Article Text

Abstract
Delirium is a serious and common condition that leads to significant adverse health outcomes for hospitalised older adults. It occurs in 30%–55% of patients with hip fractures and is one of the most common postoperative complications in older adults undergoing orthopaedic surgery. Multicomponent, non-pharmacological interventions can reduce delirium incidence by up to 30% but are often challenging to implement as part of routine care. We identified a gap in the delivery of non-pharmacological interventions on an orthopaedic unit. This project aimed to implement a bedside sign on an orthopaedic unit to reduce the occurrence of delirium by prompting staff to use multicomponent evidence-based delirium prevention strategies for at-risk older adults. Quality improvement methods were used to integrate and optimise the use of a bedside ‘delirium prevention’ sign on an orthopaedic unit.
The sign was implemented in four target rooms and sign completion rates increased from 47% to 83% (95% CI 71.7% to 94.9%; p<0.001) over a 10-month period. The sign did not have a significant impact on delirium prevalence. The mean Confusion Assessment Method (CAM)+ rate during the baseline period was 8% with an absolute increase in the intervention period to 11.4% (95% CI 7.2% to 15.8%; p=0.31). There were no significant shifts or trends in the run chart for the proportion of patients with CAM+ scores over time. The sign was well received by staff, who reported it was a worthwhile use of time and prompted use of non-pharmacological interventions. This quality improvement project successfully integrated a novel, low-cost, feasible and evidence-based approach into routine clinical care to support staff to deliver non-pharmacological interventions. Given the increased pressures on front-line staff in hospital, tools that reduce cognitive load at the bedside are important to consider when caring for a vulnerable older adult patient population.
- nurses
- evidence-based practice
- geriatrics
- healthcare quality improvement
- hip fractures
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Problem
Delirium is a serious and common condition affecting up to 64% of hospitalised older adults. It costs over US$164 billion per year in the USA alone and over US$180 billion in 18 European countries combined.1 Delirium carries an increased risk of mortality,2 functional decline3 and institutionalisation.4 From a health resource perspective, delirium is associated with increased length of stay5 and increased intensity of nursing care.6 Delirium occurs in 30%–55% of patients with hip fractures and is one of the most common postoperative complications in older adults undergoing orthopaedic surgery.7–10
This project was undertaken at Juravinski Hospital, one of the sites of Hamilton Health Sciences Corporation, a tertiary care academic site in Hamilton, Ontario, Canada. The orthopaedic ward (E2) has 35 beds and on average, 31 patients with hip fractures are admitted to this unit each month. The delirium prevalence on this unit was found to be 30.9% on a single day when evaluated by trained delirium assessors.11 Given the high prevalence of delirium on this unit and its association with mortality, cost and functional outcomes, we designed a quality improvement study to help address this issue.
We conducted focus groups with nurses on E2 to examine gaps in the delivery of evidence-based non-pharmacological delirium prevention interventions (promoting mobility, encouraging fluid intake, offering glasses/hearings aids). Nurses on this unit must screen for delirium using the Confusion Assessment Method (CAM), a commonly used and well-validated delirium screening tool.12 A ‘CAM+’ score indicates a positive screen for delirium. Nurses must also document non-pharmacological delirium prevention interventions employed during care. Our focus group discussions revealed that nurses found it challenging to remember all of the delirium prevention strategies and implement them into daily practice. We determined that a bedside tool to help staff implement delirium prevention interventions was worth exploring.
The aim of this quality improvement project was to introduce a new bedside sign on an orthopaedic unit over a 10-month period to help nurses and other staff use delirium prevention strategies.
Background
Delirium prevention should target those identified to be at-risk by addressing potentially modifiable risk factors through non-pharmacological interventions. Multicomponent interventions have been shown to reduce delirium incidence by up to 30% in randomised trials.13 14 A prominent, evidence-based model for non-pharmacological interventions is the Hospital Elder Life Programme (HELP), which has been implemented worldwide.15 Components of HELP protocols include daily visits, orientation, early mobilisation, fluid repletion, therapeutic activities, non-pharmacological support with sleep and vision and hearing adaptation. The efficacy of HELP has been assessed in a number of studies, which consistently show a reduction in delirium incidence by as much as 53% when compared with control groups.16 While length of hospital stay was not impacted statistically, the programme was reported to significantly reduce the odds of falling in older adults (OR 0.58; 95% CI 0.35 to 0.95) and led to decreased hospital costs, saving US$1600–US$3800 (2018 US dollars) per patient.15 The impact of HELP on delirium prevalence is dependent on the fidelity to the HELP protocol, which can be compromised by real-world challenges such as lack of availability of staff and volunteers, patient refusal and medical contraindications.15 Several attempts have been made to improve adherence, including staff and volunteer education and further simplifying the programme to reduce cognitive load. For example, a modified HELP that included only cognitive activities, nutrition and mobility protocols was implemented for older patients undergoing abdominal surgery and the odds of delirium were reduced by 56%, with length of stay reduced by 2 days.17 Family participation in delivering these interventions is also important. The Fam-HELP programme has demonstrated that engagement of family caregivers in preventative interventions for delirium is feasible.18 However, operationalising family partnership into daily practice is challenging and few studies focus on how families can help manage delirium in loved ones.19
There is minimal published evidence regarding the use of signage to increase delirium awareness, improve delirium prevention strategies or reduce delirium prevalence. There have been studies exploring sign use in hospital for other reasons, for example, providing bedside orientation20 and dry-erase boards for communication.21 Dry-erase communication boards have been demonstrated to help staff remembering care details for patients.22 A survey of health professionals demonstrated that patient whiteboards were a valuable tool to improve teamwork, communication and patient care for interdisciplinary teams.23 From the patient perspective one study showed that over 95% of patients found bedside whiteboards helpful and 92% read the information on the whiteboard frequently.24 Bedside signs and whiteboards are promising tools but none have yet been dedicated to delirium prevention.
Given the high prevalence of delirium on orthopaedic wards, there should be greater emphasis on supporting staff to use evidence-based delirium prevention interventions in daily care. There is little guidance on how to use signage to implement these interventions. We created, implemented and evaluated a multicomponent bedside sign on an orthopaedic unit to prompt staff to use these evidence-based non-pharmacological interventions. As per protocol, all electronic medical record (EMR) data were deidentified and informed consent was waived.
Measurement
This quality improvement project was conducted over a 10-month period on a 35-bed orthopaedic unit at a large academic hospital. Our process measure was sign completion rates. The signs have several fields related to each non-pharmacological intervention and signs were considered ‘complete’ if at least ¾’s of component fields were filled out. Due to resource constraints, we could not conduct weekly audits throughout the study but we assessed sign completion over several weeks at the beginning and the end of the intervention period.
Our outcome measure was the proportion of patients with a CAM+ score documented during their length of stay on the orthopaedic unit. CAM scores are documented by nurses on E2 once per shift with a compliance rate of over 90% at the time of the study. Use of the CAM in real-world settings may underestimate delirium prevalence25 but for this study it was impractical to use a trained assessor to screen for delirium every day for 10 months to determine the CAM accuracy. Therefore, we used the proportion of patients with a CAM+ score documented in the EMR to define ‘delirium prevalence’. CAM scores from E2 were collected monthly from the EMR between August 2017–September 2017 (baseline period) and October 2017–May 2018 (intervention period). Staff were surveyed at the end of the study to assess their impression of the sign’s impact on use of interventions.
Descriptive analyses were used to summarise demographic results and describe differences between baseline and intervention periods. Run charts were used to evaluate changes in CAM+ scores over time and were analysed using standard rules to detect any signal of special cause variation in the charted data points.26 Differences in sign completion and CAM+ rates at the beginning and end of the study were compared using two sample t-tests. This study follows the SQUIRE publication guidelines for reporting.27
Design
An interdisciplinary team made up of physicians, allied health, an education and development nurse clinician, and two geriatric clinical nurse specialists, was assembled to create the bedside sign. This multicomponent sign (figure 1) was based on HELP protocols, addressing the delirium risk factors of sensory impairment, dehydration, immobility, cognitive impairment and poor sleep. Each patient’s unique modifiable risk factors for delirium were highlighted so that nurses and other health professionals interacting with that patient would have visual cues, for example, to offer water or to put on eyeglasses.

Example of completed sign.
The QI implementation team met monthly during the baseline and intervention phases. All aspects of the project and intervention were designed in close collaboration with the unit manager on E2. Early nursing feedback demonstrated that the sign should target hip fracture patients who are at higher risk for delirium compared with patients admitted for elective joint replacement procedures. Therefore, we introduced the signs to four select rooms, which were identified as accommodating a larger proportion of patients with hip fractures compared with other rooms on the unit. Piloting the sign in four rooms first allowed us to make important early changes on a smaller scale before widespread implementation. Nurses and allied health staff working on E2 (n=40) participated in 10 min training sessions on accurate completion of the sign during one of their routine daily staff safety huddles. There sessions were conducted by an education and development nurse who was designated as the delirium prevention champion on the orthopaedic unit. Nurses and allied health staff completing the sign consulted patients and their families to determine specific details of care such as need for glasses or hearing aids.
The principle intervention was a bedside sign placed in four rooms to prompt staff to apply non-pharmacological interventions in daily routine care, with the ultimate goal of decreasing the proportion of patients with CAM+ scores over time. The remainder of the unit served as our control group as these patients were not exposed to the intervention.
Patient and public involvement
Patients and families were involved throughout the preparatory and intervention phases of this quality improvement project. Family members of patients admitted to the orthopaedic unit were invited to give feedback on the sign’s usefulness. Both patients and family members provided pertinent information (ie, answering questions about glasses and hearings aids) that assisted staff to complete the sign. Patients and family were informed that some of these questions were not part of routine care, but may have prompted action such as bringing hearings aids from home to the hospital. Acceptability of the intervention was measured through the family surveys. Burden of intervention to patients and families was not formally measured. The aim of the sign was discussed prior to administering family surveys. Patients were not involved in the study design or dissemination of results. There was no recruitment component to this project as the sign was used for all patients who were admitted to the four target rooms.
Strategy
We met with the E2 clinical manager several months prior to developing this idea to ensure that this QI initiative was feasible and aligned with the unit’s overall goals. This intervention was supported by a staff training and awareness campaign that was conducted by the education and development nurse and took place 2 weeks prior to sign introduction. There were also educational posters placed on the unit (online supplemental figure 1). After training was complete, the research team placed the delirium prevention signs in four target rooms. These rooms were more likely to be occupied by patients with hip fracture but due to patient flow and capacity there may have been other orthopaedic patients (eg, joint replacements) admitted. Throughout the study, focus groups with unit staff were conducted to identify areas for improvement and new change ideas. Phased improved was used to implement the sign and refine its use over time.
Supplemental material
The baseline period was defined as the months prior to sign use (August 2017–September 2017). Stages 1 and 2 involved preparations for sign implementation during the baseline period while stages 3, 4 and 5 occurred during our intervention phase (October 2017–May 2018). Details regarding the stages of this phased implementation project are outlined in table 1.
Stages of delirium prevention sign implementation
Results
There were 474 patients admitted to the four target rooms over the course of 10 months. The mean age was 75.8 (SD 12.8) almost 6 years older than the mean age of patients on the rest of the unit, 70.1 (SD 11.6). As we expected, there were a greater proportion of admissions for hip fracture in the target rooms compared with control rooms (42% vs 13%). This was consistent with our goal to try and target patients who were are at higher risk for delirium. Demographics for patients admitted to four rooms with the sign and the other rooms on the unit are displayed in table 2.
Characteristics of patients admitted to the orthopaedic unit (E2) at Juravinski Hospital from August 2017 to May 2018
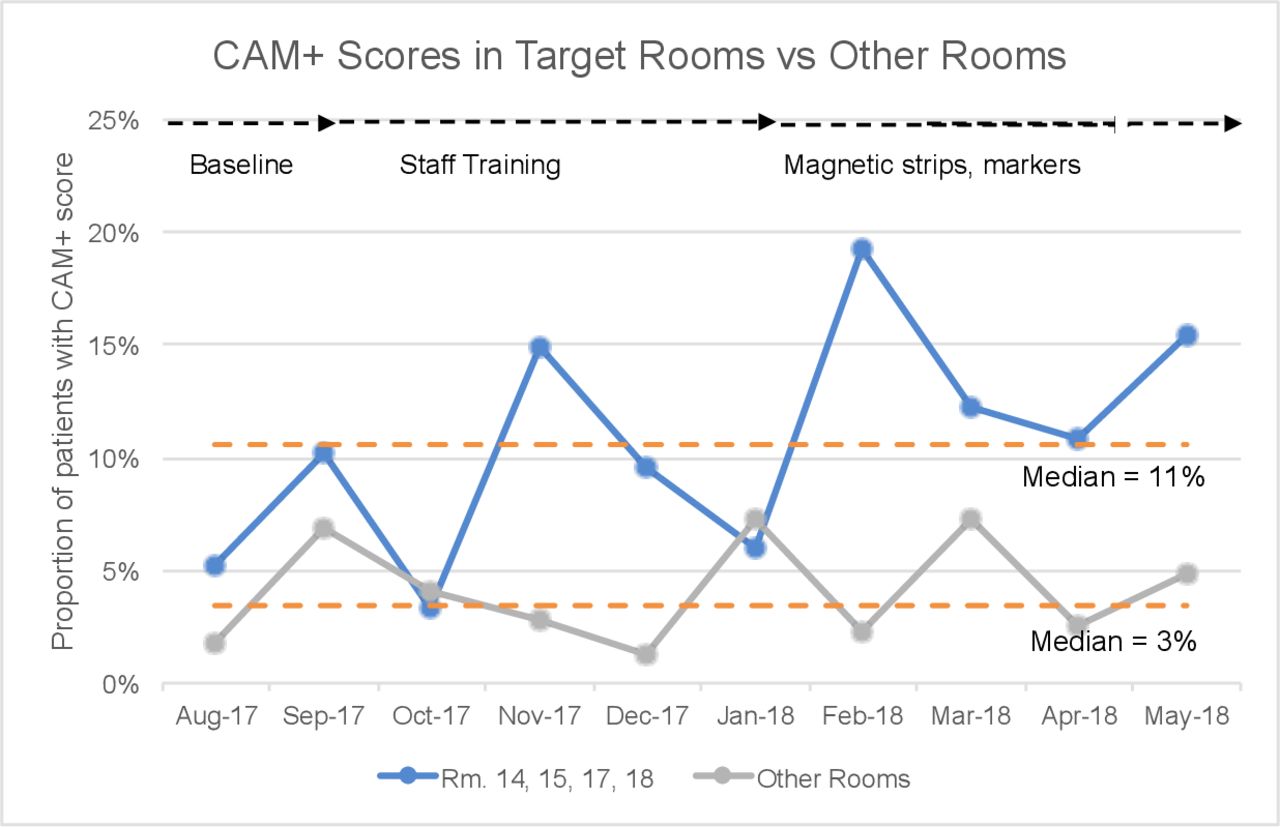
Our audits demonstrated that sign completion rates increased throughout the study period. Mean completion rate at the beginning of the intervention period was 47% with an absolute increase to 83% (95% CI 71.7% to 94.9%; p<0.001) by the end of the intervention period. The mean CAM+ rate during the baseline period prior to sign implementation (August–September 2017) was 8% with an absolute increase in the intervention period to 11.4% (95% CI 7.2% to 15.8%; p=0.31).
As demonstrated in figure 2, there were no significant shifts (six or more points on the same side of the median) or trends (five or more consecutive points increasing) over time.26 However, the proportion of patients with CAM+ scores did increase temporarily at isolated points after sign implementation in October and after signs were better secured to the wall with magnetic strips in February. These temporary increases were not observed in other rooms on the unit without the sign, indicating a possible non-random shift in data due to the sign’s impact. The mean baseline CAM+ rate in the rooms without the sign was 5.5% with a decrease to 4% (95% CI 2.2% to 5.8%; p=0.30) in the intervention period, indicating a stable environment on the unit throughout the 10 months (figure 2).
{kind=link}
{kind=link}
Run chart for proportion of patients with CAM+ scores.pdf. CAM, Confusion Assessment Method.
Towards the end of the study, we surveyed 20 family members regarding their perspectives of the sign (online supplemental figure 2). Eighty-five per cent answered that the sign was easy to understand and follow and 70% felt that it was helpful for communication. However, there was a clear need for more education about delirium because only 60% thought the sign provided a better understanding of delirium and just 50% thought it helped them care for their relative. More than 90% of unit staff (nurses, allied health) received educational sessions on how to complete and use the sign. At the completion of the study, surveys were distributed to elicit staff feedback (online supplemental figure 3). We elicited responses from 22/40 staff (7 allied health and 15 nurses) with an average of 12 years of work experience. 82% (18/22) of staff agreed or strongly agreed that the sign prompted use of non-pharmacological interventions and felt that completing the sign was a worthwhile use of time. Eighty-two per cent (18/22) of staff also agreed or strongly agreed that they would like to continue using the sign.
Lessons and limitations
We believe there are several factors that led to the success of implementing the sign on this orthopaedic unit. First, this quality improvement project was conducted in a stable environment with few changes to staff operation outside of intervention implementation and training. Second, we achieved strong engagement of nurses, clinical managers and other E2 unit staff throughout the process. Nurses play an important role in delirium identification and prevention and we ensured that they were involved in the direction of the project. Feedback from focus groups and surveys provided useful insights that supplemented the quantitative collection of EMR documented CAM scores. Despite non-significant impacts on delirium prevalence, the sign was well received by staff who felt that the sign prompted them to use non-pharmacologic interventions and was a worthwhile use of time. This is an important metric given the competing priorities of point of care staff on busy inpatient wards. Finally, we achieved buy-in from hospital administrators as the sign posed minimal risk to patients and was relatively low-cost at $C40 per sign, equivalent to approximately £23.
There are a few notable limitations, including using the CAM to detect delirium prevalence, the lack of balancing measures, the project’s short time frame and the small scale. Previous research demonstrates that the use of CAM by nurses under-represents delirium prevalence when measured outside of clinical studies.25 Though significant efforts were made through educational initiatives to increase the accuracy of nursing recognition of delirium prior to sign implementation, it is possible that accuracy was still low. Performing a chart review for key delirium words in nursing notes may have provided a more accurate reflection of delirium prevalence compared with the CAM+ scores. This would have required additional resources and will be considered for future sign evaluation projects. Though we did not collect direct balancing measures, which would have been helpful to influence future intervention, we did evaluate staff perception about whether the sign was a worthwhile use of time. Additional data points over a longer time frame would have improved our ability to assess trends and understand sustained effects. In particular collecting more data points during the baseline period prior to sign implementation would have allowed us to detect underlying trends that may have already been occurring. The impact of other unit changes (staff education and changeover, seasonal changes of patient presentations) could have influenced CAM documentation. We tried to limit these effects by comparing results with the proportion of CAM positives in other rooms where signage was not installed. The CAM positive scores in those rooms remained unchanged over the study period with no increased trends after any intervention. Finally, this study was carried out in four rooms on a single orthopaedic unit potentially limiting generalisability to other units and hospitals. However, pilot studies like this are important first steps in order to refine a process and ensure buy in prior to widespread implementation.
Conclusions
A multicomponent sign to prompt delirium prevention strategies was successfully implemented in four patient rooms on an orthopaedic ward and was well received by staff and families. Sign completion rates by staff increased by more than 50% over a period of 10 months. The intervention did not lead to significant changes in delirium prevalence, as measured by the proportion of patients with CAM+ scores over time. Increases in the proportion of patients with CAM+ scores were detected following initial sign implementation and after the signs were better secured to the wall and these changes were not demonstrated in rooms without signs. It is possible that increased awareness of delirium among nurses prompted an increase in delirium detection leading to more CAM+ scores in the rooms with the sign. The delirium sign may prompt nurses to be on higher alert for acute changes in confusion and mental status while delivering non-pharmacological interventions. Early identification of delirium is important as it leads to further workup, consultation and management.28 On this unit a CAM+ score prompts a number of interventions including initiation of a delirium order set, additional blood work for potential causes and geriatric medicine consultation. If the sign increases delirium detection by raising awareness, it may have a positive impact on patients who may have had a delayed or missed diagnosis.
Based on the results of the staff surveys, the sign was well received by nurses and allied health staff who play an important role in delirium identification and prevention for hospitalised patients. Tools that decrease cognitive load for staff are important given the pressing need to manage, recall and prioritise information in fast-paced healthcare environments.29 Tools that promote non-pharmacological interventions for delirium may be particularly important during the COVID-19 pandemic, given the increased risk for delirium due to the disease itself and as a result of isolation from visitor restrictions.30 It is vital that resources to assist healthcare workers with delivering delirium prevention interventions are available at the bedside or built into EMR, order sets and protocols.31 Equally important, family members need to be engaged as essential care partners who may be able to assist healthcare providers in instituting effective non-pharmacological approaches for delirium prevention. Our bedside sign has the potential to be completed and used by family members who felt that it was helpful for communication and easy to understand. As high patient to staffing ratios can often limit family engagement,32 the sign can also be used as a tool to involve family members with minimal increased effort on the part of staff.
We were able to successfully implement a bedside delirium prevention sign on a busy orthopaedic unit. It is possible that the sign increases awareness and recognition of delirium, which may have an impact on health outcomes for hospitalised older adults. For future directions, delirium prevalence will be defined using more rigorous chart abstraction methods and the sign will be further updated based on staff and family feedback. Our plan is to improve these elements on this orthopaedic unit first and then consider expansion to other units or hospitals.
Acknowledgments
We would like to thank all the nurses and allied health staff on unit E2 at the Juravinski hospital, and in particular Unit Clinical Manager Mary-Lou Meyers.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CR-R led the study and prepared initial draft of this manuscript. SS played a key role in the preparation of the manuscript and analysis of data. CG collected data on sign completion rates. CM provided staff training and disseminated staff surveys. EK-CW contributed the graphic design expertise to create the sign. CR-R, SS, EK-CW, JYL, CG, AC, YK, CM, SDF, KE and CP were part of the quality improvement team that designed the sign, interpreted data and discussed change ideas. All authors critically revised the draft, gave final approval of the version to be published and are accountable for all aspects of the work.
Funding This project was supported by a grant from Regional Geriatrics Program Central (Specialised Geriatrics Services Quality Improvement Grant). This project also received in-kind support from Hamilton Health Sciences-E2 unit in the form of logistical support and funding to print the signs.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the Hamilton Integrated Research Ethics Board (#3447).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.