joint degeneration was classified using a system proposed by Weishaupt et al6 as normal, mild, moderate, or severe. Additionally, we noted the presence of ligamentum flavum thickening (defined as >1 mm) in these subjects.
Synovial cysts were defined as rounded, fluid containing lesions related to the facet joint and located in the epidural, foraminal, or paravertebral (adjacent to paravertebral muscles) positions. These returned variable signal intensities on T1W and T2W images (because of synovial, haemorrhagic, or proteinaceous fluid or calcification), although the majority appeared hypointense on T1 and hyperintense on T2.
Disc degeneration was classified using a modified version of a system developed by Pfirrmann et al7 as: normal (grade 0), mild (grade 1), moderate (grade 2), or severe (grade 3). Modic end plate changes were recorded if present as type 1 to 3.8
Disc herniations were classified according to the Combined Task Forces of the North American Spine Society, American Society of Spine Radiology, and American Society of Neuroradiology on nomenclature and classification of lumbar disc pathology. Peripheral disc herniations were classified as focal or broad based and protruded, extruded, or sequestered. The severity of disc herniation was classified as mild, moderate, or severe. Intervertebral disc herniations, such as Schmorl’s nodes and limbus vertebrae, were also recorded.9
Pars injuries were classified by a system developed by Hollenberg et al10 as: normal; chronic stress reaction; subtotal stress reaction; acute stress fracture; or chronic stress fracture. The degree of spondylolisthesis was classified according to a technique described by Myerding et al11 as grade 1–5.
A full classification of these systems is shown in the Appendix (available online as supplementary material at http://bjsm.bmj.com/supplemental).
Statistical analysis
Confidence intervals (CI) were calculated using an exact method assuming a binomial distribution.
RESULTS
Five of the players (5/33, 15.2%; 95% CI, 5.1% to 31.9%) showed no abnormality on MRI; 28/33 (84.8%, 95% CI, 68.1% to 94.9%) showed at least one abnormality, which included facet degeneration, synovial cysts, disc degeneration, disc herniation, and pars injury.
Facet joint arthropathy
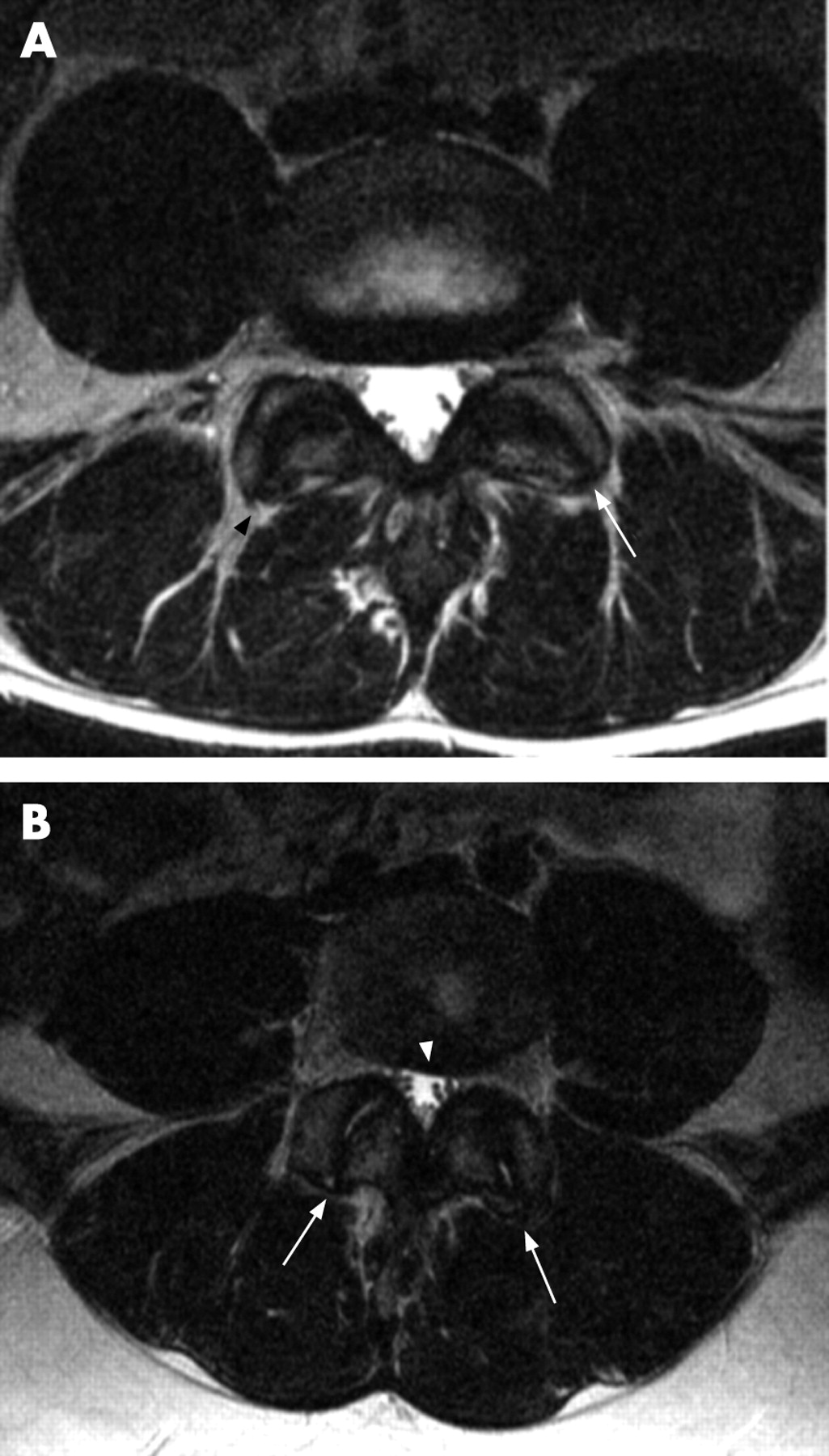
Facet joint arthropathy affected 23 of 33 subjects (69.7%; 95% CI, 51.3% to 84.4%), or 58/462 facet joints (five subjects had two levels involved and one subject had three levels). Arthropathy occurred most commonly at L5/S1 (30/462), followed by L4/L5 (24/462) and the remaining four lesions occurred at L3/L4 and L2/L3. The majority were mild (40/58) (fig 1A) and the remainder (18/58) showed moderate arthropathy (fig 1B). Only five pairs of joints were asymmetrically and bilaterally affected. All subjects with facet joint arthropathy had disc degeneration; however, the converse was not true. From the raw data the degree of facet joint change was greater than the disc degeneration change. In addition, we found one patient with asymmetrical orientation (fig 1A) and one with symmetrical coronal orientation of the facet joints. Thickening of the ligamentum flavum was present in 10 subjects (30.3%; 95% CI, 15.6% to 48.7%). These arose from 22 lamina, of which 10 adjacent facet joints showed moderate arthropathy.
Synovial cyst formation
Synovial cysts (fig 2) were present in 10 of 33 subjects (30.3%; 95% CI, 15.6% to 48.7%), who had a total of 15 cysts, measuring between 2 and 4 mm. Eight of the 15 involved left sided joints and seven involved right sided joints. All were related to facet joint arthropathy, with eight of the 15 joints showing moderate arthropathy. These synovial cysts occurred at L2/L3 (1/15), L3/L4 (1/15), L4/5 (7/15), and L5/S1 (6/15). Two (2/15) were on the epidural side and the remainder on the paravertebral side. None extruded into the exit foramina. Neither of the epidural cysts caused significant compression or stenosis.

Disc related disease
Disc degeneration
Thirteen of the 33 players (39.4%; 95% CI, 22.9% to 57.9%) showed disc degeneration, involving 15 of 231 discs (6.1%; 95% CI, 3.4% to 10.0%) (T11/12 to L5/S1). One patient showed disc degeneration at three levels (fig 3). The majority were at L5/S1 (9/15), followed by L4/L5 (3/15), and the remaining three discs were at T11/T12, L2/L3, and L3/L4. If only the last two discs in the lumbar spine were considered, then the proportion of degenerate discs was 16.7% (95% CI, 8.6% to 27.9%) (11/66). The majority (13/15) of all discs showed a mild degree of degeneration and the remainder showed moderate changes. One subject with moderate disc degeneration had narrowing of the L5 exit foramen.

Disc herniation
All the above 13 subjects showed broad central (12/15) or focal central disc herniations (3/15). The majority were of a mild degree (14/15) and did not touch or displace nerves. One was classified as moderate and this, together with a constitutionally narrow canal, caused moderate central canal stenosis. One subject had a Schmorl’s node; however, no limbus vertebrae, apophyseal injury, or Scheuermann’s disease was evident in any of the subjects. Two subjects showed a focal posterior high intensity zone.
There were no subjects with Modic end plate changes and no reactive change was identified around the Schmorl’s node.
Pars injuries
Pars injuries occurred in nine of the 33 subjects (27.3%; 95% CI, 13.3% to 45.5%), all affecting the L5 level, with one subject having an additional injury affecting the L4 level, making 10 injuries in all. Six of the 10 injuries were bilateral, three affected the right pars unilaterally and the remaining one the left. Five were chronic stress reactions (fig 4A), three were chronic stress fractures (fig 4B), and the remaining two showed features consistent with subtotal stress fracture (fig 4C). There were no acute stress fractures. Of the three chronic fractures, two showed grade 1 slip (with mild to moderate narrowing of the exit foramina) and one showed a grade 2 slip (with moderate to severe exit foramen narrowing). The subject with grade 2 slip had a rounded superior end of the S1 superior end plate and a wedged L5 (fig 4D).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Other findings
There was no evidence of spina bifida or alignment abnormalities such as scoliosis, or disease of the end plate or apophysis such as Scheuermann’s disease. However, three subjects had constitutionally narrow canals and in one case this contributed to asymptomatic stenosis (fig 1B).
DISCUSSION
Facet joint arthropathy
Facet joint arthropathy can be an important source of lumbar pain12–15 from joint capsule stretching, trapped synovium, and osteophyte impingement on the nerve root. In our subjects, facet joint arthropathy was the most common finding (70%), occurring most often at L4/L5 and L5/S1 and mostly bilateral. This rate is much higher than in the asymptomatic general population (8% to 21%).12 16 This is particularly significant as the mean age of the population in those studies was much higher than in ours (mean 42.3 years16 and 35 years12). This suggests premature degeneration of these joints in tennis players.
Most investigators suggest that facet joint degeneration occurs as a result of disc degeneration.17 18 In tennis players, degenerative changes do not appear to follow this pattern. The majority of our subjects had mild and a few had moderate arthropathy. In some, arthropathy occurred without disc degeneration and in some cases the degree of arthropathy was more extensive than the degree of disc change. Our findings are supported by a study by Videman et al, who found that facet degeneration occurred in 20% of subjects before disc degeneration.19
Tennis requires more frequent, repetitive, and rapid rotation from the lumbar spine than other sports. The modern tennis ground stroke, which is more front facing, may increase rotational forces about the facet joints, especially when topspin is added to control the ball (particularly on hard courts) and when a two handed stroke is used. In addition, increased speed of the ball (especially on grass courts) may play a part in the increased degree of rotation needed to return and control the ball.
We found one case of asymmetrical facet joints (facet joint tropism), a finding associated with disc herniation,20 spondylolisthesis, and disc degeneration.21
Synovial cyst
Synovial cysts can cause compression of neural structures in the epidural, or more commonly, the foraminal space.22 Synovial cysts in our subjects occurred more often than in the asymptomatic population (30.3% vs 0.6%).23 They occurred most commonly at L4/L5 and L5/S1 and in association with facet arthropathy. This is in agreement with previous reports in symptomatic non-athletes.22 24
Only two of the 15 cysts identified were in the epidural space. Neither of these was causing significant compression of the cauda equina. Most occurred in the paravertebral space where theoretically pain could be caused by capsular distension. The capsule of the facet joint is certainly known to be stronger in the usual direction of stretch (flexion) than in the direction perpendicular to normal stretch (axial rotation).25 Repetitive twisting and flexion from play (as described above) would increase tension on these fibres and predispose to the formation of facet joint cysts. It is known that in the degenerate spine facet cysts occur commonly in the younger age group and posteriorly more often than anteriorly.24 This may be related to supine positioning during imaging, or to reinforcement of the anterior capsule by the ligamentum flavum.24
Disc related disease
Disc degeneration
Salminen et al found a comparable rate of disc degeneration of 37% (vs 39.4%) in asymptomatic non-elite athletes of a similar age (18 years).26 The location of degeneration in our subjects increased in the caudal direction, and was most frequent at the L5/S1 and L4/L5 levels (the latter is the site of maximum spinal motion). Multilevel disease occurred rarely (in only two of the 33 subjects). Furthermore, we found less advanced changes such as disc height reduction than in other sports27–29 (3% vs 5.6–13.1%). Other advanced changes, Modic changes, Schmorl’s nodes, and end plate irregularity were also not found. Signs of disco-vertebral overuse such as limbus vertebrae and other apophyseal injuries were absent.
These findings suggest that disc degeneration in tennis players follows the normal pattern of age related change. Tennis has reduced axial loading compared with other sports, which have higher rates of disc degeneration (61–63.6%)30–32 and disco-vertebral overuse.15 Heavy lifting as part of training or during sport may also influence disc degeneration, but this form of training is not usual in tennis.15 33 34
What is already known on this topic
Trunk injuries are the third commonest type of injury in tennis after those to the lower and upper limbs.
Pars injuries are the second most common type of stress injury in elite tennis players, particularly affecting those under 18.
Injuries are related to repetitive movement.
What this study adds
Asymptomatic findings in the lumbar spine of young elite tennis players are common and arise in the posterior elements of the lower spine.
The most frequent are facet joint arthrosis and synovial cysts, with pars injuries also occurring relatively often. These may be related to rotation, hyperextension, and flexion during play.
Disc herniation and high intensity zones
Disc herniations are relatively common in asymptomatic non-athletes (16%)26 and athletes (21.1%)31 of a similar age. Various studies have suggested that herniations are often coincidental findings.12 16 35 In our players, disc herniations occurred at a higher rate (39.4%) than in those reports. Disc herniations can be the result of axial loading forces and rotational forces causing tearing in the inner annulus.8 The increase in rotation forces in tennis, particularly during serving and ground strokes (especially two handed), may explain the increased incidence of herniations. It is, however, possible that disc herniation, which can be a subjective assessment, was overdiagnosed.
No previous studies have examined the prevalence of high intensity zones in the lumbar spine of elite tennis players or other young elite athletes. The clinical significance of this finding is controversial. Some suggest that it can be associated with pain.36 In a group of asymptomatic non-athletes slightly older than our own (20 to 29 years), Weishaupt et al found a rate of 8.3%12—slightly higher than our rate of 6.1%. The location of the high intensity zones was also similar to that in Weishaupt’s report, occurring at L4/5 or L5/S1. Again this shows that our rates are similar to normal subjects. High intensity zones probably result from flexion or rotation forces on the disc,8 which are common during the follow through of serving and ground strokes.
Pars injuries
The pars is the second most common site of stress injuries in tennis. Injuries to the pars occur more often in elite players <18 years old (20.3%) than in those over 18 (7.5%).37 The rate of pars injury in our study was similar to the former value, at 27.3%. In tennis, hyperextension can be a cause of these injuries.15 This commonly occurs during the serve37 and may be exaggerated to achieve top spinning. Top spinning could play a more crucial role on hard courts, where the bounce is higher. The modern forehand shot, from a more forward facing stance, can also result in a sudden hyperextension of the spine. Furthermore an increase in ball speed, with the modern game and grass courts, results in more hyperextension.38 Increased and repetitive rotation,15 as with two handed play, may also predispose to pars injuries.37 38 Unilateral injuries are more often related to rotation than to hyperextension. This was suggested by the increased incidence of sclerosis in the pedicle and posterior vertebral body.32 We found that half the subjects had bilateral injuries and half had unilateral injuries. All injuries were isthmic, occurring at the L5 level, and have been demonstrated by others.37
Other mechanisms of stress injury—such as loss of disc height (leading to increased stress on posterior elements),39 congenital anomalies (a less frequent cause of dysplastic type fractures), and Scheuermann’s disease (from compensatory lordosis)—were not found in our group and are probably not important mechanisms of injury in tennis.
Acute injuries occurred in 6.1% of our subjects and were easy to assess on STIR sequences. MRI has a high sensitivity for these injuries and can estimate healing potential.15 40 Acute injuries are important to recognise, as progression can be prevented simply by rest,31 as has been described in the tibia.41 Unilateral and partial fractures tend to have a better healing rate and if identified early an improved long term outcome can be achieved.42
Chronic stress fractures occurred in 9.1% of our asymptomatic players. These are important to recognise as they may represent healing or evolving lesions and can be asymptomatic.42–44
We found spondylolisthesis in 6% of our players (two of 33). Both had mild narrowing of the exit foramen, but without significant compression. We found markers of possible slip progression (wedged L5 or rounded superior end plate of S1) in one patient with a grade 2 slip.45
Limitations
Our study had few subjects, which limited its power and any statistical analysis possible. This is a consequence of the small numbers of young elite tennis players in our country. We had no control group of asymptomatic non-elite athletes. Also there have been few MRI studies on the young asymptomatic lumbar spine available for comparison. We made no assessment of interobserver variability during this study; however, images were reviewed in consensus by two observers to minimise errors from subjectivity.
Whether the subjects in our study were actually asymptomatic is another factor. It is known that in the younger athlete there is a higher incidence of back pain than in the normal population and this also depends on the sport played.46 High motivation to return to sport may also create differences in the pain threshold.31 In addition, there are strong career motivational reasons for young players to underreport pain.
We did not make an assessment of whether the players were left, right, or two handed and whether this correlated with side of stress fracture or asymmetry of facet changes.
CONCLUSIONS
MRI can show abnormalities in the lumbar spine of elite tennis players and these occur most often in the posterior elements of the lower lumbar spine. A large proportion had facet joint degeneration and associated synovial cyst formation. A significant proportion also had asymptomatic pars injuries, some of which are acute or chronic stress responses. The location of changes may reflect the strain on the posterior elements of the vertebrae to increased rotation, flexion, and extension forces on the lumbar spines of tennis players. The large proportion of asymptomatic abnormalities underlines the poor specificity of these findings, and other sources of pain should be considered
Recognition of these changes is important so that training techniques can be modified to prevent progression to symptomatic disease.
Acknowledgments
This study was funded by the Lawn Tennis Association.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
Conflict of interest: None declared.