Article Text

Abstract
Objectives The frequency and the severity of drug-related visits in emergency department (ED) make the improvement of adverse drug event (ADE) recognition a crucial issue. As part of a research project aiming to improve the diagnosis and the management of ADEs in ED, the authors conducted a pilot study whose primary objective was to assess ADE recognition by emergency physicians.
Methods The patients presenting to the ED were included at randomised time periods between 1 October 2007 and 31 March 2008 in this prospective cross-sectional study. The primary outcome was the frequency of ADEs that were attributed to a medication-related problem by the emergency physician.
Results A total of 423 patients met the inclusion criteria, of which 95 experienced an ADE (22.5%; 95% CI 18.6% to 26.7%). Emergency physicians correctly attributed 33 of these cases (34.7%; 95% CI 25.3% to 45.2%) to a medication-related problem. Of the 28 cases in which the ADE was considered as a ‘direct drug effect’ (29.5%; 95% CI 20.6% to 39.7%), 16 were correctly identified by emergency physicians (57.1%; 95% CI 37.2% to 75.5%). Of the 67 cases in which the ADE was considered as a ‘drug involvement in a multifactorial pathological condition’ (70.5%; 95% CI 60.3% to 79.4%), 17 were correctly attributed (25.4%; 95% CI 15.5% to 37.5%).
Conclusions ADEs are frequent in EDs and are not well recognised by emergency physicians, especially when the drug is involved in a multifactorial pathological condition.
- Emergency
- adverse drug events
- risk management
- pharmacoepidemiology
- assessment
- healthcare quality
- clinical care
- clinical management
- diagnosis
- research
- epidemiology
- statistics
- teaching
- bacterial
- infection
- clinical
Statistics from Altmetric.com
- Emergency
- adverse drug events
- risk management
- pharmacoepidemiology
- assessment
- healthcare quality
- clinical care
- clinical management
- diagnosis
- research
- epidemiology
- statistics
- teaching
- bacterial
- infection
- clinical
Introduction
Emergency departments (EDs) are an essential part of healthcare systems and serve as an interface between hospital and community. EDs are specialised to allow for the recognition and emergent care of any patient's chief complaint or condition severity. This context makes the ED an ideal place to identify and manage adverse drug events (ADEs).
ADEs are injuries resulting from a drug-related medical intervention1 that are suspected to be a significant comorbidity in many ED patients. Numerous studies have assessed ADE frequency in EDs (1.3% to 22.2%).2–15 Some of these studies have demonstrated that ED patients with ADEs had a higher severity score than patients without ADEs4 and were hospitalised more frequently,11 ,15 with longer median length of stay15 and even worse outcomes.4 It is also clear that ADEs leading to an ED visit result in increased healthcare resource utilisation and cost.16
Because of the frequency and the severity of ED drug-related visits, it is crucial that more efforts are used to improve the ED management of ADEs. The medical management of drug-related problems consists mostly in drug regimen optimisation or drug discontinuation at ED and communication with other care providers.17 However, successful treatment first depends on the ability of emergency physicians to attribute ADEs to a medication-related problem and intervene when necessary.
Recent data have suggested that emergency physicians are moderately successful in identifying ADEs in patients presenting to the ED.18 ,19 Some specificities of ED medical practice (eg, incomplete medication history or unavailability of drug dechallenge outcome) also make drug causality assessment difficult19 and should be considered before for developing a quality improvement project in this area. This pilot study set the groundwork for a larger project that aims to improve the physician's overall ability to diagnose and manage ADEs in the ED.
This research has been done to assess the emergency physician's skill in diagnosing ADEs. The primary objective was to quantify ADE recognition by emergency physicians. Secondary objectives were: (1) to examine the differences between attributed and unattributed ADE groups and (2) to identify factors that were associated with ADEs in ED patients.
Material and methods
Study design and setting
This cross-sectional observational study was conducted at a 3000-bed tertiary care hospital with an annual ED census of 64 000 visits. Trauma ED, gynaecological ED and psychiatric ED are physically separated from medical ED and have not been considered for this project. Medical staffing in this ED consisted of junior emergency physicians with senior supervision, with the result that any final medical decision was checked by a senior emergency physician.
The study was approved by our Institutional Ethics Board. Clinicians involved in the care of included patients were unaware of the study.
Study population
All patients presenting to the ED of the study hospital between 1 October 2007 and 31 March 2008 were eligible for enrolment. Data were collected by pharmacy students (fifth professional year degree) completing a final course in ED on weekdays mornings. Fifty collection periods were defined with manual calendar randomisation to ensure a regular distribution of weekdays. All patients registered in the ED at the beginning of each period were included, regardless of severity level. Patients were excluded if: (1) they were 15 years old or less; (2) they were trauma patients; (3) they were gynaecological patients; (4) they presented for acute psychological disturbances or (5) they (or their relative in case of disability) did not agree to complete the survey. Identifying patient numbers were subsequently checked and in case of repeated ED admissions, only the first visit was considered for analysis.
Data collection
Information was prospectively collected in real time after patient inclusion, during the care. Trained pharmacist students on final course reviewed all available ED charts (ie, clinician records, nursing notes, emergency medical services logs and discharge instructions) and interviewed the patients and/or their relatives when possible. Supervision was done by clinical pharmacists, fellow and professor. Hospitalised patients were followed to collect information about their progress and outcome. In cases of discharge, further information could be obtained from any medical correspondence but not from the patients themselves.
Data collection included: (1) socio-demographic characteristics; (2) medical history; (3) current clinical status; and (4) patient outcome. Special attention was focused on drug exposure, including self-medication, during the 2 weeks preceding the ED visit. Drugs were classified on the basis of the Anatomical Therapeutic Chemical (ATC) classification index, which is recommended by WHO for drug utilisation studies (see online appendix). The emergency physician's diagnosis was coded according to the International Classification of Diseases 10th revision. Cases with two or more final diagnoses were recorded as polypathology.
Primary outcome measure
The primary outcome was the frequency of ADEs that were attributed to a medication-related problem by the treating emergency physician. An ADE was considered ‘attributed’ if any evidence of ADE suspicion, ADE diagnosis or ADE management (eg, drug regimen optimisation, drug discontinuation, prescription of a symptomatic treatment) was documented on the ED chart. An ADE was labelled as ‘unattributed’ when no evidence was found that the emergency physician recognised or provided management of the ADE.
We defined an ADE as an injury (ie, noxious or harmful effect) resulting from a drug-related medical intervention.1 This definition included adverse drug reactions (ADRs), medication errors and drug interactions. ADRs are defined according to WHO as ‘noxious and/or unintended responses to medication which occur despite appropriate drug dosage for prophylaxis, diagnosis or therapy of the indicating medical condition.’20 Non-compliance, intentional drug poisonings and ADEs that occurred as a result of ED medical treatment were excluded.
ADEs were identified on the basis of reviewing ED charts, patient interviews and using validated databases of known drug side-effects. When two ADEs or more occurred in the same patient, only the most clinically relevant ADE was considered. Data were reviewed by a trained pharmacist and an emergency physician with special skill in internal medicine. Contentious issues were resolved by consensus and the expertise of a pharmacologist when required. ADEs were all events identified via formal diagnosis by ED staff, as well as those detected by investigators during data reviews. Thus, the study focused on ADEs either that had been the cause for the patient to present to the ED or were unrelated to the patient's chief complaint.
ADE severity was assessed according to the Common Terminology Criteria for Adverse Events.21 This assessment includes five stages of increasing severity: (A) spontaneous regression; (B) regression after symptomatic treatment; (C) hospitalisation with no life-threat; (D) life-threatening risk; and (E) death. No attempt was made to assess ADE preventability.
The drug effects were classified into the following two categories: (1) ‘direct drug effect’ (when the drug was judged to be the only cause of the pathological condition, eg, cough with ACE inhibitors) and (2) ‘drug involvement in a multifactorial pathological condition’ (when the drug was judged not to be the only cause of the pathological condition, but to have participated as a facilitating or aggravating factor, eg, patient death consecutive to intracerebral aneurismal rupture while vitamin K antagonist therapy). The agreement of this original approach with the validated Naranjo ADR Probability Scale22 was tested on a randomised sample of observations.
Data analysis
Comparison of means between groups had been tested for a Student's test for normally distributed variables and by a Wilcoxon rank sum test for the other variables. Comparison of groups for qualitative variables had been tested by a χ2 test. The link between ADE and covariables had been tested in a first time by univariate logistic models. Only variables with p<0.2 had been retained for the multivariate analysis. Selection of the variables of the multivariate model had been realised with a manual backward procedure. Only clinically relevant interactions had been tested. Outliers and influent observations were studied and the model fit was tested (Hosmer and Lemeshow). The κ index between ADE classification and the ADR Probability Scale was computed (and tested as equal or not to 0). All analyses were performed using SAS statistical software (SAS V.9.1; SAS Institute).
Results
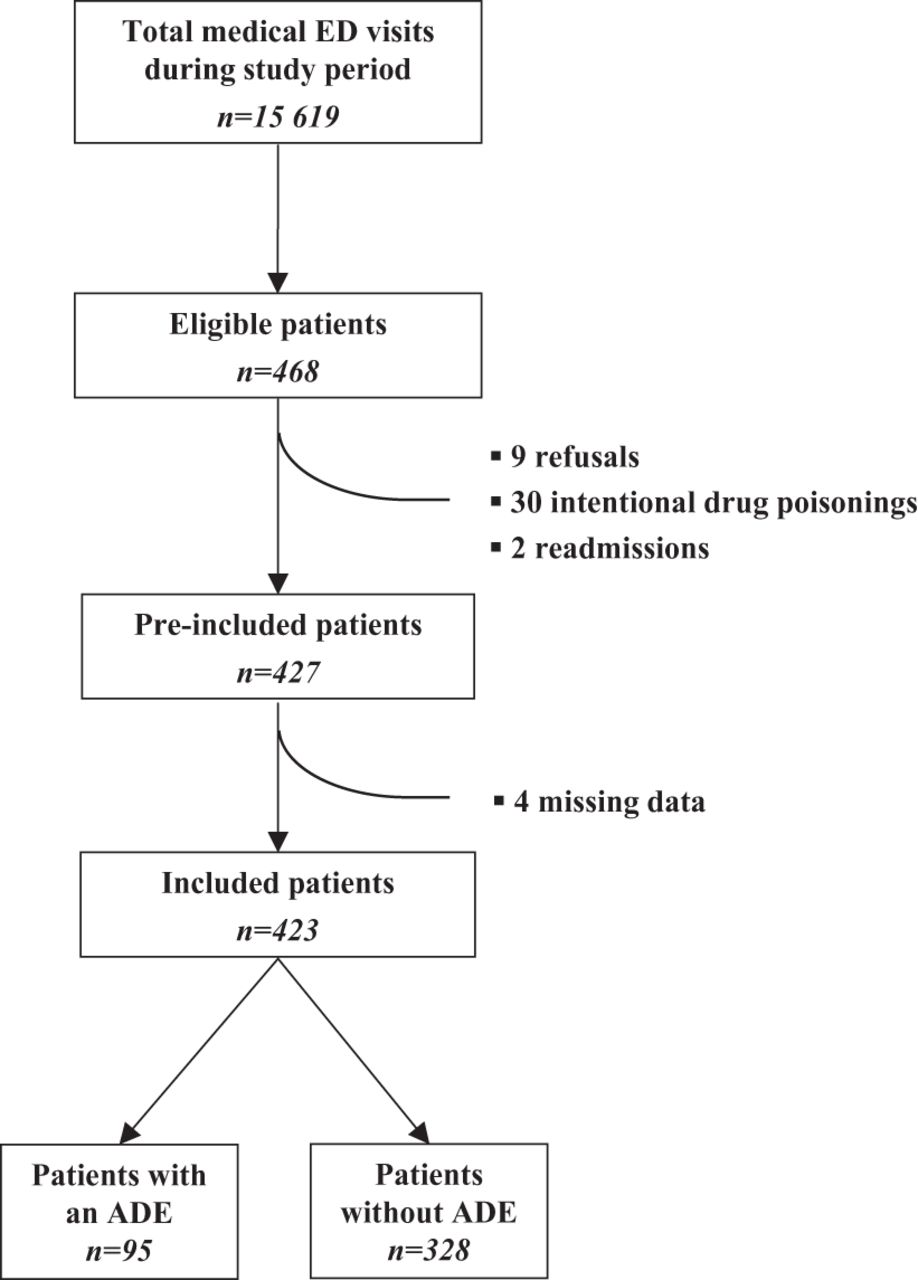
Four hundred and twenty-three patients met inclusion criteria (figure 1). The characteristics of the study population are presented in table 1. Included patients differed from the overall medical ED patients admitted during the study period for mean age (respectively 62.4±22.2 vs 54.9±23.2 years, p<0.0001) and hospitalisation rate (61.0 vs 52.2%, p<0.0001), but not for gender.
Characteristics of the study population and comparison between ADE and no ADE groups
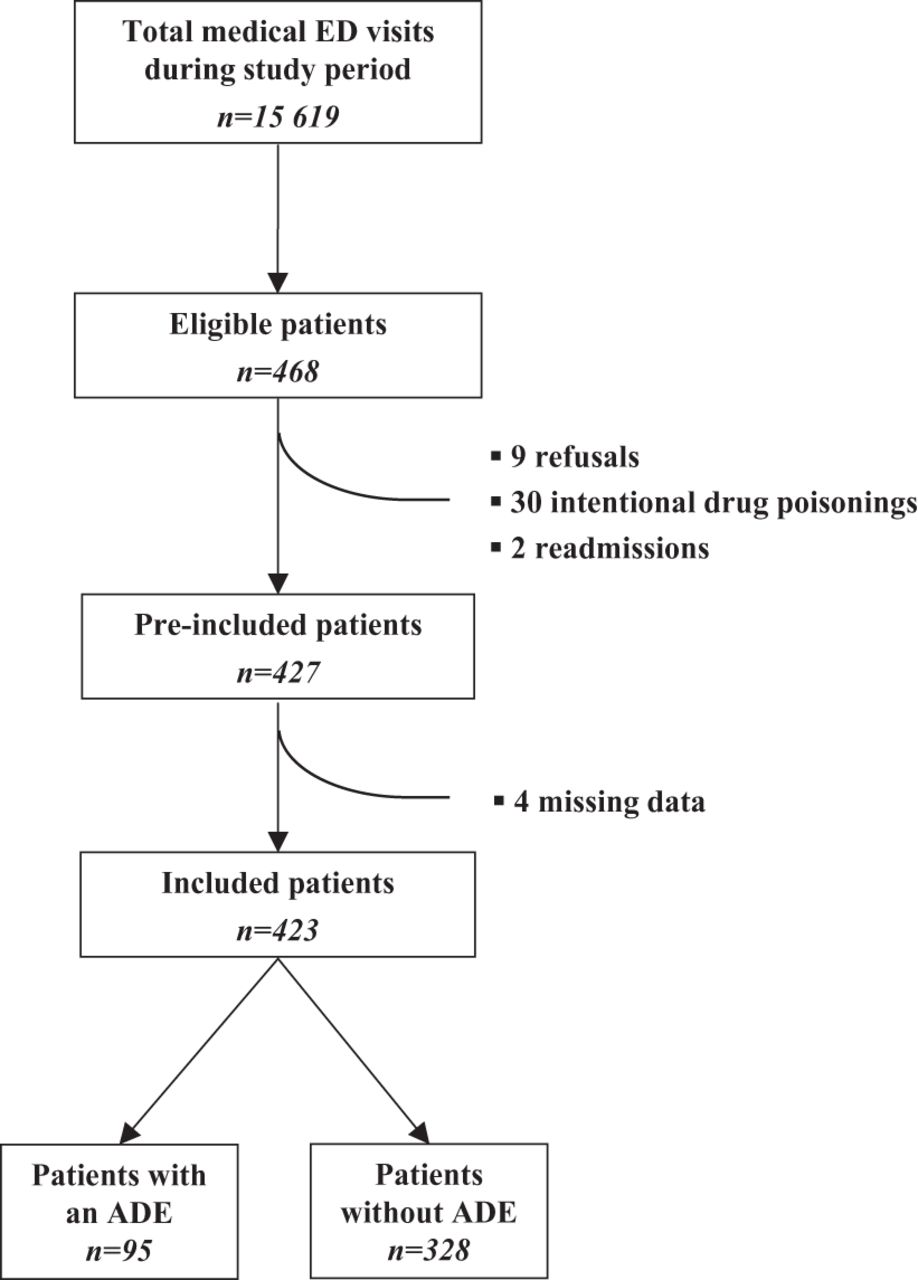
Patient flow. ADE, adverse drug event; ED, emergency department.
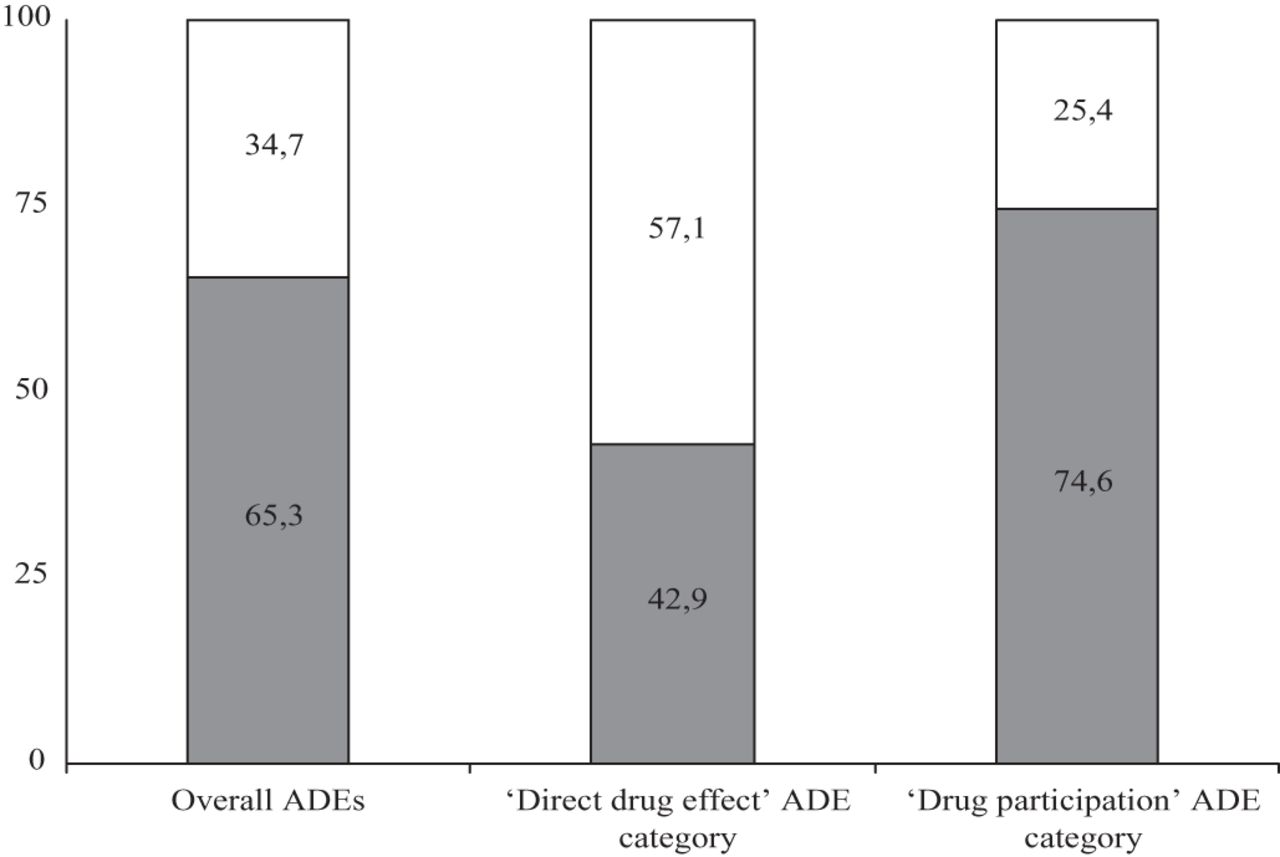
Using the inclusion criteria, it was determined that 95 patients experienced an ADE (22.5%; 95% CI 18.6% to 26.7%). Emergency physicians attributed 33 of these cases (34.7%; 95% CI 25.3% to 45.2%) to a medication-related problem. Drugs were judged to be the only cause of the event in 28 patients (29.5%; 95% CI 20.6% to 39.7%). Of these 28 cases, 16 were identified by emergency physicians as medication-related (57.1%; 95% CI 37.2% to 75.5%). In 67 cases (70.5%; 95% CI 60.3% to 79.4%), the drug effect was combined with the influence of other pathological factors. Of these, 17 (25.4%; 95% CI 15.5% to 37.5%) were attributed to an ADE by the emergency physician (figure 2).
{kind=link}
{kind=link}
Attribution rate for different adverse drug event (ADE) categories.
Sixty-nine ADEs (72.6%) led to hospitalisation, of which seven were deemed to be serious (D gravity category). An average of 1.3 (SD 0.5) drugs was judged to be implicated in ADE occurrence.
While classifying ADEs, it had been noticed that a Naranjo ‘doubtful’ or ‘possible’ score corresponded to our ‘drug involvement’ category and a Naranjo ‘possible’ or ‘definite’ score corresponded to our ‘proper drug effect’ category. Agreement between our ADE assessment method and the ADR probability scale was correct (κ=0.83; 95% CI 0.44 to 1.00).
In 68 cases (70.5%), only one drug was involved in the ADE, usually a daily medical prescription (96.1%) or occasionally a self-medication drug (3.9%). Considering the whole ADEs (whether attributed or not), the classes of medications most frequently implicated in ADE occurrence were: (1) ATC-C ‘cardiovascular system drugs’ (36.2%); (2) ATC-N ‘nervous system drugs’ (17.3%); (3) ATC-A ‘alimentary tract or metabolism drugs’ (11.0%); (4) ATC-B ‘blood and blood forming organs’ (8.7%); and (5) ATC-M ‘musculo-skeletal system drugs’ (8.7%). The ‘drug involvement’ category represented 51.5% of attributed ADEs (17/33) and 80.6% of unattributed ADEs (50/62) (table 2).
Comparison between attributed and unattributed ADE patients
The results of the comparison between ADEs and non-ADEs patients are presented in table 1 (univariate analysis). After adjustment for possible confounders, the multivariate analysis has shown that ADEs were significantly more frequent in hospitalised patients (OR=5.06; 95% CI 1.71 to 14.92; p=0.003), in cases with involuntary intoxication (OR=5.5; 95% CI 1.46 to 20.69; p=0.012), polypathological condition (OR=3.68; 95% CI 1.65 to 8.23; p=0.001), endocrine or metabolic pathology (OR=5.37; 95% CI 1.59 to 18.09; p=0.013) or in patients with daily prescription of cardiovascular system drugs (OR=2.77; 95% CI 1.24 to 6.15; p=0.007). Polymedication was significantly associated with ADE observation only in patients discharged after ED examination (OR=1.39; 95% CI 1.16 to 1.67; p<0.0001). Neither outlier nor influent observation was detected. A good fit of our model was not rejected (p=0.56).
Discussion
These results suggest an ADE frequency higher than 20%, but not readily identified by the emergency physicians. ‘Drug involvement in a multifactorial pathological condition’ was both the most frequent and the less attributed ADE category. The observation of an ADE in ED patients was most often associated with polypathology, endocrine or metabolic diseases and cardiovascular system drugs.
Some studies found an ADE frequency similar to ours (20.1% to 22.2%),3 ,4 ,13 but most found a lower frequency (1.3% to 12.6%).2 ,5–8 10–12 ,14 ,15 Many investigators chose an outcome definition which excluded events when causes other than drugs were possible and thus were likely to underestimate ADE frequency. An association with polypathology13 ,23 ,24 and/or metabolic pathologies was previously found.11 ,24 Polypathology is frequently accompanied by polymedication and thus is expected to be associated with ADE observation. Concerning endocrine or metabolic diseases, our results have important implications because diabetes and hydro-electrolyte disorders are very common clinical situations in EDs.
We voluntarily chose a pragmatic definition of the primary outcome to reflect as well as possible on the awareness of the emergency physicians. Asking emergency clinicians for their diagnosis could be a way to examine their ability to detect an ADE but does not demonstrate whether they clinically intervened. The management of drug-related problems and the reduction of their recurrence yet depend on clinical interventions such as medication regimen optimisation, follow-up plans or patients’ and care providers’ feedback and education.
A stringent study recently examined the frequency of drug-related visits that emergency physicians attributed to medication-related problems.19 In agreement with these first results, we found that a significant proportion of drug-related visits are not deemed medication related by emergency physicians. Nevertheless, our data show a higher proportion of unattributed ADEs. This is consistent with the fact that this study did not focus on just ADEs leading to ED presentation, but instead included ADEs unrelated to the patients' chief complaint, a type of ADEs whose diagnosis was expected to be more difficult.18 One of the most patent explanations for these findings consists in the information bias resulting from ED context. Emergency physicians may have attributed more drug-related visits to ADEs if additional information, which became available during the follow-up period, had been available to them during the ED visit. As a consequence of the ED organisation, medical care essentially focuses on the patient's chief complaint with little time for further investigation. When patients present with minor complaints, emergency physicians generally just treat the patient's symptoms without taking a more detailed medication history and can miss the opportunity to identify an ADE. Factors such as crowding or high workload may also have influenced ADE identification.
Bias and limitations
No relationship was found between age or gender and ADE observation. This is consistent with the hypothesis that age or gender is not an independent risk factor for ADE because it does not take into account patient-specific physiological and functional characteristics.25 However, many studies found a link between increasing age or female gender and risk for ADE.4 ,5 ,11 In the same way, polymedication is a well-known risk factor for ADEs,11 ,13 ,23 ,24 ,26 but the number of daily medications was unexpectedly associated with ADEs only in discharged patients. These discrepancies raise concerns about the relevance of our results and suggest we have not adjusted for some confounders, such as for comorbid conditions. The strong association with the ‘polypathology’ condition is consistent with this hypothesis.
Data were collected prospectively and their reliability was ensured by examination of various information sources including patient interviews. However, some data were difficult to retrieve in the ED context (eg, complete medication history when the patient's interview was impossible or condition evolution in discharged patients) and there may have been some difficulties in concluding an ADE. Another limitation was that our study relied on a single investigator team to identify ADEs. Finally, the classification of drugs and diagnoses only at the first level of ATC classification index and International Classification of Diseases 10th revision simplified data analysis but made interpretation of the results more difficult.
Even though the results of this monocentric study could vary depending on emergency structure and healthcare system organisation, we are convinced that lack of recognition of ADE by emergency physicians is a general issue concerning any European ED structure. Another limitation is related to our sampling design that included only weekday morning patients. This may lead to a selection bias which could be confirmed by the fact that included patients were older and more frequently hospitalised than the overall medical ED patients and by the fact that our ADE frequency is higher than the proportion reported previously in literature, regardless of the variations in case definition, study design and patient populations.
Conclusions
This pilot study confirms the low rate of ADEs attributed to a medication-related problem by the emergency physicians, especially when the drug is involved in a multifactorial pathological condition. Our findings partly reflect the natural limitation of ADE identification in the ED, where working diagnoses are made according to incomplete information, and underscore the need for specific help to improve the performance of emergency physicians in this task. In addition to well known risk factors such as polypharmacy and polypathology, our findings emphasise that ED final diagnosis should be considered for identifying patients that emergency physicians need to be vigilant for ADE. Further research is now required to improve ADE recognition in ED context. Our experience also suggests that physician–pharmacist collaboration may improve the management of drug-related issues.
Acknowledgments
The authors thank Christelle Bordet, Marjolaine Dablaing, Claire Heauville, Jeanne Mendoumengue, Constance Riom, Guillaume Brement and Sébastien Ruaud for carrying out the patient interviews, and Sophie Bour for the linguistic support.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Prior presentations Part of these results were presented in the ACCP congress, April 2009, Orlando, USA.
-
Competing interests None.
-
Ethics approval The project was approved by the GNEDS (Groupe Nantais d'Ethique dans le Domaine de la Santé).
-
Provenance and peer review Not commissioned; externally peer reviewed.