Article Text

Abstract
Background Provision of prompt, effective analgesia is rightly considered as a standard of care in the emergency department (ED). However, much suffering is not ‘painful’ and may be under-recognised. We sought to describe the burden of suffering in the ED and explore how this may be best addressed from a patient centred perspective.
Methods In a prospective cohort study, we included undifferentiated patients presenting to the ED. We undertook two face to face questionnaires with the first immediately following triage. We asked patients: (a) if they were ‘suffering’; (b) how they were suffering; and (c) what they hoped would be done to ease this. Prior to leaving the ED, we asked patients what had been done to ease their suffering. Data were analysed thematically.
Results Of 125 patients included, 77 (61.6%) reported suffering on direct questioning and 92 (73.6%) listed at least one way in which they were suffering. 90 (72.0%) patients had a pain score >0/10 but only 37 (29.6%) reported that pain was causing suffering. Patients reported suffering from both physical symptoms (especially pain, nausea, vomiting and dizziness) and emotional distress (notably anxiety). Treatment (to ease physical and emotional symptoms), information (particularly diagnosis, reassurance and explanation), care (notably friendly staff) and closure (being seen, resolving the problem and going home) were the key themes identified as important for relief of suffering.
Conclusions In seeking to ease suffering in the ED, clinicians must focus not only on providing analgesia but on treating Emotional distress, Physical symptoms, providing Information, Care and Closure (EPICC).
- clinical assessment, effectiveness
- communications
- patient support
- psychology, patient support
Statistics from Altmetric.com
Background
In recent years there has been a commendable focus on patient centred medicine with increasing attention being paid to the timely assessment and management of acute pain. Pain is, in fact, the most common reason for presentation to an emergency department (ED); 78% of patients who present to the ED report pain, which is rated as severe (≥7/10) in more than a third.1 ,2 There is evidence to suggest that pain is under-treated in the ED.3 ,4 This has led to significant focus on the importance of timely and appropriate assessment and management of pain, which some regard as ‘the fifth vital sign’, alongside pulse rate, respiratory rate, blood pressure and temperature.5 There is an irrefutable need for this focus, as the management of pain is an extremely important part of the role of a physician.
With rising pressure on EDs, overreliance on addressing ‘pain’ alone as a means of improving patient wellbeing could potentially encourage a culture that seeks to address physical pain (nociception) while ignoring the psychological distress or ‘suffering’ of the individual. Further, focusing only on physical pain may neglect (a) other physical symptoms with the potential to cause equal suffering (such as nausea, dizziness or pruritus, for example) and (b) other forms of mental anguish (including anxiety, low mood, anger, panic and doubt). It is also possible for relatively mild physical pain to cause great mental suffering, which may not always be recognised in medicine.6 Indeed the aetiology of physical pain itself may often be primarily psychological or emotional.7
Ultimately, it is ‘suffering’ (and not just pain) that we are truly seeking to relieve, with attention paid to the relief of both its physical and mental sources. To quote the Canadian philosopher Leonard Sumner, “It is plausible to say of suffering, as it is not of pain, that its presence necessarily compromises our happiness, and thereby also our wellbeing. Suffering seems just the sort of condition which, in itself and apart from any further accompaniment, makes our lives go worse”.8 While there is an extensive literature regarding the management of pain in emergency medicine, there is very little literature around the burden of ‘suffering’ and, in particular, its non-nociceptive causes.
We aimed to address this gap in the evidence by describing: (a) the burden and nature of ‘suffering’ as reported by patients presenting to the ED; and (b) how patients hope that their suffering will be addressed in the ED.
Methods
Design and setting
We undertook a prospective cohort study in the ED at Manchester Royal Infirmary, which has an annual census of approximately 110 000 patients and is based in the inner city of Manchester in the northwest of England. All participants provided written informed consent. The study was approved by the research ethics committee (reference 11/NW/0245) and sponsored by the University of Manchester. This report forms the first stage of a planned two part analysis of the data collected.
Selection of participants
We included any patients aged >16 years who presented to the ED, in a convenience sample dictated by investigator availability. To obtain a representative sample, an investigator (EK) worked a rotational shift pattern incorporating all times of the day and all days of the week. For ethical reasons, we excluded patients with critical illness warranting immediate medical attention and those who declined or had no capacity to both participate and provide written informed consent. Given the importance of undertaking the initial questionnaire immediately after triage, it was not possible to include patients who could not speak English, as interpreters would have been required.
Data collection and processing
We undertook face to face questionnaires with all participants at the time of presentation or immediately after triage (the admission questionnaire). We provided a written information sheet detailing the purpose of the study (see online supplementary appendix). Patients were then asked: (a) if they were ‘suffering’; (b) how and why they were suffering; and (c) what they hoped would be done to address their suffering. Patients were asked to quantify their pain on an 11 point scale (with 0 representing no pain and 10 representing the most severe pain they could imagine). We recorded the data using a custom designed case report form, along with basic demographic details. A second face to face questionnaire was undertaken after the patient had been seen by a clinician and initial interventions had been undertaken but before the patient left the ED (the pre-discharge questionnaire). At this stage, patients were asked: (a) what had been done to ease their suffering; and (b) if anything had happened that made them suffer more. At each questionnaire, the investigator was permitted to clarify the question (eg, to define ‘suffering’) but did not provide prompts or ask patients directly whether they were suffering in specific ways.
A copy of the case report form is available in the online supplementary appendix. Data were entered into an electronic database with responses transcribed by one investigator (EK). All of the data entry (100%) was subsequently verified from source documents by a second independent investigator (RB).
Analysis
We undertook (a) a descriptive analysis, reporting the frequency of responses to each question to describe the overall burden of suffering in the ED and (b) a thematic analysis using the methodology advocated by Braun and Clarke9 to further explore and understand themes arising from the data. This thematic analysis was undertaken by RB and SK using an inductive (data driven) approach. The analysis included five phases: (a) familiarisation with the data; (b) generation of initial codes (using the precise words or phrases that were recorded in the case report forms contemporaneously. These codes were also the basis of the descriptive analyses presented); (c) searching for themes from the initial codes generated; (d) review of the themes identified to generate a thematic map of the analysis; and (e) generation of clear definitions and naming of themes and refinement of the overall story told by the thematic analysis.
Data were analysed using IBM SPSS Statistics V.20.0.0 (descriptive analyses) and NVivo V.10 (QSR International Pty Ltd, 2012; thematic analysis). The sample size was calculated to provide adequate statistical power for multivariate analyses, which will be reported separately.
Results
We included 125 patients between May and June 2012. Baseline characteristics of the participants are shown in table 1. All patients were interviewed both at the time of arrival and prior to leaving the ED. Seventy-seven patients (61.6%) reported that they were suffering, one (0.8%) patient was unsure and 47 (37.6%) patients reported that they were not suffering at the time of arrival in the ED. The distribution of pain scores, stratified by whether the patient reported that they were suffering, is shown in figure 1. Thirty-two (25.6%) patients with an initial pain score of ≤3/10 reported that they were suffering. Fourteen (11.2%) patients gave a pain score of 0/10 but reported that they were suffering. Two (16%) patients with a pain score of ≥7/10 reported that they were not suffering.
Baseline characteristics of the study population
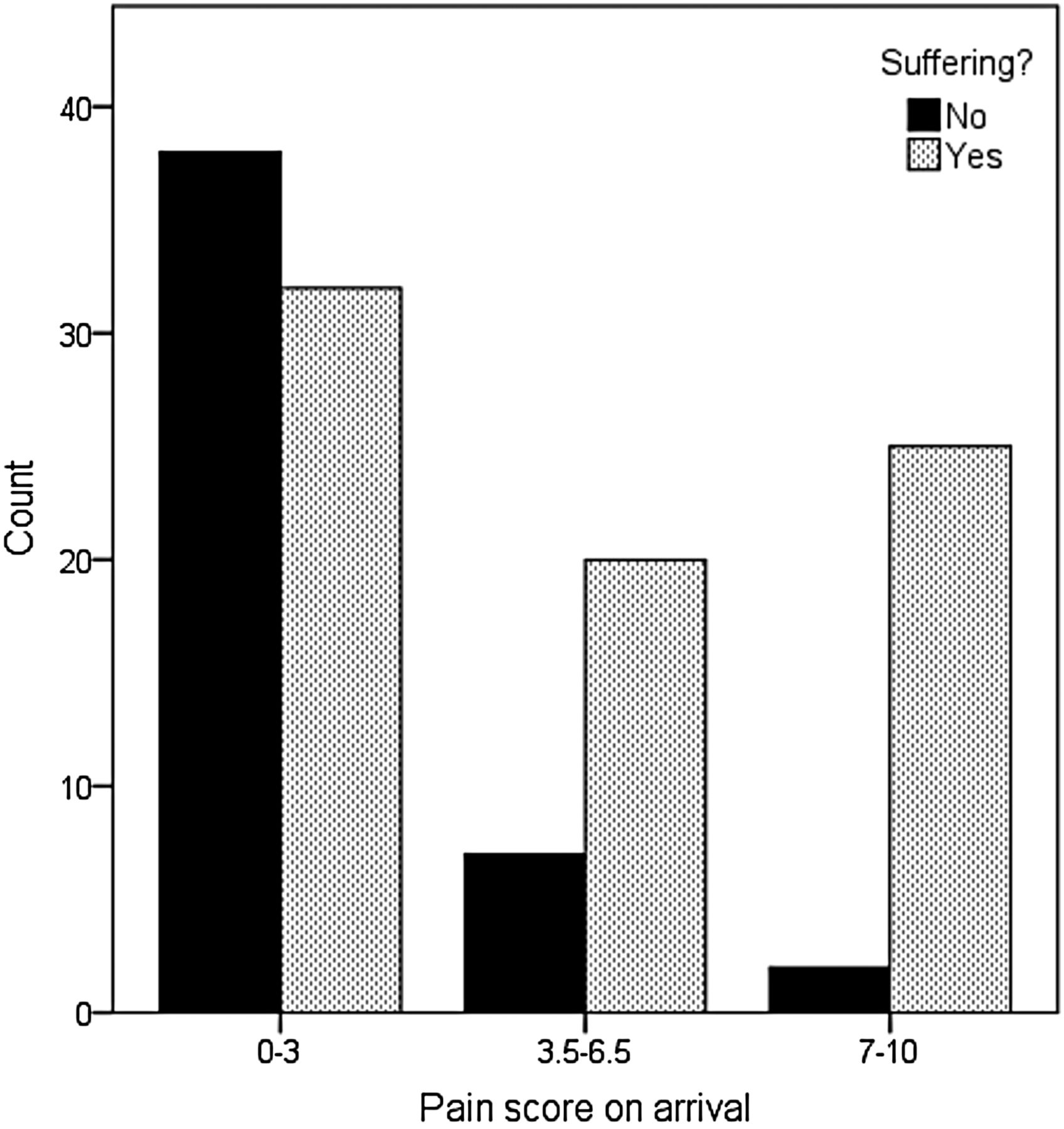
Distribution of pain scores stratified by the patient's response to the question, “Are you suffering?” at the time of admission.
Descriptive analysis
Patients reported 37 different responses to question 1 (“In what way are you suffering?”) with a total of 183 responses being provided by the 125 participants (table 2). Although 47 (37.6%) patients had reported that they were not suffering on direct questioning, only 33 (26.4%) patients listed no sources of suffering. Considering that anxiety, worry, concern, adjustment difficulties, low mood, embarrassment, agitation, bereavement, fear, uncertainty, stress and wanting to go home are all primarily emotional in nature, a total of 49 patients (39.2%) reported sources of emotional suffering. Assuming that discomfort, soreness and chest heaviness or tightness can be considered as forms of pain, a total of 58 (46.4%) patients reported that some form of pain was causing them to suffer. In contrast, 90 (72.0%) patients reported a pain score of greater than 0/10.
Sources of suffering as reported by patients at the time of presentation to the emergency department
When asked how they hoped the staff in the ED would help them to feel better, 125 (100.0%) patients gave at least one response. Ninety-four (75.2%) patients gave one response, 28 (22.4%) patients gave two responses and three (2.4%) patients gave three responses. Most commonly, patients were hoping for diagnosis (n=35, 28.0%), reassurance (n=25, 20.0%) and analgesia (n=13, 10.4%). The entire list of responses is shown in table 3. On being asked what had been done to ease their suffering prior to leaving the ED, 79 (63.2%) of the entire cohort listed at least one item (table 4).
Responses to the question, “How do you hope we will help you to feel better?” at the time of emergency department presentation
Response to the question, “What has been done to ease your suffering?” prior to leaving the emergency department
Of the patients who were hoping for analgesia (n=13), 12 (92.3%) received analgesia in the ED. Four (30.8%) of these patients later stated that the analgesia had eased their suffering. Of the patients who were hoping for explanation and/or reassurance (n=25), 12 (48%) later reported that reassurance or explanations had eased their suffering. The full range of responses to the pre-discharge questionnaire is shown in tables 4 and 5.
Response to the question, “Has anything happened to make you suffer more?” prior to leaving the emergency department
Thematic analysis
Our initial analysis identified three descriptive themes that reflected the structure of the initial and pre-discharge questionnaires: patients’ reported reasons for suffering; their expectations; and on leaving the ED, their judgement about whether expectations had been met. Following Braun and Clarke's approach,9 we were able to move on from our initial observations and develop a conceptual framework that we were satisfied represented the underlying meanings in the data, based around: (i) characteristics of ED patient suffering; (ii) tensions in patient perceptions of need; (iii) the importance of care; and (iv) the importance of closure.
Characteristics of patient suffering in the ED
Physical and emotional suffering occurred together. The physical symptoms reported were dominated by pain, although nausea, vomiting, dizziness and shortness of breath were also common. A minority of patients reported feeling hungry, thirsty or too hot, symptoms that may have been triggered by their immediate environment rather than a presenting condition.
While waiting in the ED, patients’ emotional distress was mainly characterised by anxiety and worry, around concerns such as fearing that they had a serious disease, not being believed by clinicians or anticipating clinical decisions that might represent bad news. For instance, one patient reported that they were anxious about being transferred from minors to majors for leg swelling.
Tensions in patient perceptions of need
In terms of how clinicians may ease the suffering of patients in the ED, we identified three distinct sets of patient perceptions of need. First, participants reported wanting reassurance plus information, particularly diagnosis, explanations and advice, indicating that these were the interventions that would reduce their suffering.
Second, these patients wanted treatment to relieve both physical and emotional symptoms. Patients often reported that treatment of their physical symptoms eased their suffering. Finally, while the patients wanted treatment, treatment itself was sometimes unfortunately seen as the cause of suffering. Indeed, some patients reported increased suffering, caused by delays to receiving painkillers, or nausea and vomiting occurring between triage and discharge. For instance, six patients noted that unpleasant or painful treatment such as intravenous cannulation had caused them to suffer more. Therefore, although the patients generally sought treatment, they could be disappointed by their experience of it.
The importance of care
Our data tell us about the importance of care in our approach to reducing suffering. Basic care was seldom mentioned when patients were asked how they hoped that clinicians would make them feel better, suggesting that patients themselves may not recognise this at the time of arrival in the ED. However, when asked what had been done to ease their suffering, 10 patients gave the answer ‘friendly staff’ and a further patient gave the answer ‘efficient staff’. One patient felt that an unpleasant waiting area had worsened their suffering while a further patient reported that open access to the ward area had caused them to suffer. Taken in conjunction with the expressed need for information and reassurance described above, these data highlight the importance of simple compassion and communication for reducing patient suffering in the ED.
The importance of closure
The theme of closure appeared to be strongly related to relief of suffering. As patients highlighted the impact of fear and uncertainty on their experiences in the ED, it is perhaps unsurprising that they valued closure, as represented by being able to go home, gaining understanding about their condition or being referred for definitive care. The data showed that prior to leaving the ED, 11 patients reported that being seen or being seen promptly had eased their suffering, four patients expressed their desire to be discharged or to go home and two patients were hoping for referral to other departments.
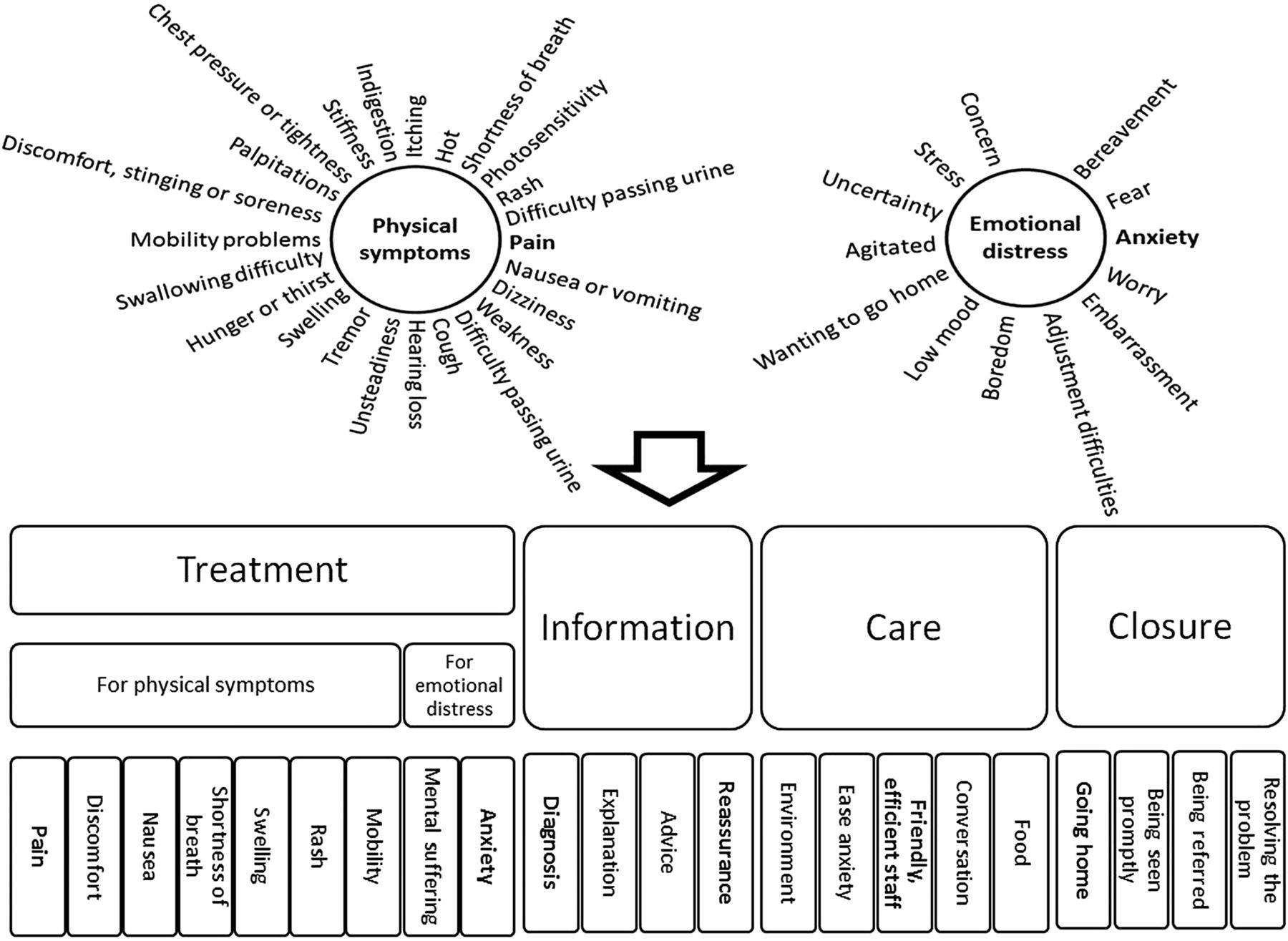
Considering these data together, we illustrated the themes identified in a conceptual model describing the nature of patient suffering in the ED and what our data tell us about how it may be addressed from a patient centred perspective (figure 2).
{kind=link}
{kind=link}
Conceptual model of the nature of patient suffering in the emergency department.
Discussion
Our findings have reaffirmed that the majority of patients are in pain when they first present to the ED. Indeed, 72% of the patients in our study reported a pain score greater than 0/10, which is similar to previous reports. Interestingly, however, only 37 (29.6%) of the cohort stated that pain was causing them to suffer on further questioning. Although pain was the most commonly reported source of suffering in patients presenting to the ED, the majority of the sources of suffering listed by patients were not related to pain. Our thematic analysis identified that patients reported suffering with a number of other physical symptoms (notably nausea, vomiting, dizziness and shortness of breath but also including basic needs such as tiredness or drowsiness and hunger or thirst) and emotional distress (notably anxiety, concern and embarrassment).
To our knowledge this is the first report of the burden and nature of suffering in patients presenting to the ED. While there is extensive literature regarding pain and pain management in emergency medicine, there has been relatively little focus on the burden of other important physical and mental symptoms that affect the wellbeing of our patients. In contrast, there has been much discussion about the relationship between physical and emotional pain in chronic settings.7
It is interesting to note that 62.4% of patients had stated that they were suffering in response to a direct question. However, 73.6% of patients had been able to describe at least one way in which they were suffering when questioned further about the ways in which they were suffering. When we asked patients how they hoped staff in the ED would help them to feel better, 100% of patients provided at least one response. The most common responses were ‘diagnosis’ and ‘reassurance’. Only 10.4% of patients stated that they were hoping to receive analgesia.
Therefore, while our findings with regard to the prevalence and burden of pain in the ED do support current initiatives to improve timely pain management, they also suggest that our patients may actually assign even greater value to explanations and reassurance from clinicians. When we asked, “What has been done to ease your suffering?” the most common positive responses were ‘explanation’ or ‘advice’ and ‘reassurance’, followed by ‘pain relief’. Indeed, of the patients who listed pain as a source of suffering at the time of arrival, over 90% received analgesia. However, less than a third of these patients subsequently reported that analgesia had relieved their suffering.
To ease suffering in the ED, our findings suggest that attention is required in four key areas: (1) treatment for (a) emotional and (b) physical symptoms; (2) information (particularly explanation, diagnosis and reassurance); (3) care (including staff friendliness and provision of a pleasant environment, as well as attention to basic needs, such as hunger and thirst); and (4) closure (being seen promptly, resolution of the problem, and either discharge from hospital or referral for definitive care). Thus the acronym EPICC (Emotional symptoms, Physical symptoms, Information, Care, Closure) may provide a useful framework for use in clinical practice.
Our findings are consistent with previous reports of patient expectations in the ED. Cooke et al10 demonstrated that over 90% of patients who visit the ED expect explanations of test results and the reasons for the tests. Poor communication has been shown to be the most common reason for complaints11 and is a frequent factor in the aetiology of patient safety incidents.12 Interventions to improve communication with patients have been shown to improve patient satisfaction in the ED.13 Despite the growing evidence in support of the value of communication,12 there is little centrally driven incentive to improve communication in the ED.
Contemporary quality indicators focus largely on process measures (eg, time to assessment; total time spent in the ED; senior sign off). We measure the measurable, which is not necessarily what is most valuable. This risks encouragement of a culture that seeks to achieve process targets at the expense of providing the explanations and reassurance that patients value most highly. We are particularly vulnerable to this eventuality as those valued interventions take time, and investment of time to provide explanation or reassurance may compromise the achievement of process targets. Indeed, 36.8% of our patients reported that nothing had been done to ease their suffering while 29.6% of patients reported that we had acted to worsen their suffering. This suggests that we are currently failing to adequately address the suffering of our patients. Perhaps our findings suggest that it is time to move towards a value based model of healthcare rather than our current focus on process targets as the primary measure of quality of care.
Limitations
In this work, we sought to describe the burden of suffering in the ED, to explore how patients hoped we would ease the suffering and, prior to leaving the ED, to determine what had been done to ease or worsen their suffering. In order to achieve this and for our findings to be valid, it was imperative that the research had as little impact as possible on routine clinical practice and the patient journey. Thus we used brief questionnaires immediately after triage and prior to leaving the ED, which helped us to achieve our goal.
We have not, therefore, explored the nature of each patient's suffering in great detail. Semi-structured interviews may be better designed to achieve that and are highly likely to enhance our understanding of this clinical problem. However, it is not possible to do this without substantially affecting the patient journey and routine clinical care. It is important for future work to explore the findings emerging from this work in greater depth. Semi-structured interviews with patients who have recently been treated in the ED may help us to achieve this in future.
Our sample size of 125 patients was decided upon in order to provide adequate statistical power for a separate quantitative multivariate analysis. It is possible that a larger sample may have picked up on additional themes relevant to patient suffering. However, our work does robustly demonstrate that our current approach to relieving suffering in the ED (which focuses largely on pain management and provision of analgesia) is inadequate, and we highlight the large additional burden of non-nociceptive sources of suffering. This should clearly lead on to further work with the humane goal of optimising our approach to the relief of suffering in patients presenting to the ED.
Areas for future work
Our research has identified a number of areas for further work. We have reported that pain only accounts for a minority of the burden of suffering in the ED. Future work should focus on further exploration of this area with patients and clinicians, and on the development of interventions to successfully ease the suffering of patients at the time of presentation to the ED. It is particularly interesting to note that analgesia eased the suffering of less than a third of patients who were in pain, despite the fact that over 90% of these patients received analgesia. This suggests that further work should evaluate whether the effectiveness of analgesia is augmented when given alongside simple human interventions to improve communication between the practitioner and patient, such as explanation and reassurance. While we have identified that patients are seeking reassurance to ease their suffering, further work should explore this further to examine more closely what is meant by the term ‘reassurance’. Given the importance of a patient centred approach to this work, we advocate that further work in this area should be completed in partnership with patients.
Conclusions
Our work confirms that physical pain and suffering are different entities, which may be under-recognised in emergency medicine. We identified a plethora of physical and emotional symptoms that cause patients to suffer in the ED. To address this, our data tell us that patients are seeking information, care and closure. Future work should focus on the development of innovative approaches to address the under-recognised burden of patient suffering in the ED.
Acknowledgments
We acknowledge the support of the Manchester Biomedical Research Centre, the University of Manchester and the Manchester Academic Health Sciences Centre.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
Footnotes
Contributors All authors contributed substantially to the manuscript and meet the criteria for authorship.
Competing interests None.
Ethics approval The study was approved by the research ethics committee (reference 11/NW/0245) and sponsored by the University of Manchester.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data may be supplied on contacting the corresponding author.