Article Text

Abstract
Background Postpartum haemorrhage (PPH) contributes to substantial maternal morbidity. Research into PPH has led to improvements in care which have been incorporated into the Obstetric Bleeding Strategy for Wales.
Intervention A national quality improvement team supported local teams in implementing multiple interventions including risk assessment, objective measurement of blood loss, multiprofessional assessment (at the bedside at 1000 mL blood loss) and point-of-care (POC) testing of coagulation to guide blood product resuscitation during PPH. The project was rolled out to all 12 obstetric units in 2017. The interventions were reinforced by an All Wales Guideline, PPH proforma and standardised training. A national database, biannual audits, and patient and staff surveys reported process and outcome measures.
Results Process measures: during 2017, there was an increase in the percentage of maternities with documented risk assessment (0%–76%), objective measurement of blood loss (52%–88%) and POC testing for coagulation for PPH ≥1500 mL (38%–59%). Maternity staff survey indicated that 94% were aware of the project and 87% stated that it had changed their unit’s management of PPH. Interim outcome measures: the incidence (95% CI) of PPH ≥2500 mL per 1000 maternities in 2017 was 6.03 (5.23–6.95). The annual number of women receiving any red blood cell transfusion, level 3 intensive care admission and hysterectomy for PPH was 19.7 (18.2 to 21.3), 0.702 (0.464 to 1.06) and 0.255 (0.129 to 0.504) per 1000 maternities, respectively.
Conclusions A high level of project awareness across Welsh maternity units has been achieved. Measurement of blood loss was reported to be the most important early change in practice, while PPH documentation and POC testing continue to be embedded. Combining qualitative and quantitative measures to inform implementation has improved project delivery and allowed teams to adapt to local contexts.
- healthcare quality improvement
- obstetrics and gynecology
- teamwork
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Problem description
Postpartum haemorrhage (PPH) is the leading cause of maternal mortality worldwide,1 and was responsible for 18% of direct maternal deaths in the UK (2014–2016).2 The Scottish Maternal Morbidity Enquiry recorded an increase in the incidence of major obstetric haemorrhage from 3 to 6 per 1000 deliveries (2006–2012), with PPH contributing to 80% of severe maternal morbidity.3 This morbidity may be prolonged and impact on the newborn child and wider family.4 Within Wales, the maternity network identified PPH as one of the top five priorities for all health boards in 2015.
Available knowledge
PPH is defined by The Royal College of Obstetrics and Gynaecology (RCOG) in the UK as a blood loss of ≥500 mL within 24 hours of vaginal delivery, or ≥1000 mL after caesarean delivery, while severe (>2000 mL) and massive PPH (>2500 mL) are described regardless of mode of birth.1 Appropriate management of PPH requires an effective multiprofessional team comprising midwives, obstetricians, anaesthetists and haematologists to promptly recognise abnormal bleeding and undertake specialist intervention with appropriate use of medication, surgical techniques and blood products. RCOG published comprehensive guidance advocating this approach in 2016,5 yet there remains wide variation in the incidence and management of PPH across the UK.2 6 7
A programme of research into PPH has been undertaken at the University Hospital of Wales, Cardiff and Cardiff University since 2010.8–12 Observational data collected during the research showed a reduction in the incidence of PPH of >2500 mL by 60%, the use of blood products by 30%, and a fall in hysterectomies and intensive care unit admissions from PPH.12 Although the research focused on point-of-care (POC) clotting tests and the role of fibrinogen in obstetric bleeding, the improvement in morbidity outcomes was observed for all women who had suffered PPH, indicating that the improvements could not be explained solely by the effect of early fibrinogen concentrate administered to mothers within a randomised controlled trial.10 It was felt that in order to facilitate trial recruitment and in a change from previous management, the following steps were being routinely undertaken:
Risk assessment of every woman to plan delivery location and management of the third stage.5
Cumulative measurement of all blood loss.
Escalation of care to ensure multiprofessional clinical review (obstetrician, anaesthetist and senior midwife) at 1000 mL blood loss.
Bedside assessment of coagulation, haemoglobin and lactate.
The bedside blood results were used to inform patient resuscitation and administration of blood products using an evidence-based algorithm,12 and tranexamic acid was given by 1000 mL blood loss.13 Measurement of blood loss (using graduated containers and gravimetric measurement of blood-soaked swabs and pads) was integrated into routine practice to standardise study recruitment (which depended on PPH volume),14–17 although measurement of blood loss as a single intervention has been shown not to improve maternal outcomes in PPH.18 To be clinically useful blood volume lost must be reported in real time,19 therefore cumulative, measured blood loss was integrated into an escalation policy (based on the speed and volume of bleeding, with recognition of the potential for concealed haemorrhage).20
Clinical pathways can improve healthcare outcomes.21 Similar themes of risk assessment, measured blood loss and multiprofessional working have been employed by several PPH quality improvement initiatives in the USA.22 23 These projects advocate empirical blood and blood product resuscitation rather than POC-directed administration. In California, this approach led to a 27% reduction in total number of blood products used,24 25 while Bingham et al described an 18-month project which did not impact on outcomes.26
Baseline data
Following extensive discussion between all clinicians involved in maternity care at meetings across Wales (facilitated by the Maternity Network Wales, the Society of Welsh Obstetricians and Gynaecologists and the South Wales Obstetric Anaesthetic Forum) it became apparent that the rates of hysterectomy, intensive care admission and blood transfusion varied widely across the 12 obstetric units (OUs). Similar variation had been observed previously in Scottish maternity units.3 An All Wales PPH management strategy was therefore developed called the Obstetric Bleeding Strategy for Wales (OBS Cymru) with a successful grant application submitted to the Welsh Government.
Specific aims
The aim of OBS Cymru was to improve outcomes and reduce variation in severe PPH rates for all modes of birth across Wales, by implementing a standardised PPH pathway. This approach also aligned practice with the prudent healthcare agenda published by the Welsh Government.27 Specific outcome measures included:
Blood product transfusion.
Level 3 intensive care admission.
Hysterectomy due to PPH.
Massive PPH (>2500 mL).
Methods
Context
Wales has a population of 3.1 million with approximately 31 000 maternities per annum. Women have the choice to give birth in an OU, an adjacent or free-standing midwifery-led unit or at home. The smallest maternity unit has a birth rate of around 500 per year, there are seven units of approximately 2000 births per annum, three units of 4000 and one tertiary referral unit that has a birth rate of 6000. The units vary in staffing levels, case mix and structures of the clinical teams. In 2017–2018, the rate of induction of labour was 33.8%, while 63.5% of mothers gave birth vaginally without assistance, 9.8% had an instrumental delivery, 13% had an elective caesarean and 13.7% had an emergency caesarean.28
Funding
Initial funding via an Efficiency Through Technology Fund (Welsh Government) was augmented by support from 1000 Lives Improvement and Werfen (industry partner who manufactures POC ROTEM Sigma device (Werfen, Barcelona, Spain)).
Project organisation
Project board
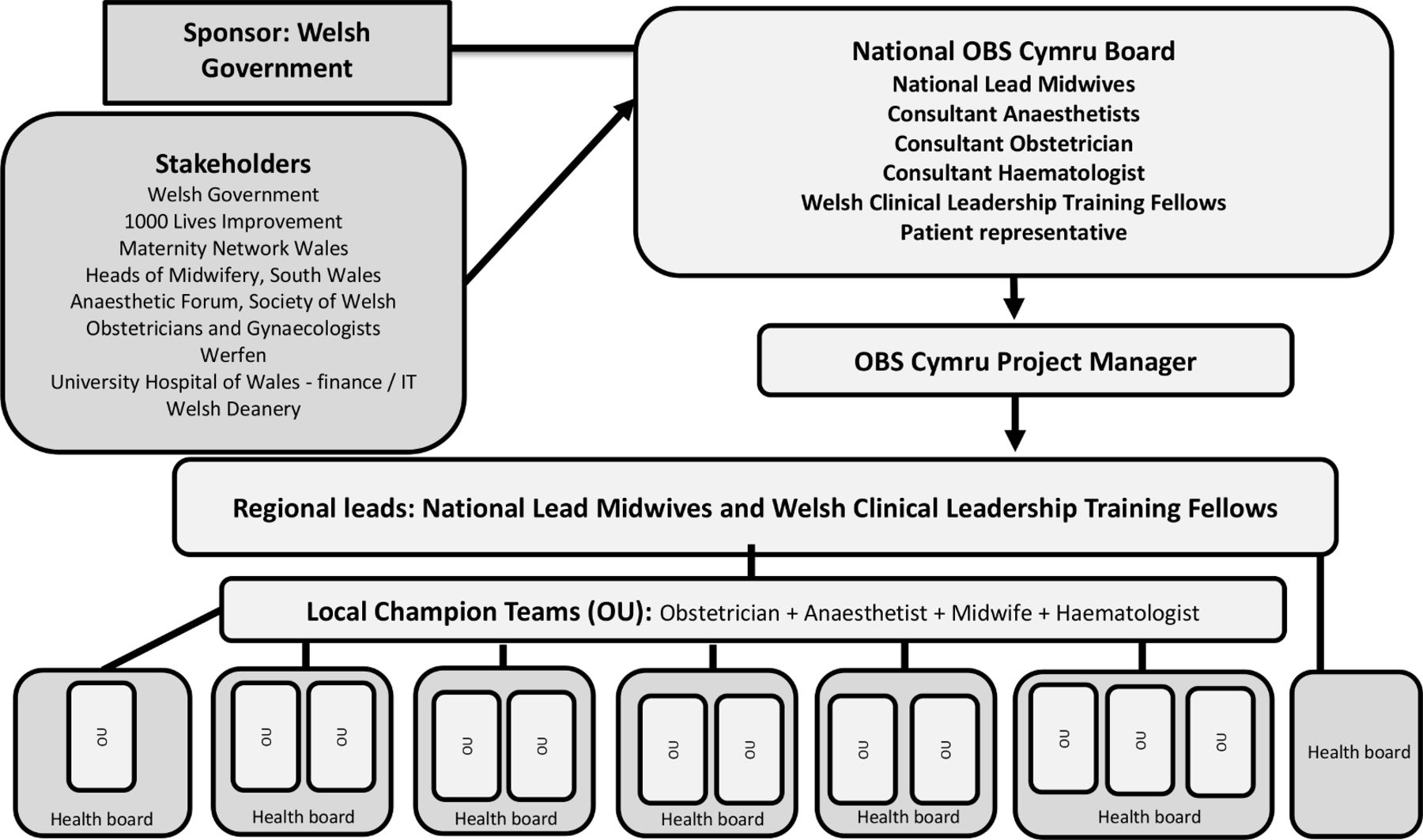
The lead applicants (RC and SFB) on the Welsh Government grant set up a national project board which included a patient and a lay representative, two senior midwives employed by 1000 Lives (working as one full-time equivalent), midwifery representation from The Maternity Network Wales, Welsh Clinical Leadership Fellows funded by Welsh Deanery (two full-time fellows per year), a consultant obstetrician, a consultant haematologist and consultant anaesthetists (figure 1). Administrative support was provided through 1000 Lives Improvement, including data analysis figure 1.
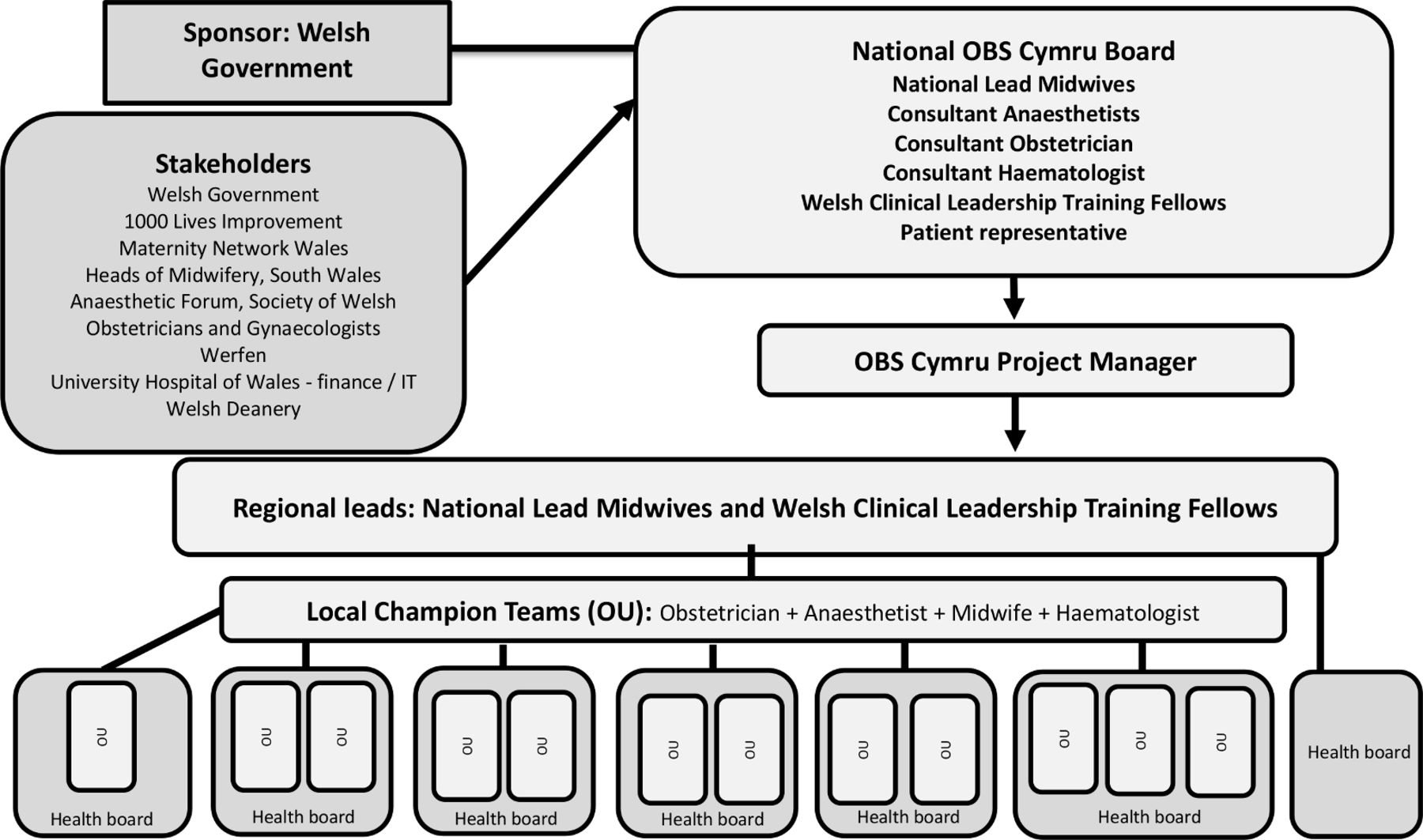
Schematic representation of the Obstetric Bleeding Strategy for Wales (OBS Cymru) organisation. OU, obstetric unit.
The project board provided strategic leadership and monitored the introduction and uptake of the project. The board produced an identifiable project brand: ‘Obstetric Bleeding Strategy for Wales - OBS Cymru’, with bilingual (English and Welsh) patient and professional facing publicity material. Project information was provided via a website, quarterly newsletters, social media and brief ‘Situation, Background, Assessment, Recommendation’ communications for urgent information. After a national launch in November 2016, annual national meetings provided opportunities for local champion teams to consolidate their training, share experiences and discuss barriers to implementation. Annual site visits were undertaken to understand the context of each OU and help inform local changes. Training was provided on all aspects of the project at regional and local study days and governance sessions.
Regional leads
The regional leads (Welsh Clinical Leadership Fellow or senior midwife) were part of the national project board and were each assigned to two to three OUs based on geographical location. Their responsibility was to support the creation of local champion teams consisting of a local midwife, obstetrician, anaesthetist and haematologist to lead the project in each OU. The regional leads maintained contact with the local champion teams, providing regular updates and support with training on all aspects of the project, including quality improvement skills. The frequency of support was front-loaded during the first year of the project.
Local champion teams
The local champion teams provided role-specific cascade training to their local team (including obstetricians, midwives, anaesthetists, haematologists and theatre teams). The local champion midwifery role was funded for 3.7 hours per week through the grant, while consultants contributed through their supporting professional activity time.
Project development and support
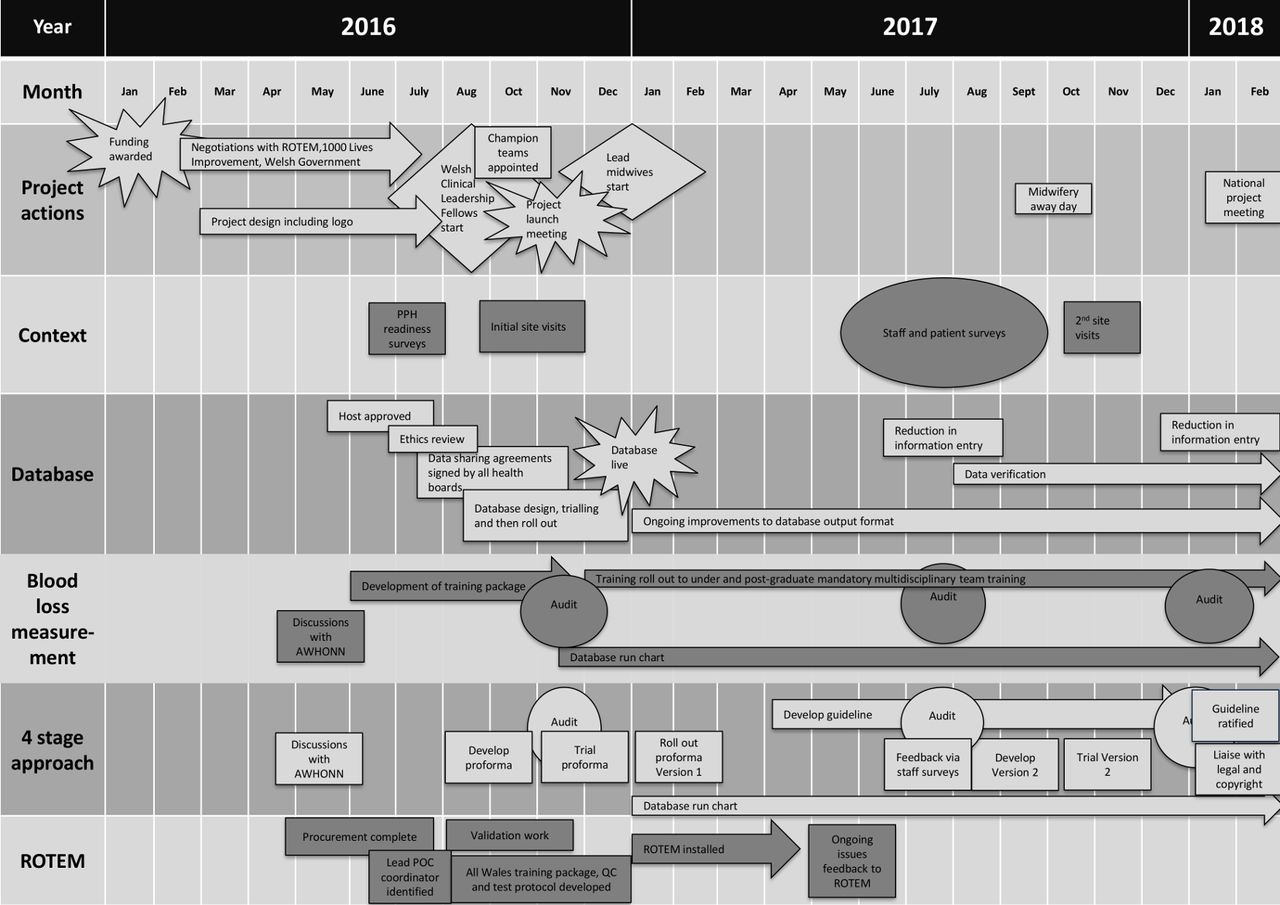
The project was designed to be delivered over 3 years. The initial 5 months (August–December 2016) were used for planning and development prior to a phased introduction of the interventions over the first 3 months of the implementation period (January–March 2017). Driver diagram and Gantt charts were developed to guide project progress. (figure 2, online supplementary appendix 1). The impact of project interventions was assessed according to Medical Research Council guidance.29
Supplemental material

Gantt chart depicting the Obstetric Bleeding Strategy for Wales (OBS Cymru) implementation. POC, point of care; PPH, postpartum haemorrhage.
OBS Cymru intervention
The project has four key themes described as ‘The 4- stage approach’:
Formal risk assessment.
Cumulative objective measurement of blood loss after every delivery to facilitate timely and appropriate escalation of care.
Multiprofessional working with a senior midwife, obstetrician and anaesthetist attending the mother at 1000 mL blood loss, or earlier for clinical concern, to enable early obstetric interventions to control bleeding, optimise resuscitation and ensure blood sampling for POC tests of coagulation, haemoglobin and lactate.
POC-guided, individualised blood product replacement supported by an algorithm developed from previous research10 30 (see online supplementary appendix 2).
Supplemental material
These themes were embedded into clinical practice, using several strategies:
A paper proforma that facilitates the four-stage approach (see online supplementary appendix 3) was developed for use in all women in labour. The proforma prompts escalation to appropriate clinicians, reinforces PPH management and standardises documentation. It includes risk assessment and obstetric interventions based on RCOG guidance.5
A national measurement of blood loss training package was developed. This included an educational video (developed in conjunction with The Association of Women's Health, Obstetric and Neonatal Nurses (AWHONN)) and a scripted simulation session. The national team developed education sessions for all undergraduate midwifery courses in Wales.
Multiprofessional teamworking and escalation was reinforced with drills incorporating OBS Cymru interventions. The practice was integrated into mandatory training.
A POC algorithm for blood clotting based on ROTEM sigma was developed based on previous research. Automated ROTEM sigma devices were installed into each OU between January 2017 and April 2017. The project provided a device with consumables for each OU with appropriate training in maintenance and test interpretation.
The four-stage approach and ROTEM sigma algorithm were incorporated into an All Wales PPH Guideline.31
Supplemental material
All Wales quality improvement registration and data sharing approval
OBS Cymru was supported by the national quality improvement organisation for National Health Service (NHS) Wales (1000 Lives Improvement Wales). The research and development department at Cardiff and Vale University Health Board confirmed the project was a quality improvement initiative. Each Health Board established a data sharing agreement supporting national data collection and sharing.
Data collection
A custom-built national database, developed by 1000 Lives Improvement Wales, was introduced to record real-time outcome and process measure data. This was launched in January 2017 and captured all PPH episodes of ≥1000 mL across Wales. Data were inputted by local champion teams with data verification performed by the national project team. The database interface provided both funnel plots and run charts to enable local units to track change and benchmark against all Wales data. Biannual audits were used to collect process measures including measurement of blood loss, presence of the paperwork in the mother’s notes and the use of the risk assessment on admission in labour. Annual staff and patient surveys informed mechanisms of project uptake.
Data analysis
Data were analysed using Microsoft Excel (Redmond, USA). Binomial CIs were calculated using the Hmisc R library V.4.2.0 implementation of the Wilson method.32
Results
The timescales of the interventions are described in figure 2.
Context
Preproject baseline survey
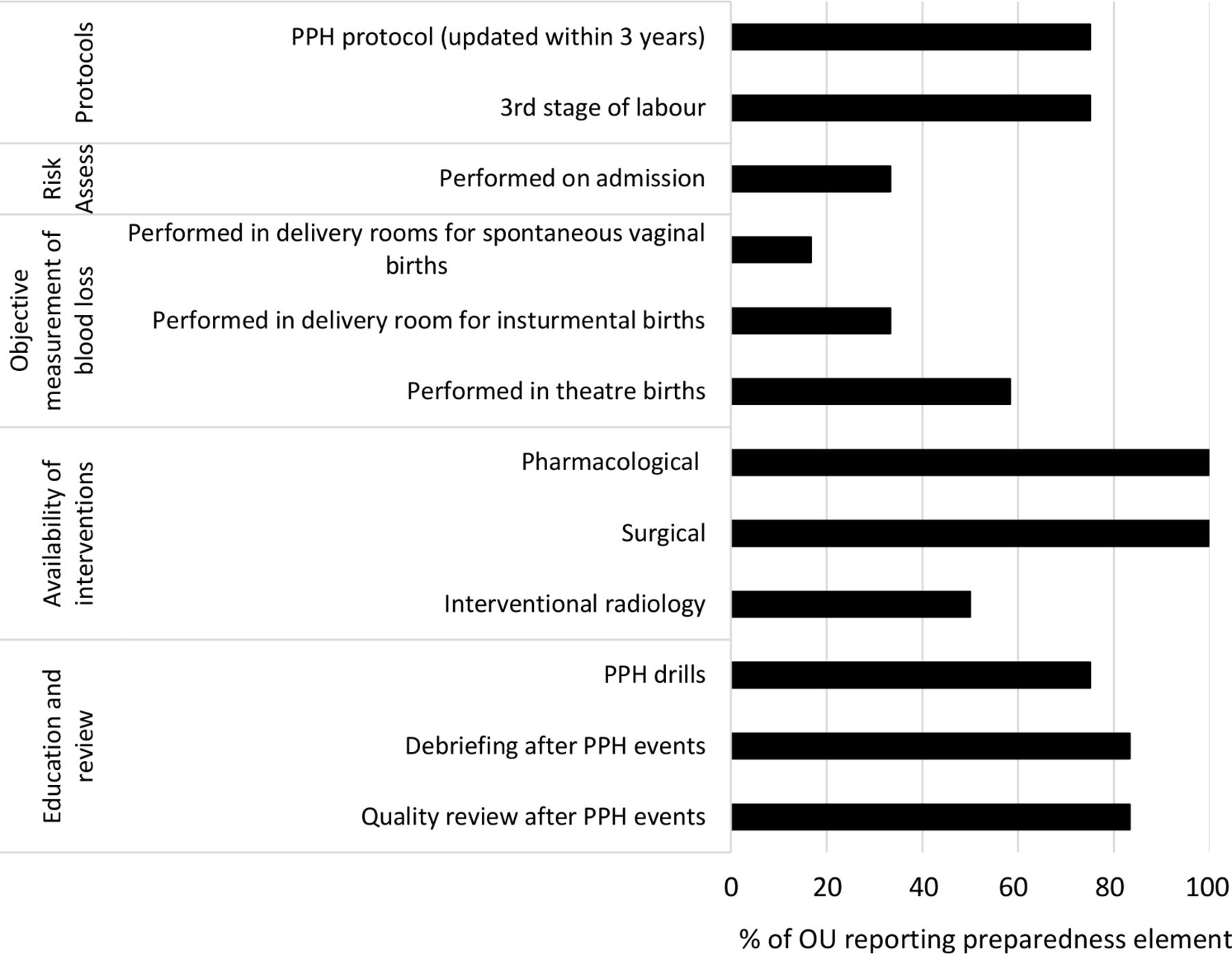
A 37-question self-assessment survey was completed by lead clinicians (and or teams) in each OU prior to project launch.33 The document assessed general confidence in readiness to manage a PPH (score 1–5) and objective elements of PPH management (weighted score, maximum 100 points). The median (range) reported confidence in readiness to manage a PPH was 4 (3–5), while median objective weighted score was 70 (40–79). A summary of the objective elements of PPH management is shown in figure 3. This showed that although most units felt they had a high degree of readiness for PPH management, there was a large variation in what was considered key elements and no units had them all in place at the beginning of the project.

Summary of objective elements of postpartum haemorrhage (PPH) management reported by all 12 obstetric units (OUs).
Site visits
Formal project visits were repeated annually by representatives of the national project team, with qualitative summaries then shared with the local teams. These described the strengths and challenges of a unit when dealing with PPH in terms of communication (eg, escalation pathways), task factors (eg, use of massive haemorrhage protocol), site (eg, locality of delivery suite), team (eg, availability), patient factors (including complexity), education/training (including multiprofessional training), equipment/resources, working conditions (eg, timing of PPH events) and organisational factors (eg, governance structures). The visits highlighted local barriers to improvement, such as a lack of equipment (eg, weighing scales). These issues were escalated to and resolved by local management.
Understanding uptake of interventions
Staff survey
A staff survey was circulated to all 12 OUs in July 2017 (7 months after start). All staff groups were represented in the 272 returned surveys (midwives (50%, 137/272), obstetricians (14%, 37/272), anaesthetists (19%, 53/272) and theatre staff (15%, 40/272), with a median (range) number of surveys received per OU of 20.5 (12–34). The percentage of respondents aware of the principles of OBS Cymru was 94% (256/272), with 87% (236/272) reporting a change in their unit’s practice of PPH management as a result of the project. Measurement of blood loss was thought to have contributed to the change by 79% (216/272) respondents, while POC, the four-stage approach and teamworking had contributed by 53% (143/272), 47% (127/272) and 41% (112/272), respectively. Training had been received by 63% (172/272) with additional training requested by 65% (177/272). Barriers to implementation included training, staff and time constraints, and teamworking. Local data were fed back to inform ongoing focused project development.
Patient survey
An experience survey was circulated to mothers who had a PPH >1000 mL in September 2017. Analysis of 37 responses from five OUs found that 95% (35/37) of women felt well supported by staff during their PPH. Three women suggested improvements in care that included communication, particularly with the birthing partner. This information was fed back to teams and integrated into training sessions.
Interventions
Process measures
Measurement of blood loss
Several strategies were used to understand uptake of measurement of blood loss in clinical practice:
Reach and dose
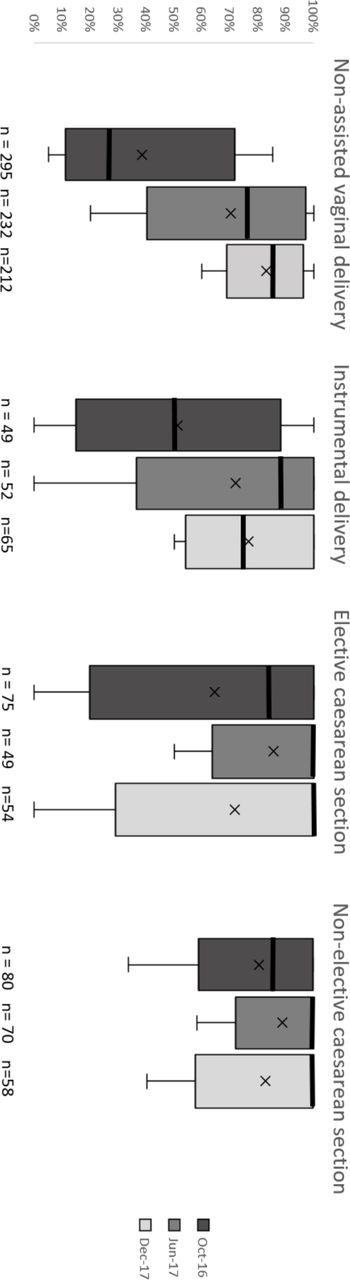
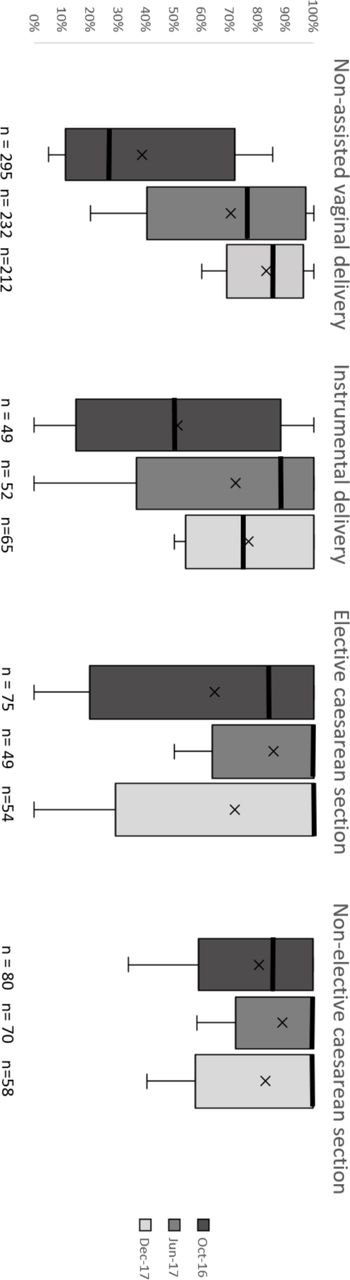
Prospective audit cycles of consecutive deliveries occurring during a single week were conducted biannually in OUs. Data were obtained from the maternity notes and included mode and place of delivery, blood loss volume, type of blood collection equipment and whether all blood loss was measured. Objective measurement of blood loss increased from 51% (260/511) to 88% (356/405) of all maternities (not just those deliveries where there was a PPH). Measurement of blood loss for all modes of delivery is shown in figure 4.
Continuous data were collected for all PPHs (>1000 mL) as part of a national OBS Cymru database from January 2017 onwards, indicating whether the intervention was being adopted for all PPH events. Monthly recorded measurement of blood loss in the database increased from 77% (166/215) in January 2017 to 89% (205/230) in December 2017. A run chart of weekly measurement is illustrated in online supplementary appendix 4.
Fidelity
A standardised training package was delivered at the national launch event and reproduced at local multiprofessional training sessions by local teams.
Staff survey
Of the staff involved in measurement of blood loss, 63% (132/209) had received training and 93% (194/209) felt confident undertaking the task.
Supplemental material
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box and whisker plots to describe % of mothers in each obstetric unit (OU) with measured (vs estimated) blood loss for different modes of delivery in sequential audit cycles. Median, mean, IQR and range are illustrated. Data for elective caesarean sections in December 2017 are skewed by one elective caesarean section occurring in a single OU in which the blood loss was estimated.
Four-stage approach to managing PPH
The phased introduction of the paperwork into clinical practice included a draft design followed by small-scale trial use in each unit prior to roll-out in January 2017. Uptake was described using:
Reach and dose
Two audit cycles in 2017 showed the presence of the paperwork in all maternity notes increased from 0% to 83% (336/405) of women and completion of the risk assessment increased from 0% to 76% (308/405) of women.
The OBS Cymru database recorded completion of the risk assessment in cases of PPH. The accuracy of these data was limited by difficulties in accessing patient notes to ascertain completion, with only 33% (505/1521) of episodes in the second half of 2017 having this information recorded. Where the information was available, 79% (399/505) had a risk assessment completed, use of the four-stage paperwork was recorded in 47% (771/1521) episodes and 65% (503/771) had had it completed.
Fidelity
Regional leads delivered training to local champion teams who then cascaded to the local multiprofessional team.
No data were recorded regarding the impact of the paperwork on review of PPH events or documentation.
Staff survey
Of respondents 49% (132/272) had used the paperwork and 60% (165/272) supported it replacing prior PPH documentation. The survey identified multiple improvements that were required in the four-stage proforma (including simplification and flow), which were incorporated into a revised version. This was circulated for additional trial and comment prior to release in January 2018 (see online supplementary appendix 3) and incorporation into the All Wales PPH Guideline.
Use of POC testing for coagulation
POC testing of coagulation (ROTEM sigma) was indicated for bleeds >1000 mL with ongoing bleeding or earlier for clinical concern. ROTEM sigma devices were installed between January and April 2017 into 10 OUs (two sites had them installed prior to the project but adopted the OBS Cymru protocol in 2017). A training package was developed in conjunction with a national lead POC testing manager to ensure standardisation of training and testing across sites. The training was cascaded by local POC testing managers, supported by the national team. Internal quality control (QC) systems were adhered to. All units were enrolled into the National External Quality Assurance Scheme by 2018. The use of POC coagulation testing across Wales was assessed using information from the OBS Cymru database:
Reach and dose
Four hundred and ninety ROTEM tests were performed on 26% women (369/1448 database episodes) in the first half of 2017 compared with 685 ROTEM tests on 38% of women (583/1521) in the second 6 months of 2017.
Of the women who had a PPH >1500 mL, 38% (206/547) had a ROTEM test performed in the first half of 2017 compared with 59% (346/588) in the second 6 months of 2017.
The number of women who had repeat tests as per protocol was not recorded in the national database.
Fidelity
Use of ROTEM to guide blood product management was informed by the database linking test results to patient transfusion but was limited by a lack of information around when bleeding stopped.
In the first 6 months of 2017, 40 women received Fresh frozen plasma (FFP) or fibrinogen concentrate, of which 53% (21/40) had ROTEM tests performed. In the second 6 months, 30 women received coagulation products and all of them had a ROTEM test performed.
Staff survey
Of respondents, 92% (249/272) were aware that they had a ROTEM device on their unit; 49% (133/272) had received training and the most commonly requested additional training was for the ROTEM (81%, 144/177).
Outcome measures
Full outcome measures will be published following completion of the project and data analysis. Data from 2017 led to a better understanding of the incidence of PPH. Of the 31 341 maternities in 2017, 2969 episodes were entered into the database with 2868/2969 (96.6%) having blood loss >1000 mL. The median (IQR) blood loss for women entered on to the database was 1339 mL (1123–1700), with a maximum loss of 7806 mL. The incidence (95% CI) of PPH >2500 mL in Wales was 6.03 (5.23 to 6.95) with a median (IQR, range) per OU of 7.8 (3.6 to 9.0, 2.6 to 9.9). The incidence of >1000 mL and >2000 mL has been published previously.34 Additional outcome data for 2017 are described in table 1.
All Wales PPH outcome indicators per 1000 maternities in 2017 (data extracted from the Obstetric Bleeding Strategy for Wales (OBS Cymru) database, 25 June 2019)
Discussion
The OBS Cymru PPH management strategy was adopted by all 12 OUs in Wales. A high level of project awareness was achieved early in the implementation phase across all sites and professional groups. We believe this was a crucial step in changing practice and was accomplished by local and national teams communicating effectively and receiving the support of multiple stakeholders.
Local teams were encouraged to adapt OBS Cymru to the needs of their local contexts, allowing them to take ownership of the project. In addition, the development of local and national interprofessional networks allowed shared learning and maintained enthusiasm.35 The provision of time and resources (including quality improvement training, data interpretation and feedback) across professional groups was essential in ensuring rapid adoption of OBS Cymru.36
Quantitative assessment of process measures showed changes in practice, while qualitative data were used to describe the potential mechanisms of these changes and how implementation differed across sites. This in turn allowed OBS Cymru to be adapted and refined during implementation.
An early staff survey indicated that the project had led to a change in PPH care, with measurement of blood loss accepted as routine practice. Use of the four-stage approach proforma and ROTEM increased over the first year with further refinement of the paperwork and ROTEM education required. To address the need for additional team training, the national team collaborated with the national Practical Obstetric Multidisciplinary Training course,37 to align the content of both initiatives and further embed the OBS Cymru approach.
The lack of a unified maternity database in the Wales database presented a significant barrier to data collection. A bespoke, cross-site, national database was therefore created to measure process and outcome change and allow local units to monitor their progress and benchmark against others. The data collection resulted in duplication of data entry into local and project databases. The national project team have therefore been working with stakeholders to explore embedding quality markers into national statistics. The initial data set was also recognised as being too comprehensive, creating a significant time burden for data entry and reducing the time available to deliver local training and quality improvement. The data requirements were therefore stratified depending on the severity of the PPH following feedback from local teams.
The outcome measures chosen to describe OBS Cymru are relevant to mothers and maternity providers. They reflect bleed severity, blood transfusion, maternal separation from her newborn child (during level 3 critical care admission) and long-term fertility implications following hysterectomy. During project implementation, both hysterectomy and level 3 intensive care admissions were recognised as infrequent and sentinel events and although every such event must be reviewed, and lessons learnt, these measures are not useful to inform day-to-day changes in practice. More common indicators that describe effective PPH care include rates of 1000 mL PPH (and progression to larger bleeds) and blood transfusion rates were found to be more important to measure change of practice in the Quality Improvement project.
It is anticipated that the national scale of the data collection will facilitate substantial PPH learning. Recognition of the increased incidence of 1000 mL PPH, when blood loss is measured as opposed to estimated, will have implications for service users and researchers on an international scale.38–41
Future reports and research
The key themes for sustainability (guided by the NHS Improvement Sustainability Model),42 and achievements (including outcome data) will be described in subsequent publications. The paucity of data regarding cost analysis of POC tests of coagulation in PPH has been identified by NICE guidance,39 and we will therefore perform a cost analysis following project completion. Furthermore, the variation in effectiveness of local leaders across sites,43 and the impact of the adoption of OBS Cymru into community and midwifery-led settings in 2018 is yet to be described.
OBS Cymru was designed as a national quality improvement project. All OUs implemented the intervention and so there was no control arm for comparison. A future cluster randomised control trial would be required to further understand the impact of the OBS Cymru complex intervention.
Conclusions
OBS Cymru is a quality improvement collaboration which has been implemented into all 12 OUs in Wales. High levels of project awareness was achieved by both local and national multiprofessional leaders engaging and empowering local maternity staff. Communication networks within and between units enabled shared learning across sites. Using both quantitative and qualitative measures to understand impact and mechanisms of change allowed project delivery to be adapted to local contexts and needs; an approach relevant to all expanding quality improvement initiatives. Measurement of blood loss was the most important early change in practice, while ROTEM use, PPH documentation and team training continues to be embedded. The nationally agreed data set has improved understanding of PPH care, with the aim of improving outcomes and reducing variation across Wales. The early adoption of the OBS Cymru approach across 12 OU of different sizes and staffing structures demonstrates applicability of the approach across a wide variety of NHS settings.
Acknowledgments
The authors thank all the staff working in maternity services across Wales who have engaged with OBS Cymru.
References
Footnotes
Contributors SFB, holds the grant from the Welsh Government, devised and leads OBS Cymru, designed the analysis, interpreted data and wrote the first draft of the manuscript. AW, analysed and interpreted the data and critically reviewed the manuscript. MJ, EM, TK, CS, CB, KK, KJ collected and interpreted the data and critically reviewed the manuscript. TE collected the data, interpreted data. IV, NS, CF, KG JT, PC analysed the data, interpreted data and critically reviewed the manuscript. RC holds the grant from the Welsh Government, devised and leads OBS Cymru, collected the data, interpreted data and critically reviewed the manuscript.
Funding This study was funded by 1000 Lives Improvement Wales, NHS Wales (Efficiency Through Technology Fund) and Werfen.
Competing interests PC has received support for research from CSL Behring and Haemonetics. He has acted as a paid consultant to Werfen and Haemonetics. RC has received support for research from CSL Behring.
Patient and public involvement Patients and/or the public were involved in the design, conduct, reporting and dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.