Article Text

Abstract
Background Unintended shocks from implantable cardioverter defibrillators (ICDs) are often distressing to patients and family members, particularly at the end of life. Unfortunately, a large proportion of ICDs remain active at the time of death among do not resuscitate (DNR) and comfort care patients.
Methods We designed standardised teaching sessions for providers and implemented a novel decision tool in the electronic medical record (EMR) to improve the frequency of discussions surrounding ICD deactivation over a 6-month period. The intended population was patients on inpatient medicine and cardiology services made DNR and/or comfort care. These rates were compared with retrospective data from 6 months prior to our interventions.
Results After our interventions, the rates of discussions regarding deactivation of ICDs improved from 50% to 93% in comfort care patients and from 32% to 70% in DNR patients. The rates of deactivated ICDs improved from 45% to 73% in comfort care patients and from 29% to 40% in DNR patients.
Conclusion Standardised education of healthcare providers and decision support tools and reminders in the EMR system are effective ways to increase awareness, discussion and deactivation of ICDs in comfort care and DNR patients.
- standards of care
- quality improvement
- patient preference
- patient-centred care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Implantable cardioverter defibrillator (ICD) shocks can be traumatic for patients and families, particularly at the end of life.1 2 Retrospective studies estimate that between 51% and 65% of ICDs remain active at the time of death.3 4 Given the high risk of malignant arrhythmias in this patient population, up to 24%–33% of patients receive shocks within the last 24 hours of life, and 7%–14% receive shocks in the last hour of life.5
As patients age or progress in their illness severity, ICD shocks may no longer be welcomed. Accordingly, the Heart Rhythm Society guidelines state that physicians are obligated to have a conversation about whether a patient’s device therapy is in line with his or her goals of care, particularly whenever there is a change in code status.6 While studies show that physicians believe they should engage in these types of conversations with patients, they rarely do.7 8 Commonly reported barriers include lack of experience in holding these discussions and lack of knowledge that any official guidelines exist.7–9
We performed a 6-month retrospective chart review on admitted patients made ‘do not resuscitate’ (DNR) and/or comfort care with active ICDs at our institution. Discussions surrounding ICD deactivation or device deactivation occurred in only 50% of patients made comfort care and only 32% of patients made DNR. In line with published guidelines, we designed a quality improvement project to prevent unwanted ICD shocks in patients. Our aim was to increase the percentage of discussions regarding ICD deactivation by 10% in both the comfort care and DNR cohorts over a 6-month study period. Our hypothesis was that through education sessions and decision support tools in the electronic medical record (EMR), we would achieve this aim.
Methods
A resident-led improvement team used the model for improvement to design a project charter aimed at increasing patient engagement and provider awareness around ICD deactivation during discussions about DNR and comfort care status. Adult patients aged 18 years and older admitted to teaching and non-teaching services on the general medicine, cardiology or intensive care units (ICUs) with active ICDs were included. Patients admitted to other hospital services or admitted with already deactivated ICDs were excluded from analysis. Active ICD status was established based on the most recent device interrogation as documented by a licensed electrophysiologist (attending or nurse practitioner).
Prior to any interventions, a retrospective review was performed on patients made DNR and comfort care while admitted to medicine services at NewYork-Presbyterian (NYP) Hospital/Weill Cornell Medical Centre (New York, New York) from 1 December 2017 to 30 May 2018. This was followed by a 2-month project design period. The improvement team identified areas for improvement using process maps and driver diagrams around code status, comfort care discussions and hospital protocol for deactivating ICDs. Change ideas were developed for targeted intervention to test from 1 August 2018 through 31 January 2019. During this 6-month period, weekly plan–do–study–act (PDSA) cycles were performed to adjust the frontline workflow as needed. Every Friday, a Microsoft Excel spreadsheet, containing all patients who were made DNR and comfort care during the week prior, was sent to us from the NYP Analytics department. We chart reviewed this list of patients to filter those admitted with active ICDs. Alerts of comfort care or DNR patients resulted only after death or discharge.
Interventions
We designed 10-minute standardised lectures for residents, fellows and physician assistants, and assessed knowledge using pre-education and post-education surveys (weeks 1–6). Surveys were administered immediately prior to and after these education sessions. (Survey questions and answers can be found in online supplementary appendix A1.) The goals of these sessions were to bring awareness to the issue, to make providers comfortable with discussing ICD deactivation with their patients and to clarify hospital process and documentation for deactivation. At the 3-month mark, we readministered identical education surveys to measure retention of knowledge (weeks 13–17). On completion of the surveys, we used incorrect answers as an opportunity to briefly re-educate providers. We also had separate, one-time lectures dedicated to the cardiology fellows (week 8), nurse practitioners (week 8), hospitalists (week 16) and the hospital’s quality and patient safety officers (week 19).
Supplemental material
Our second intervention focused on EMR changes. Alerts and decision support tools were integrated into the comfort care order set (week 14) and DNR document (week 18) to alert and remind providers to document discussions and indicate consent for deactivation when indicated. For the comfort care order set, we created a hard stop titled ‘AICD Deactivation Planning’ (AICD stands for automatic implantable cardioverter defibrillator). For the DNR change, a pop-up appeared prior to opening a DNR document stating, ‘Please review whether the patient has an ICD and if so, whether or not deactivation of that device would be desired. If deactivation is desired/intended, please place an order for ICD deactivation and call cardiology as per policy’. (Details of EMR changes can be found in online supplementary appendix A2.)
After each week’s data collection, using a number generator, we selected 10 random DNR patients and 5 random comfort care patients (irrespective of ICD carrying status) and emailed the provider caring for the patient. This question was worded, ‘Q: When making your patient DNR and/or comfort care, did it cross your mind to check whether or not the patient had an ICD? (Y/N)’. The goal of this email was to generate a process measure to evaluate if, at the time of DNR or comfort care documentation, the provider was aware of the ICD status of the patient. This was used as an additional tool to track the efficacy of our interventions. Physicians were emailed within 1 week of patient discharge to minimise recall bias.
Lastly, posters were created as reminders and displayed in common workspaces and bathrooms throughout the medicine and ICU wards (weeks 20–28).
Measures
Primary outcome measures were per cent of ICD carriers made comfort care with documented ICD deactivation discussions and per cent of ICD carriers made DNR with documented ICD deactivation discussions. Process measures were per cent of ICD deactivations in comfort care and DNR patients, comparison of pre-education, post-education and retention knowledge survey responses, and provider awareness of ICD status (via weekly questionnaire directed at random providers, as stated previously). Balancing measures were any patients who underwent undesired ICD deactivations or required reactivation of the device at a later point.
Statistical analysis
Data collected from the surveys and the chart review were entered into Research Electronic Data Capture (REDCap), a secure, electronic data collection platform designed to manage data capture for research studies.10 Descriptive statistics were performed to describe the frequency of documented discussions for ICD deactivation among DNR and comfort care patients, as well as the survey results among healthcare providers. To compare pre-intervention, post-intervention and retention survey results, Fisher’s exact test and χ2 tests were performed. An alpha of 0.05 was considered as criteria for statistical significance. Our ultimate outcomes (post-intervention) were compared with these baseline values. STATA V.14 and QI chart software were used to perform the statistical analysis.
Patient and public involvement
Patients with ICDs were involved in discussions regarding their wishes for device deactivation during the 6-month study period. Outside of these discussions, patients had no other roles in the study. No active recruitment occurred; we only reviewed patients already admitted to our hospital. Patients were not asked to assess the burden of our interventions. Providers were the sole recipients of education sessions, weekly emails and EMR changes.
Results
Retrospective data from 1 December 2017 to 30 May 2018 were obtained for comparison. Among comfort care patients, only 50% (10 of 20 patients) had documented discussions and/or deactivated ICDs at the time of death or discharge. Among DNR patients, only 32% (14 of 41 patients) had documented discussions and/or deactivated ICDs at the time of death or discharge.
During our 28-week study period, in the comfort care cohort, the rate of documented discussions surrounding ICD deactivation improved from 50% to 93% (14 of 15 patients). In the DNR cohort, the rate of documented discussions surrounding ICD deactivation improved from 32% to 70% (28 of 40 patients). Concomitantly, the rates of ICD deactivation increased from 45% to 73% in the comfort care cohort and from 29% to 40% in the DNR cohort. Most importantly, zero patients received undesired shocks from their ICDs during our study. No patients experienced undesired deactivations or required reactivation of their devices at a later date. Figure 1A,B shows the run charts for the comfort care and DNR cohorts, with interventions listed along the x-axis.

Run charts. Twenty-eight-week study period for (A) comfort care cohort and (B) DNR cohort showing the documented discussion rate (solid line) and the ICD deactivation rate (dotted line). Each data point reflects the percentage of successful outcomes divided by the total number of patients up to that week of data collection. The horizontal red dotted line is to compare with the rate of documented discussions or ICD deactivations in the retrospective data prior to any interventions. Study interventions are listed along the x-axis. DNR, do not resuscitate; EMR, electronic medical record; ICD, implantable cardioverter defibrillator; NP, nurse practitioner; PA, physician assistant.
Our education sessions proved effective in helping providers feel knowledgeable and comfortable when encountering patients with active ICDs. Post-education surveys had a statistically significant improvement in correct answers as compared with pre-education surveys. Retention of knowledge surveys performed from weeks 13 to 17 proved effective in retention of knowledge. Based on Likert scale responses, providers also reported feeling more comfortable participating in conversations about ICD deactivation after our education sessions, and their reported comfort level was preserved during the retention surveys (table 1).
Survey results: percentage of correct responses for surveys administered to providers during pre-education, posteducation and the 3-month retention point
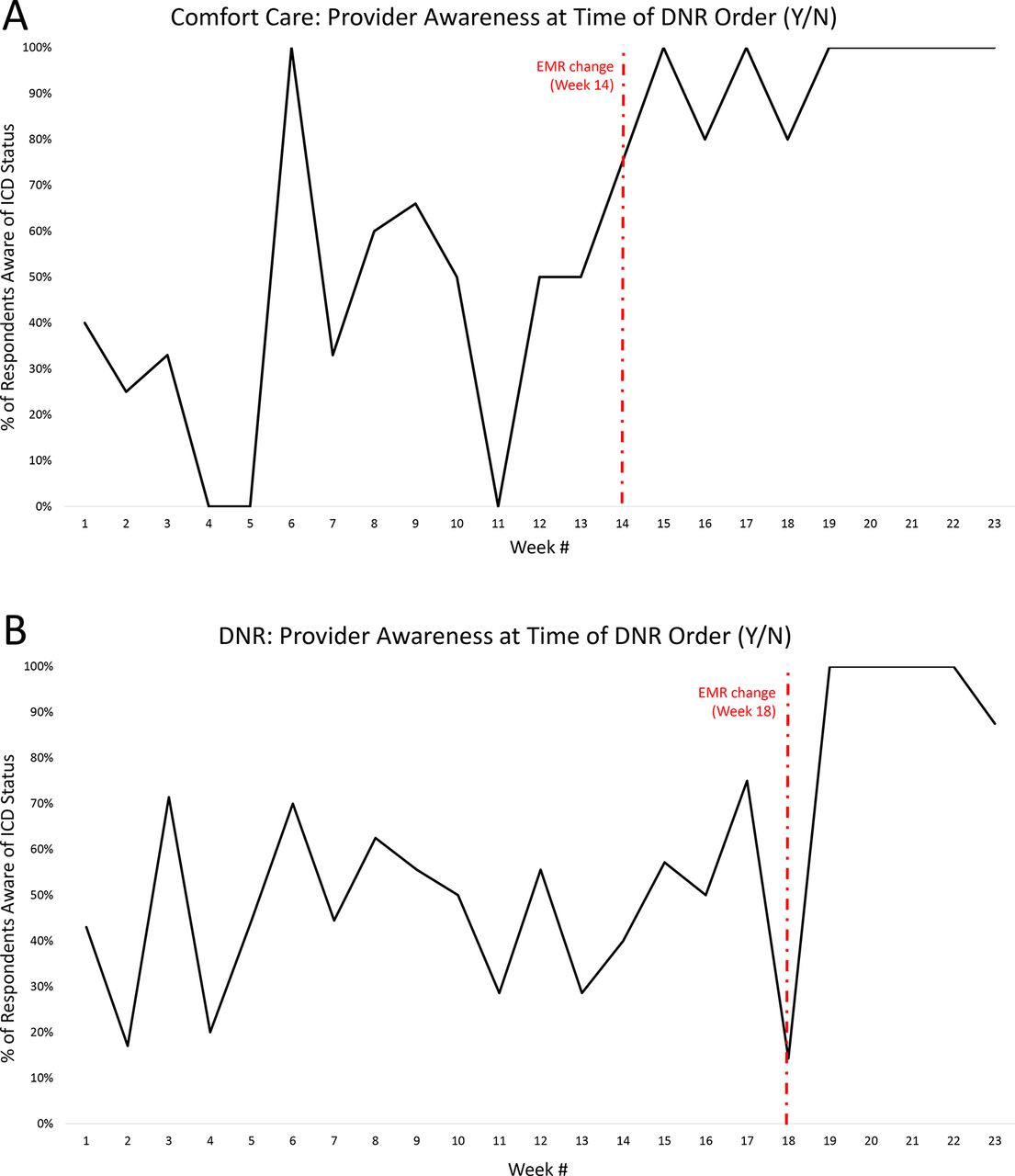
Weekly surveys targeted at providers (who entered DNR or comfort care orders during the PDSA cycle of interest) showed the most impressive and consistent changes after EMR changes (figure 2A,B). The question of interest was phrased, ‘Q: When making your patient DNR and/or comfort care, did it cross your mind to check whether or not the patient had an ICD? (Y/N)’. In the beginning, we struggled to keep providers consistently and reflexively checking ICD status when entering DNR and/or comfort care orders for their patients, as shown by the wide variation in responses. Immediately on enacting EMR changes, the majority of providers were consistently answering ‘yes’ to our question. For the comfort care cohort, providers who responded ‘Y’ were 49% (24/49) pre-EMR change vs 95% (36/38) post-EMR change (p<0.01). For the DNR cohort, providers who responded Y were 48% (63/131) pre-EMR change vs 93% (40/43) post-EMR change (p<0.01). The average overall response rate from providers was 75%. We stopped sending weekly emails at week 24 of 28 as the results were overwhelmingly positive and we did not want to burden providers.
{kind=link}
{kind=link}
Provider awareness of ICD status. Weekly survey targeting providers who entered DNR and/or comfort care orders. Ten DNR patients and five comfort care patients were selected at random using a number generator. (A) The comfort care order set was added on week 14. Providers who answered ‘Y’ were 49% (24/49) pre-EMR vs 95% (36/38) post-EMR change (p<0.01). (B) The DNR document pop-up was added on week 18. Providers who answered Y were 48% (63/131) pre-EMR vs 93% (40/43) post-EMR change (p<0.01). DNR, do not resuscitate; EMR, electronic medical record; ICD, implantable cardioverter defibrillator; N, no; Y, yes.
Discussion
With our interventions, the rates of discussions detailing patients’ wishes on ICD therapy successfully increased by 43% and by 38% in comfort care and DNR patients, respectively. The rates of ICD deactivation concomitantly improved in both cohorts. No patients received unwanted defibrillation during the study period. Education sessions were effective and successfully demonstrated retention of knowledge based on survey results. Prompting through EMR changes resulted in providers more reliably checking ICD status on patients. Our novel ‘AICD deactivation planning order set’ showed reliable, consistent use and effectiveness in reminding providers to discuss ICD deactivation in patients made DNR or comfort care.
A related project by Javaid et al used teaching sessions to increase the rate of ICD deactivation from 0% to 54% over 6 months.11 No patients received shocks during their study as well. A few notable differences exist between our two studies. First, we created EMR changes embedded within our regular workflow to make durable impact, as education alone is prone to knowledge attrition over time. Second, we performed more frequent, weekly PDSA cycles. Weekly data collection allowed us to methodically track the efficacy of our interventions by polling providers weekly, and also react immediately to missed opportunities to improve outcomes.
Another critical distinction is that our primary outcome was rates of discussions instead of ICD deactivation itself, the latter of which is typically reported in the literature. Our priority was to empower patients and providers with information to allow patients and/or surrogate decision makers to make informed and personalised decisions regarding ICD therapy. Our goal was to prevent only undesired shocks among our patients, realising that not every patient ultimately will decide to deactivate their device. We propose this as a novel, prudent and more patient-centred outcome to evaluate future studies on deactivation of ICDs at end of life. There are in fact some DNR or comfort care patients who are open to being shocked by their devices, and these instances should not be viewed as missed opportunities, as long as an informative discussion occurred.
Unsurprisingly, the rates of ICD deactivation were lower in the DNR cohort compared with the comfort care cohort. DNR patients have a wider spectrum of illness severities. While discussion about device therapy is always necessary, a shorter conversation may be adequate for a DNR patient presenting with cellulitis as compared with a patient in cardiogenic shock on cardiovascular support. Tailoring discussions is important. Providers should be cognisant of the patients most vulnerable to shocks perideath: (1) admitted for cardiac reasons, (2) anticipated to have sudden death (defined as death occurring within 1 hour of symptom onset), (3) victims of prior shocks or (4) recipients of ICDs prior to 2000 when ICDs were implanted more for secondary than primary prevention.4 5 Notably, patients who have had their ICDs for longer are less receptive to deactivation, perhaps from an emotional attachment developed to their devices over time.12 Providers can use these patterns to know when to more strongly advocate for deactivation and prepare more persuasive language.
Limitations of this study are that it was a single centre and had a small sample size, but we feel that our results are generalisable to other services in our hospital as well as other hospital systems. The first half of the study also relied heavily on education, which is vulnerable to knowledge attrition over time. We mitigated this by introducing EMR changes to serve as a more durable way to sustain culture change within our institution (as evidenced by figure 2).
Future directions will be to spread this initiative to departments outside of medicine, non-MD staff and other hospital campuses within our hospital network. Recognition of the project has also spread internally to other units, prompting plans for additional education sessions and expansion of the improvement process across campus. Nurses have also joined the improvement effort to deliver reminders during nursing work rounds. Finally, this issue is not unique to admitted patients at our institution but even pervades hospice facilities, with only 10% of hospices nationally having an official ICD deactivation policy.13 Creating more ubiquitous hospice policies in our vicinity may rapidly expand our scope to improve this issue.
Conclusion
Shocks from ICDs should be avoided in patients who no longer desire them, especially at the end of life. Education of healthcare providers and the development of an ‘AICD deactivation planning’ support system in the EMR were effective ways to invite discussion regarding patients’ wishes on ICD therapy among DNR and comfort care patients. This also resulted in an increased number of ICDs being deactivated according to patients’ wishes. We hope to increase our scope to other departments and hospital campuses to spread awareness of this important issue.
References
Footnotes
DYC and MPW contributed equally.
Contributors DYC and MPW both contributed equally to this study. They were responsible for the design and execution of this study, writing of the study charter, submission of institutional review board exemption, creation and delivery of EMR and education sessions, data collection, data analysis, creation of figures, writing of the manuscript. BY was responsible for data collection and writing of parts of the manuscript. DPJ-K was responsible for statistical analysis after data completion. DCM was responsible for assisting the design of this study. DJC and JIL were principal investigators and were responsible for supervision and oversight of this project’s design and implementation and editing of this manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval According to institutional review board (IRB) policies at the authors' institution, this work met the criteria for quality improvement activities and was exempt from IRB review.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.