Article Text

Abstract
Corticosteroids are synthetic analogues of human hormones normally produced by the adrenal cortex. They have both glucocorticoid and mineralocorticoid properties. The glucocortoid components are anti-inflammatory, immunosuppressive, anti-proliferative and vasoconstrictive. They influence the metabolism of carbohydrate and protein, in addition to playing a key role in the body’s stress response. Mineralocorticoid’s main significance is in the balance of salt and water concentrations. Due to the combination of these effects, corticosteroids can cause many adverse effects. Oral corticosteroids are absorbed systemically and are therefore more likely to cause adverse effects than topical or inhaled corticosteroids. Furthermore, it is assumed that greater duration of treatment will lead to a greater number of adverse effects, and therefore the most at risk group are those taking high dose, long-term oral corticosteroids (LTOC). High dose is defined as a prescription of >5 mg oral prednisolone and long term as duration of treatment >1 month (based on National Institute for Health and Care Excellence guidance for patient’s ’at risk' of systemic side effects). Parameters to be monitored in primary care include weight, blood pressure, triglycerides, glucose and urea and electrolytes. From clinical experience within the general practice setting, the authors propose that these patients do not receive adequate baseline monitoring before starting corticosteroids nor are these markers monitored consistently thereafter. This project intended to evidence this claim, evaluate the adverse effect profile and improve monitoring in this patient group. The initial audit of 22 patients, within a single general practice, detected at least one documented adverse effect in 64% of patients, while 41% reported more than one adverse effect. 45% had recorded weight gain, 18% had recorded osteoporosis, 18% had at least one recorded cataract, 14% had recorded Hypertension, 14% had recorded diabetes mellitus, 9% had recorded dyspepsia and 5% had a recorded psychiatric complaint. All of these recorded conditions were either directly attributed to steroid medication or occurred since LTOC were prescribed.The aim of this project was to increase the percentage of patients on LTOC with complete baseline monitoring to 100%. ’Baseline monitoring' was defined as a measurement taken within the previous 5 years. Although somewhat arbitrary, 5 years was felt to be the maximum timeframe in which monitoring would still be relevant for comparison following introduction of LTOC. Quality improvement methodology was used throughout this project with multiple PDSA (Plan, Study, Do and Act) cycles. Through this, a monitoring system and protocol for patients taking LTOC was developed. As a result of this project, five adverse effects were detected in five different patients. These included two cases of secondary hypertension, one case of diabetes mellitus, one cataract and one case of adrenal insufficiency. 12 out of 20 patients achieved complete baseline monitoring. While this study did not fully achieve its aim, the aim was deliberately ambitious. As not all patients in this study attended for monitoring, a figure of 100% was impossible to achieve. The remaining ’incompletely monitored patients' had some but not all parameters measured. The creation of a staff protocol and increased clinical experience will ensure that complete monitoring takes place in the future. In conclusion, this project has shown that adverse effects from LTOC are prevalent in a single general practice population. It is also shown that monitoring for LTOC adverse effects is inadequate but can be improved relatively easily as skills and competencies from other medication monitoring systems already exist within healthcare settings and are immediately transferable.
- primary care
- healthcare quality improvement
- adverse events, epidemiology and detection
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Problem
From clinical experience within general practice, the authors propose that patients on long-term oral corticosteroids (LTOC) do not receive adequate baseline monitoring before starting these medications nor are these markers monitored consistently thereafter. This is a problem as corticosteroids are commonly prescribed and have many associated adverse effects some of which can be fatal. Adverse effects include but are not limited to weight gain, diabetes mellitus (DM), secondary hypertension, peptic ulcer(s)/gastric irritation, hypertriglyceridaemia, osteoporosis and cataract(s).1
In a general practice with a patient list of around 5000, 22 patients were noted to be prescribed LTOC. This was defined as a prescription of >5 mg oral prednisolone for >1 month (based on National Institute for Health and Care Excellence (NICE) guidance for patient’s ’at risk' of systemic side effects from oral corticosteroids).1 ’Baseline monitoring' was defined as a measurement taken within the previous 5 years, thus allowing for comparison following introduction and sustained use of corticosteroids.
This project aimed to increase the percentage of patients on LTOC with complete baseline monitoring to 100%.
Background
Corticosteroids can cause severe adverse effects through both mineralocorticoid and glucocorticoid activity. Mineralocorticoid properties may cause water retention and hypertension, while glucocorticoid properties may cause DM and osteoporosis.1 Consistent monitoring based on the NICE guidance may help reduce these harmful effects through early identification and treatment.
NICE recommends that blood pressure (BP, secondary hypertension), weight (Wt, gain), glucose (DM), triglycerides (TG, hypertriglyceridaemia) and glucose and urea and electrolytes (U&Es, adrenal insufficiency) are monitored regularly. In addition, patients should have their eyes tested yearly for cataract and have bone density monitored for osteoporosis.1
Few recent studies exist regarding the use, adverse effects and monitoring of corticosteroids in primary care. It also appears that none of these studies have been carried out in the UK.
One American observational study on asthma suggested that of 21 999 patients with asthma, in a primary care population, 12.5% of patients were prescribed LTOC in a near 10-year period. This study provides no data on adverse effects of LTOC but gives some indication on use of oral corticosteroids in primary care.2
A separate American retrospective cohort study also investigating LTOC in asthma found that patients who received four or more courses of oral corticosteroids had 1.29 times the odds risk of developing an adverse effect within the year compared with those who received between one and three prescriptions of oral corticosteroids. This study therefore suggests that the greater the duration of treatment with oral corticosteroids, the greater the risk of developing adverse effects.3
An American claims-based analysis into adverse effects of oral corticosteroids in giant cell arteritis found that in a patient population of 2497, who had at least one prescription of oral corticosteroids, 4472 adverse events were reported in a 10-year period.4 This equates to 1.79 adverse effects per patient in 10 years, a clear significant figure.4
A French epidemiology study aimed to assess general practitioners (GPs) perception of impact of corticosteroid adverse effects. It found that GPs significantly overestimated the impact of weight gain and significantly underestimated the impact of neuropsychiatric side effects in terms of patient’s concerns.5 This suggest although GPs may be aware of the adverse effects associated with corticosteroid use, they may not be placing enough significance on them.
An Australian cost-effectiveness study into LTOC in severe asthma estimated that the costs associated with adverse effects were $598.32 per patient per year.6 This indicates that adverse effects in LTOC use are of major clinical significance and have major financial implications.
Baseline measurement
In a general practice with a patient list of around 5000, 22 patients were noted to be on LTOC. This was defined and searched for as prescriptions of >5 mg oral prednisolone for >1 month (based on the NICE guidance for patient’s ’at risk' of systemic side effects from oral corticosteroids).1
’Baseline monitoring' was defined as a measurement taken within the previous 5 years. Although somewhat arbitrary, 5 years was felt to be the maximum timeframe in which monitoring would still be relevant for comparison following introduction of LTOC ’complete baseline monitoring' was defined as the measurement of all parameters as recommended by NICE (Wt, BP, glucose, TG, U&Es) within the previous 5 years.
Initial baseline measurements showed poor monitoring in patients taking LTOC. Only 18% had complete baseline monitoring.
Statistics regarding the adverse effects recorded in the patients' GP notes was also startling. Sixty-four per cent of patients taking LTOC had at least one recorded adverse effect, with 41% of patient with more than one recorded adverse effect. Forty-five per cent had recorded weight gain, 18% had recorded osteoporosis, 18% had at least one recorded cataract, 14% had recorded Hypertension, 14% had recorded DM, 9% had recorded dyspepsia and 5% had a recorded psychiatric complaint. All of these recorded conditions were either directly attributed to steroid medication or occurred since LTOC were prescribed.
All 22 patients were tagged in their GP patient record with the read code: prolonged corticosteroid therapy. This was done manually with new data entered on each patient’s record.
The outcome measure will be complete baseline monitoring defined as having all parameters as recommended by NICE (Wt, BP, glucose, TG and U&Es) recorded within the last 5 years.
Process measures
Staff will answer questionnaires regarding the monitoring of LTOC, to assess clinical knowledge this will be reassessed 4 months later.
Patients' GP record data will be analysed at 2 monthly intervals to identify any monitoring undertaken.
Balancing measure
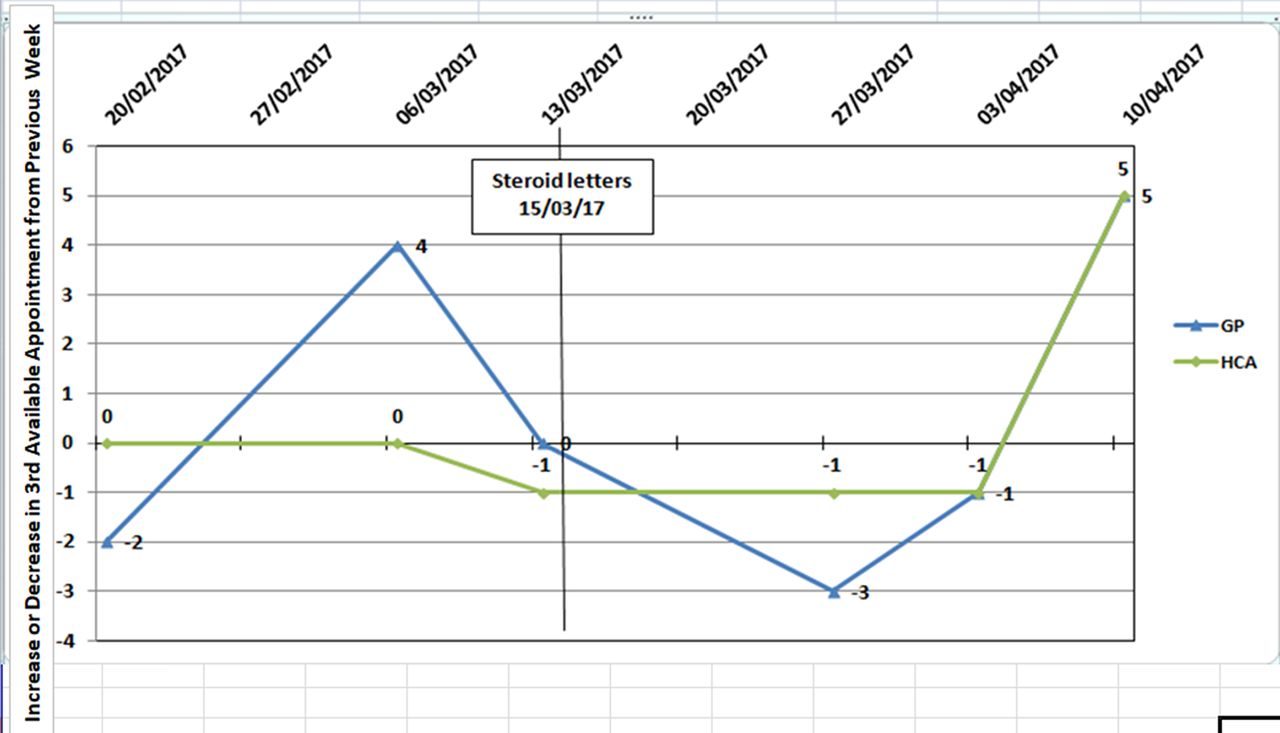
Availability of GP and healthcare assistant (HCA) appointments will be measured weekly as ’the number of working days until the third available appointment'. This is data already collected within the practice and is proven to be an accurate measure of availability of appointments.7
Design
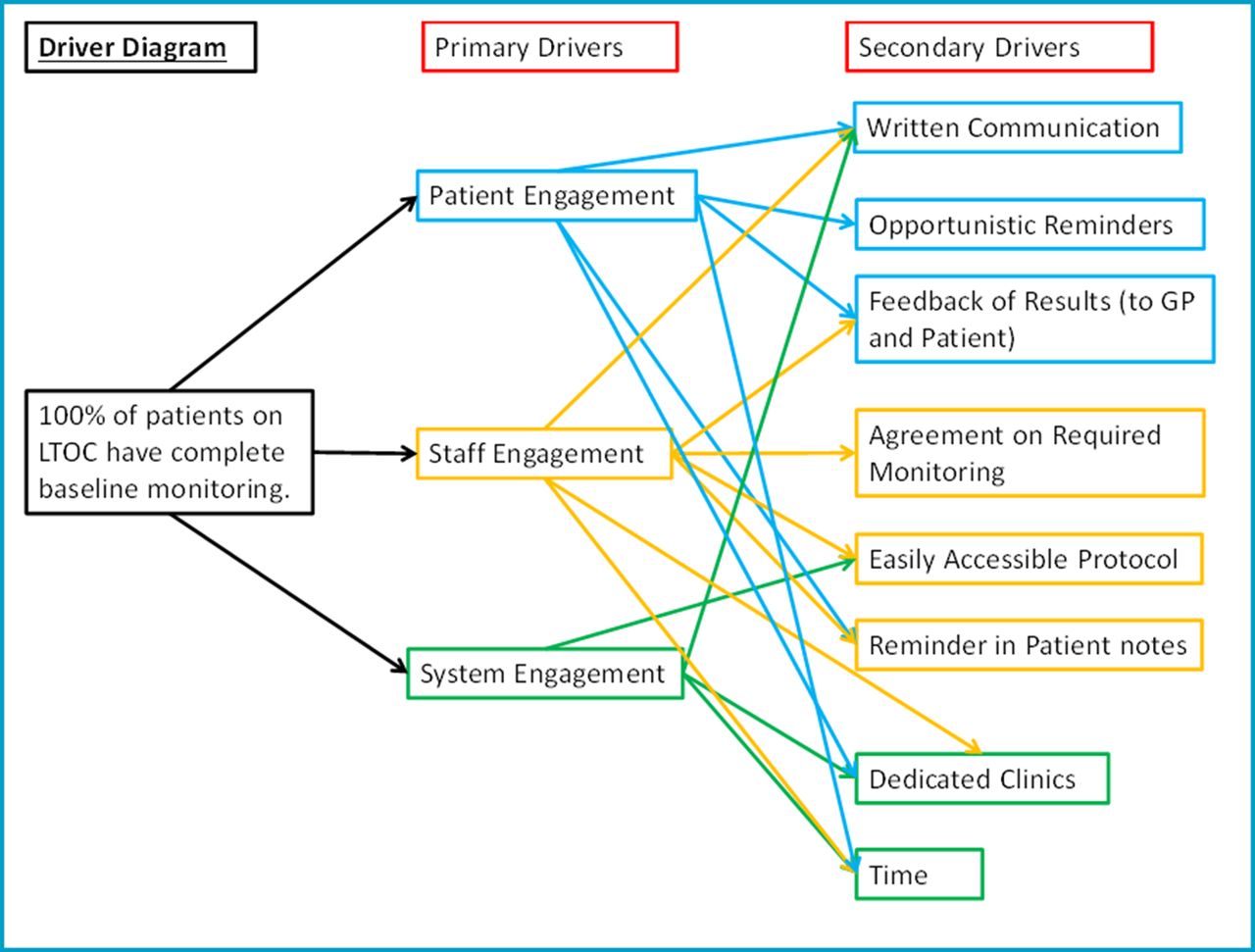
Once presented with the results of the audit and analysis of the process flow (figures 1 and 2), the practice team decided it was appropriate to take action and improve monitoring. The subject was discussed at three practice meetings. This involved the key stakeholders with GPs, practice nurses and HCAs at one meeting; the practice manager and other administrative staff at another; and finally one meeting with reception staff.

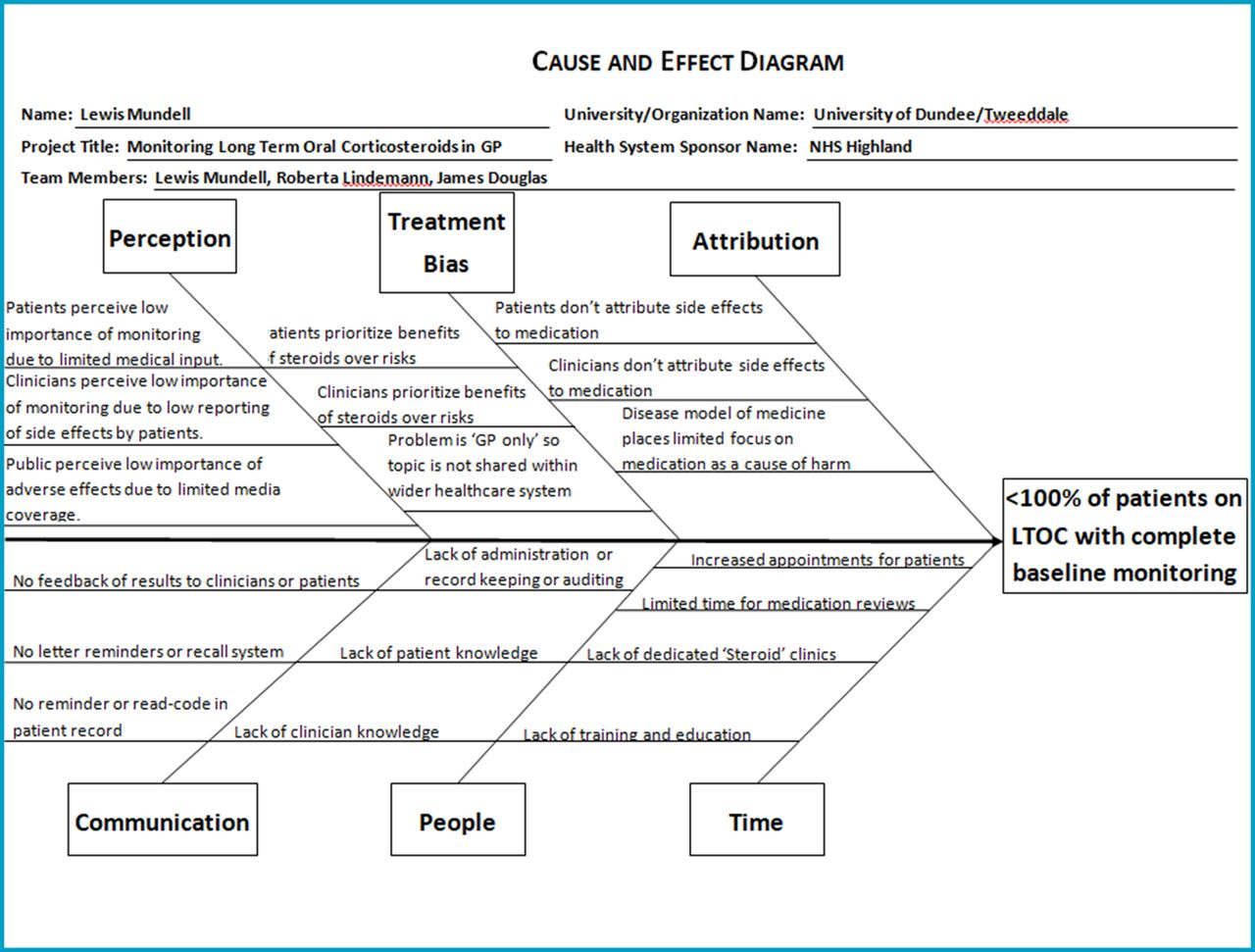
Cause and effect diagram. GP, general practitioner; LTOC, long-term oral corticosteroids.
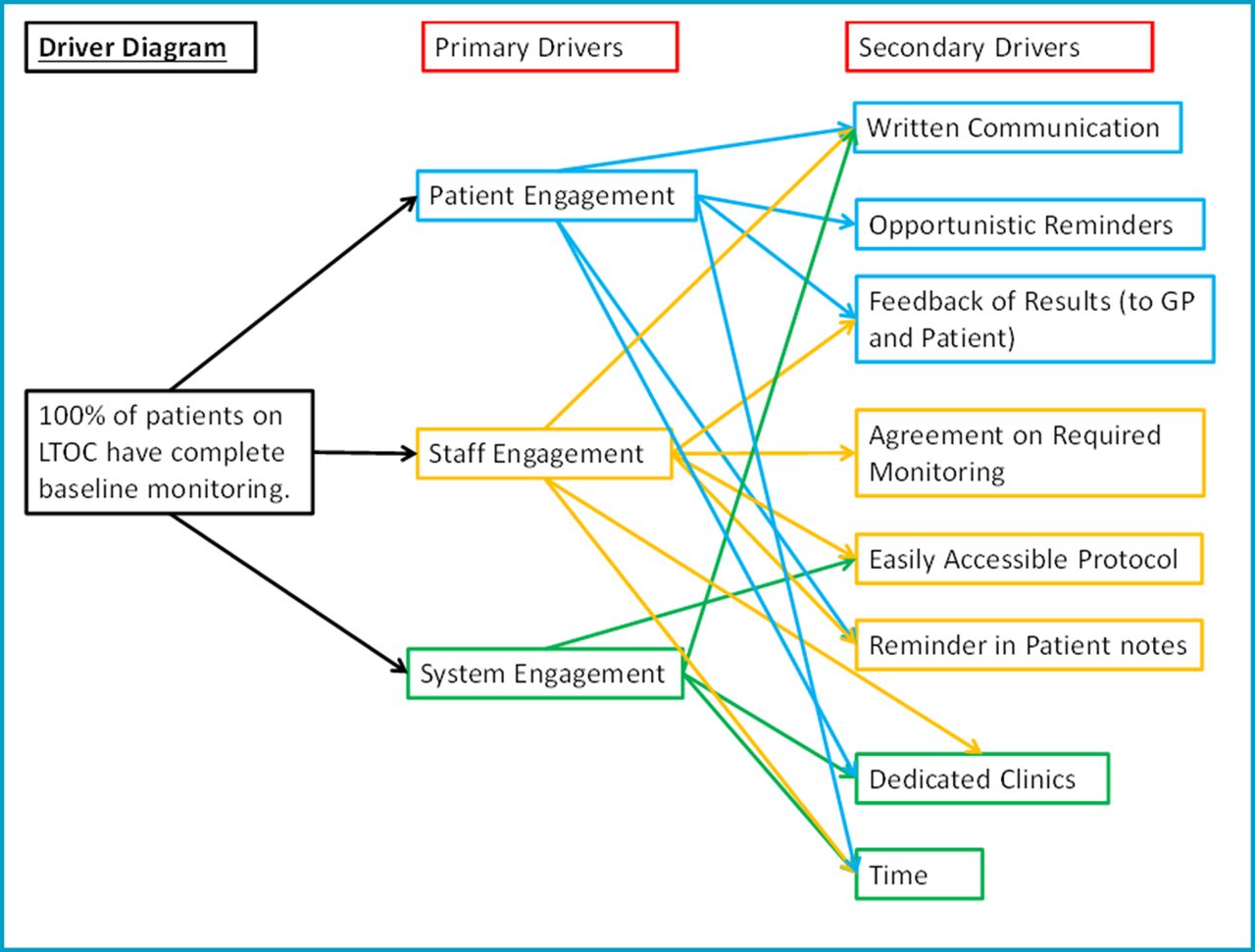
Driver diagram. GP, general practitioner; LTOC, long-term oral corticosteroids.
It was decided that a protocol for monitoring steroids needed to be created for use with new patients but that a ’catch-up' process was also required to monitor those already taking oral corticosteroids.
A process of steroid reviews was agreed with patients seeing an HCA to have their blood taken and a review appointment with a GP 1 week later to discuss results. It was thought the best way to inform and encourage patients to attend these appointments was through letters asking patients to phone up to book an appointment. This proved an appropriate and effective method and is used for monitoring other medications so is within competencies of staff and the system.
Queries were regarding workload, and the requirement of DEXA bone scanning was raised by GPs. It was agreed that increased workload would very likely result but that the GPs had a duty of care to monitor LTOC as they had prescribed these medications. DEXA bone scanning was deemed surplus to requirements as it would not change management.8
Strategy
This quality improvement project aimed to increase the percentage of patients on LTOC with completed baseline monitoring to 100%. A quality improvement methodology using PDSA cycles as set out by the Institute for Healthcare Improvement.9
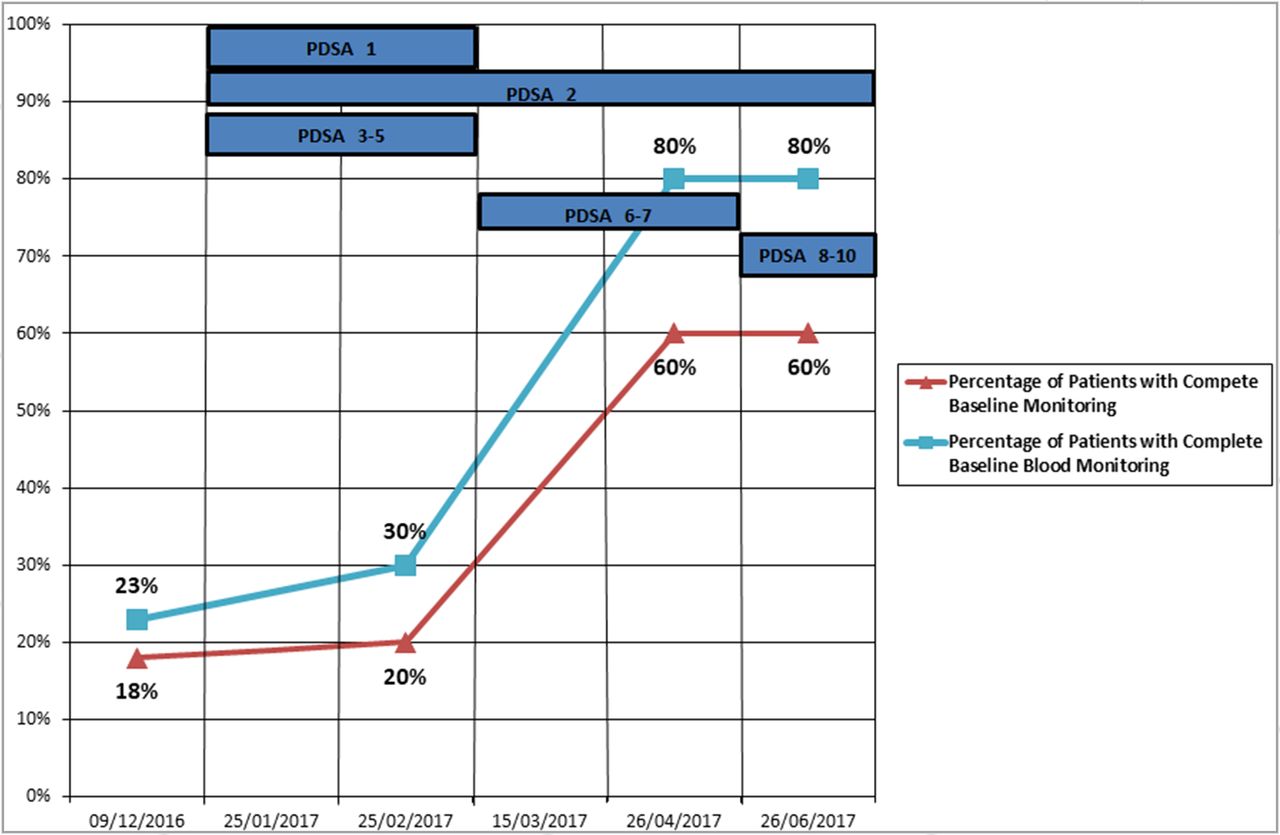
PDSA 1 (practice meeting): The initial intervention was to hold a practice meeting to inform the practice clinicians of the problem of steroid monitoring within the practice and work as a team to solve it. It was thought that after this meeting there may be a small increase in monitoring within the patient population, due to increase clinician awareness but that progress towards the project aim would be small. The study lost two participants at this point due to death, the number of patients in the study was now 20. Objectively, as expected, after the clinical meeting complete baseline monitoring of patients on LTOC increased very slightly from 18% to 20%. However, when looking at monitoring in general (measured as altered monitoring data in patients' records in the previous 2 months), this increased from 36% to 55%. It is thought that this was due to increased awareness of the need to monitor LTOCs. Although this increase in monitoring was positive, it was not the full or correct monitoring that is, not all parameters were measured. Further change was then focused on the system in the hope of yielding more significant improvement (figure 3).
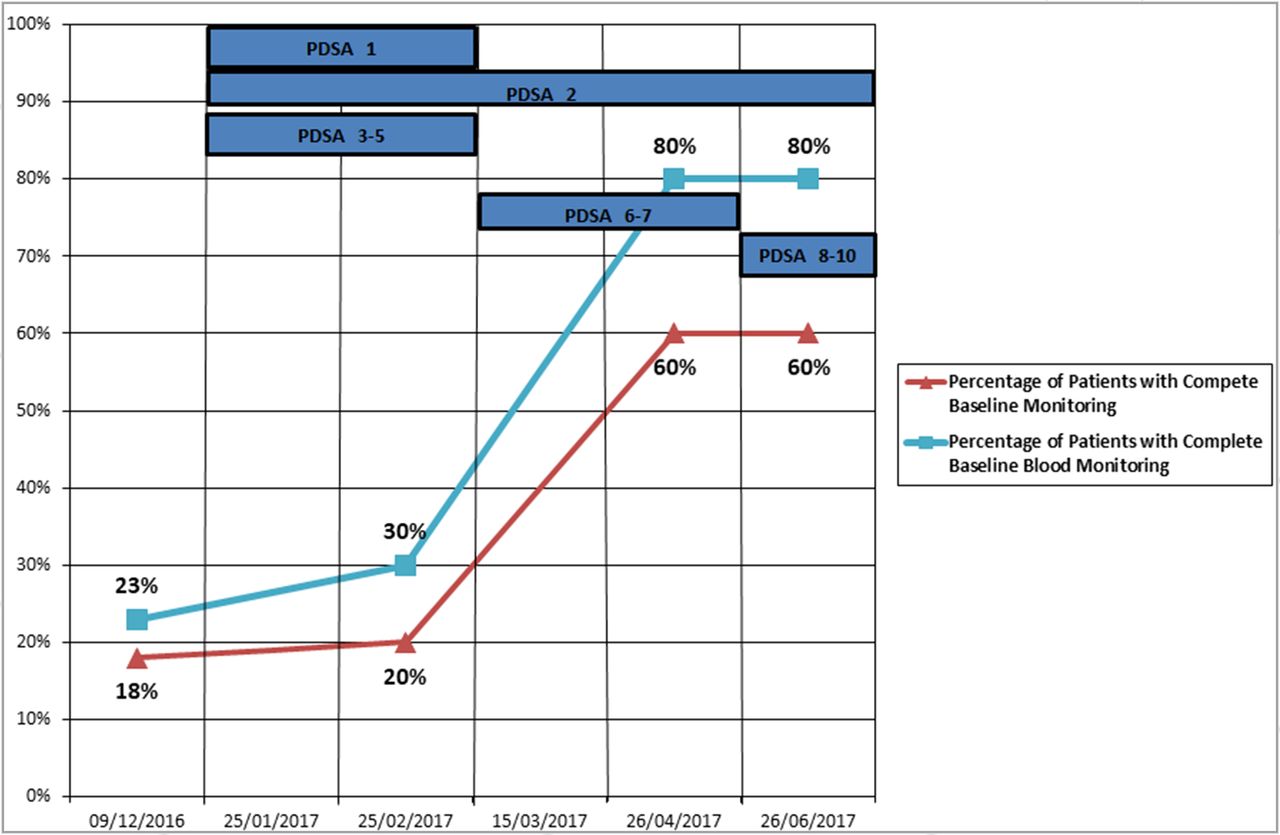
Baseline monitoring of long-term oral corticosteroids.
PDSA 2 (questionnaire): The second intervention was in the form of a questionnaire. Clinical staff were asked to answer questions regarding their knowledge of monitoring required for corticosteroids. This would assess the healthcare professionals' knowledge of the subject but also assess their retention as it would be retested at a later date. It was thought knowledge would increase over time due to awareness and participation in this project. Initially, knowledge regarding LTOC monitoring among clinical staff (GPs, nurses and HCAs) was mixed. 37.5% of staff were able to identify four of the five components that should be monitored (BP, Wt, U&Es, TG, glucose).
37.5% of staff identified three components, while 25% of staff identified just two. The questionnaire was repeated 4 months after the initial clinical meeting. A slight alteration was made to the original question, changing from ’What should we monitor in people taking long-term high dose steroids?' to ’What should we monitor (within the GP setting) in people taking long-term high dose steroids?'. It was hoped this would add clarity to the question. Knowledge was found to be at a similar level 4 months later. Twenty-eight per cent identified two components of LTOC monitoring, 28% identified three components and 42% identified four components. This suggests that staff knowledge at 4 months regarding monitoring of LTOC is largely unaltered by having a clinical meeting in itself as well as carrying out a QI project. Ideally, the same healthcare professionals would have been surveyed in the follow-up questionnaire; however, this was challenging from a practical point of view without allowing preparatory ’study'. Retention would likely have been improved had staff received training on LTOC. This did not occur to organisational difficulties and time constraints but would definitely have been of significant value.
PDSA 3 (steroid protocol): As a team, the practice decided that there was need for a protocol to be created for patients starting on LTOC. This would contain accurate medical guidance but also practical steps relevant within the setting of general practice. This was then created based on the NICE guidelines and shared with one GP. It was then circulated to the practice team electronically. The first GP provided critical feedback; however, feedback from the wider team was limited, from only one other GP. A key discussion point on the protocol focused on the need for bone monitoring patients on LTOC. Reviewing NICE guidance on osteoporosis, it cites Scottish Intercollegiate Guidelines Network (SIGN) guideline 142 (Management of Osteoporosis and the Prevention of Fragility Fractures) which suggest people on LTOC should be on bone protection medications due to the high risk of fractures associated with corticosteroid medication.10 Therefore, it was decided that patients did not need bone scanning as long as they were taking bone protection medications. If done again, it may have been more advantageous to share the new protocol in person at a practice meeting as this may have yielded greater feedback from a larger and more diverse group of stakeholders. As part further research, there would be value in assessing compliance to this new protocol.
PDSA 4 (patient information leaflet): As part of creating a staff protocol for the use of LTOC, it was suggested that this should include a patient information leaflet. Before creating a new leaflet, it was sensible to identify any pre-existing leaflets that may already exist. One such leaflet was available from the web-based ’patient', commonly used by the practice for patient information leaflets. A further advantage is that these leaflets (from ’patient') are already embedded within the patient record system, thus allowing easy access for clinicians. The information leaflet was reviewed with one GP and was approved for use within the staff protocol. In hindsight, it may have been more thorough to share the patient information leaflet with other members of the healthcare team. Creating a unique, to the practice, patient information leaflet may have produced a higher quality of leaflet but again time was restrictive due to other clinical work undertaken by the authors.
PDSA 5 (drafting a patient letter): A letter was chosen as the most appropriate method to invite a patient to attend for blood tests followed by a GP appointment 1 week later to review their results. A letter must include relevant information and be approved by both clinical and administrative staff. The letter was drafted using a patient letter template from within the practice. It was first discussed with a GP who approved it and then shared in person at an admin team meeting. Thankfully, at this point it was noted that the letter did not include the requirement to fast before the blood tests—vital for the accuracy of TG measurement. If repeated it would be wise to review the blood testing requirements prior to drafting the letter.
PDSA 6 (sending letters): Letters were sent to patients asking them to attend for blood tests followed by a review with a GP of their results. The question: ’Does providing patients with written communication increase LTOC monitoring within the practice?' It was hypothesised that the letters would greatly increase monitoring. This was the case with complete baseline monitoring increasing from 20% to 60%. Twenty per cent received incomplete monitoring due to absent BP and/or Wt measurements. On the other hand, 20% of patients did not attend for monitoring. The letter was updated to inform patients that their Wt and BP should be checked. If this project was repeated, it would sensible to have sent the letters to a small sample of the patients within the study. This may have allowed the letter to be improved earlier. It is also noted that despite a protocol for new patients starting LTOC being created, no protocol for the HCA-led clinic itself existed. This will likely have contributed to lower complete baseline monitoring (figure 3).
PDSA 7 (GP review): 80% of patients attended for blood tests following a letter. The letter also instructed them that they were to have review with a GP with the results. The question: ’Does written communication increase steroid reviews among patients on LTOC?' 70% of all patients on LTOC had review of their LTOC treatment with a GP following the steroid letter. Twenty per cent of patients did not have a review of blood results with a GP and 10% of patients did not attend for blood tests or a GP review following the steroid letter. Within the 70% who attended for GP review, 20% had not had a previous review of their LTOC since the start of the project (4 months). In hindsight, it may have been pertinent to ensure that both an appointment with the GP and HCA were booked at the same time. This is the process now. Some patients may have only expected to have a review with a GP if blood tests were abnormal (figure 4).

Percentage of patients attending for GP steroid review following steroid letter. GP, general practitioner; LTOC, long-term oral corticosteroids.
PDSA 8 (’pop-up' reminders): Following lower than anticipated Wt and BP monitoring, it was discussed within the team the value of adding a ’pop-up' message to patient records. This would remind the attending clinician that the patient was due to have these parameters measured. However, it was decided that this would be ineffective. Many patients have such ’pop-ups' and thoughts among GPs that they are mostly ignored. Therefore, it is assumed that using ’pop-up' messages would not yield greater monitoring. Further quality improvement projects could study the value of these ’pop-ups'.
PDSA 9 (clinic protocol): In evaluation of the project, qualitative research was carried out to gain the views of the HCAs involved in monitoring. Overall reaction to the project was positive with HCAs feeling appointments were ’as normal'. However, staff suggested that a ’clinic flow diagram' would be useful so that ’every knows what they are doing’ and that ‘everybody is doing the same thing’. It was also advocated that appointment times would need to be doubled in order to carry out Wt and BP measurements with HCAs noting ’difficulty bleeding fasting patients' and that ’anomalies [in BP] may occur due to "busy-ness" [of the clinic]'. A draft clinical was shared and approved by HCAs and is now in use. In hindsight, this would have been a valuable exercise to carry out at the start of the project.
PDSA 10 (sustainability): Also as part of evaluation qualitative research was undertaken with the practice manager. The hope of this was to achieve a sustainable model for the future in terms of monitoring patients on LTOC. It was identified that no recall system existed to identify these patients again and thus monitor them. To counteract this, an audit has been placed in the ’audit calendar' and will now take place annually. This audit will identify patients tagged with the read code ’prolonged corticosteroid therapy' and patients without a read code who have been prescribed >5 mg of oral prednisolone for >1 month. This was deemed sustainable as it was ’similar to other medication monitoring' and ’within existing competencies and systems'. Again, in hindsight, it would have been beneficial to set up this project in the ’audit calendar' at the start of the project.
Results
Data variation
Two patients were withdrawn after the first data collection due to their death, reducing the number of patients in the study to 20.
Third next available appointment data were not collected every week. It was however collected for the majority of weeks for the duration of the project. As these data are normally only collected for management meetings, if the management meeting did not take place or was cancelled the data were not collected. Ideally these data should have been collected weekly regardless of meeting schedules.
This initial staff questionnaire surveyed eight healthcare professionals, while the second, follow-up, questionnaire surveyed only seven. This was due to practical difficulties of collecting data from eight healthcare professionals at the same time.
Data collection
Data were collected through a series clinical audits of patient’s GP records.
Results
Clinical meetings appeared to increase monitoring generally, with a percentage change in altered monitoring data of 19% compared with the previous 2 months but only achieved an absolute increase of 2% in complete baseline monitoring. Sending letters to patients asking them to attend for monitoring proved far more effective, increasing complete baseline monitoring by a further 40% to 60% and this was greatest for baseline blood monitoring which increased by 50% (figure 3).
From the monitoring undertaken during this study, in a patient population of 20, the following new diagnosis were given: one diagnosis of DM, two diagnoses of essential hypertension, one diagnosis of cataract and one diagnosis of adrenal suppression. This translates to 15% of all patients on LTOC within a single general practice setting, developing at least one newly identified adverse effect within the timescale of this quality improvement (QI) project.
Qualitative research
This was collected from staff within the GP practice (GP, the practice manager and HCAs). Feedback in response to this project was very positive. There was constructive suggestions both for improvement and sustainability across the multidisciplinary team. This has helped the project be a success overall.
Balancing measures
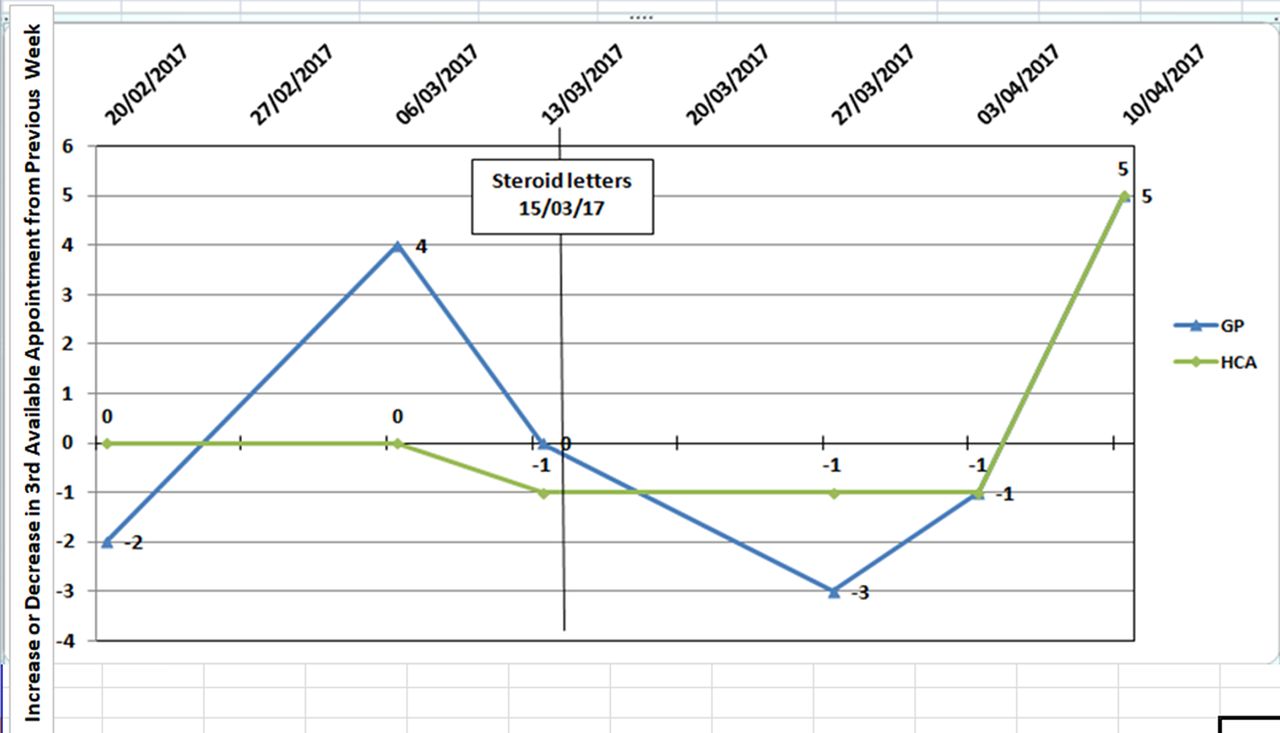
Available third next available appointment data suggested no tangible impact of this project on the availability either GP or HCA appointments (figure 5).
Sharing of results
Results were shared electronically throughout the project with the practice team to highlight improvement and promote engagement.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Increase or decrease in third available appointment from the previous week.
Lessons and limitations
Learning
In this quality improvement, the full aim—'100% of patients on LTOC with complete baseline monitoring'—was not achieved. The figure reached was 60%. However, this does not tell the full story. Based on patients who attended the practice for monitoring, the maximal achievable aim was 80%. Therefore, there are two key areas of learning: ’patient attendance' and ’monitoring completeness'. Realistically, in terms of ’patient attendance', further intervention would need to be more invasive and likely to be more time consuming for staff. One such intervention could be calling patients to ask them to attend.
It is important to ensure that for those who do attend that monitoring is complete. In this project, 20% of patients did not achieve this due to absent weight and/or blood pressure measurement(s). With reflection, this could have been done within HCA appointments but it is imperative that there is enough time (ie, double appointments) and a recognised protocol to follow.
Cost analysis demonstrated the total cost of the project to be £912. This includes staff patient time, administration time, staff planning time, administrative equipment and an approximation of the cost of blood tests. This cost breaks down to £45 per patient in the study. This figure can be compared with the adverse effect identification rate due to this monitoring which was 15%. This included two cases of secondary hypertension, one case of DM, one cataract and one case of adrenal suppression. It is not unreasonable to assume that costs relating to complications from the adverse effects identified would amount to far greater than £912.
This study has a high level of ’generalisability'. As the project took place in a ’standard' general practice, the methodology used should be transferable to other general practices. Furthermore, as identified by practice staff, monitoring systems exist for other drugs and therefore competencies required to undertake LTOC monitoring also exist.
Finally, the lead author of this project was a fourth-year medical student on a Longitudinal Integrated Clerkship (LIC). In practical terms, this LIC based the student in a general practice for an entire year with 60% of time spent with primary care and 40% with secondary care. An LIC is therefore an ideal base for quality improvement work. It allows a student to take the lead on a project within a small setting with ample support and unlike conventional medical education models the student remains in a single place and therefore can complete a project of significant duration.
Limitations
The major limitation of this project was small numbers. At the beginning of the study, only 22 patients were identified as being on LTOC. During the study, this number dropped to 20 due to patient death. These small numbers limit the scientific significance of the results. However, they do not limit the clinical significance. If possible, future research should include more patients, likely from multiple GP practices to provide greater scientific significance. It is also worth noting that some of these patients are managed in secondary care and therefore, some monitoring data may be recorded on hospital-based systems/records but not within the practice. This has the potential to produce some false-negative results.
Linked to a poor scientific significance in this study are the few points of data collection. On face value, it would seem wise to have recorded data more frequently and if time was unlimited, the study would have done so. However, with such a small pool of patients, collecting data more frequently would be onerous and likely week-to-week figures would not display significant change nor add quality to measurement of interventions. Again, further research with a higher number of patients would facilitate increased monitoring and thus achieve greater clinical and scientific significance.
It is also noted that this project did not determine when ‘baseline monitoring’ first took place for individual patients. This time specific data may have added clarity to the monitoring process undertaken prior to this project but this monitoring was deemed too irregular to be included.
One further limitation, related to small numbers, was the decision not to include patients taking four or more courses of oral corticosteroids in 1 year, for example, patients with regular exacerbation of asthma or chronic obstructive pulmonary disease. NICE identifies this group as high risk of developing adverse effects due to corticosteriod use[1]. These patients were not part of this study again due to time pressures but also as they were considered to be a clinical subset. Future research, specifically into adverse effects experienced and monitoring, within this subgroup would be extremely valuable. It may also be of value to research the incidence of adverse events of inhaled corticosteroids.
Further PDSA cycles would also have been of value particularly for the created protocols and for staff education. This would help refine the use of the protocols and improve staff training.
Conclusion
In the literature, there is very little research into the long-term impact of oral corticosteroids use. Evidence regarding the frequency of adverse effects and monitoring to identify and treat these adverse effects is scarce. This statement is particularly true in the setting of general practice, where it appears that virtually no research into this topic is published despite the majority of LTOC prescriptions passing through a GP.
The aim of this project was to increase the percentage of patients on LTOC with complete baseline monitoring to 100%. This aim was not met. A figure of 60% was reached. If this figure was maximised, by ensuring that all patients who attended following a request had complete monitoring undertaken on their visit, the figure would be 80%. This is the maximum realistic attainable percentage as it not all patients will attend for monitoring on request. If a group of patients remain ’unmonitored', this should prompt questions on the continued prescription of LTOC in this group. For those patients who did attend for monitoring but were ’incompletely monitored', the fault lies with the system. With the introduction of protocol and further clinical experience in monitoring LTOC will ensure that these patients are ’completely' monitored in the future.
This project could be replicated quite straightforwardly within a single GP setting. The competences and skills required exist within most GP practices, and therefore there is limited need for training and supervision in terms of monitoring. Financially, it is projected that the total cost of this project was £911.21 equating to £45.56 per patient in the study. This would appear to be cost-effective with an adverse effect detected objectively in 15% of all patients taking LTOC.
This project is sustainable, again through processes that already exist within the GP setting. An audit calendar is used to annually to monitor other drug and diagnosis monitoring. LTOC have been added to this group allowing monitoring to be systemised.
Further, more scientifically significant, research in this field would be challenging. Due to organisational structure, it would be difficult to study a larger patient group across multiple GP sites. However, this would be extremely worthwhile adding significance to this project’s findings but also further emphasising the need for LTOC monitoring.
Expansion of the knowledge base is also required among patients taking high-dose corticosteroids frequently throughout the year. The most abundant group of these would be patients with asthma. Analysis of adverse effects in these patients would provide help to define the impact high-dose oral corticosteroids have on patient’s taking them frequently throughout the year. It would also provide insight into the need for corticosteroid monitoring within this group. It may also be of value to assess the side effect profile of long-term inhaled corticosteroids.
Acknowledgments
All staff at Tweeddale Medical Practice
Footnotes
Contributors LM: lead author. RL: co-author and clinical advisor. JD: clinical mentor/superviser.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.